
記住我
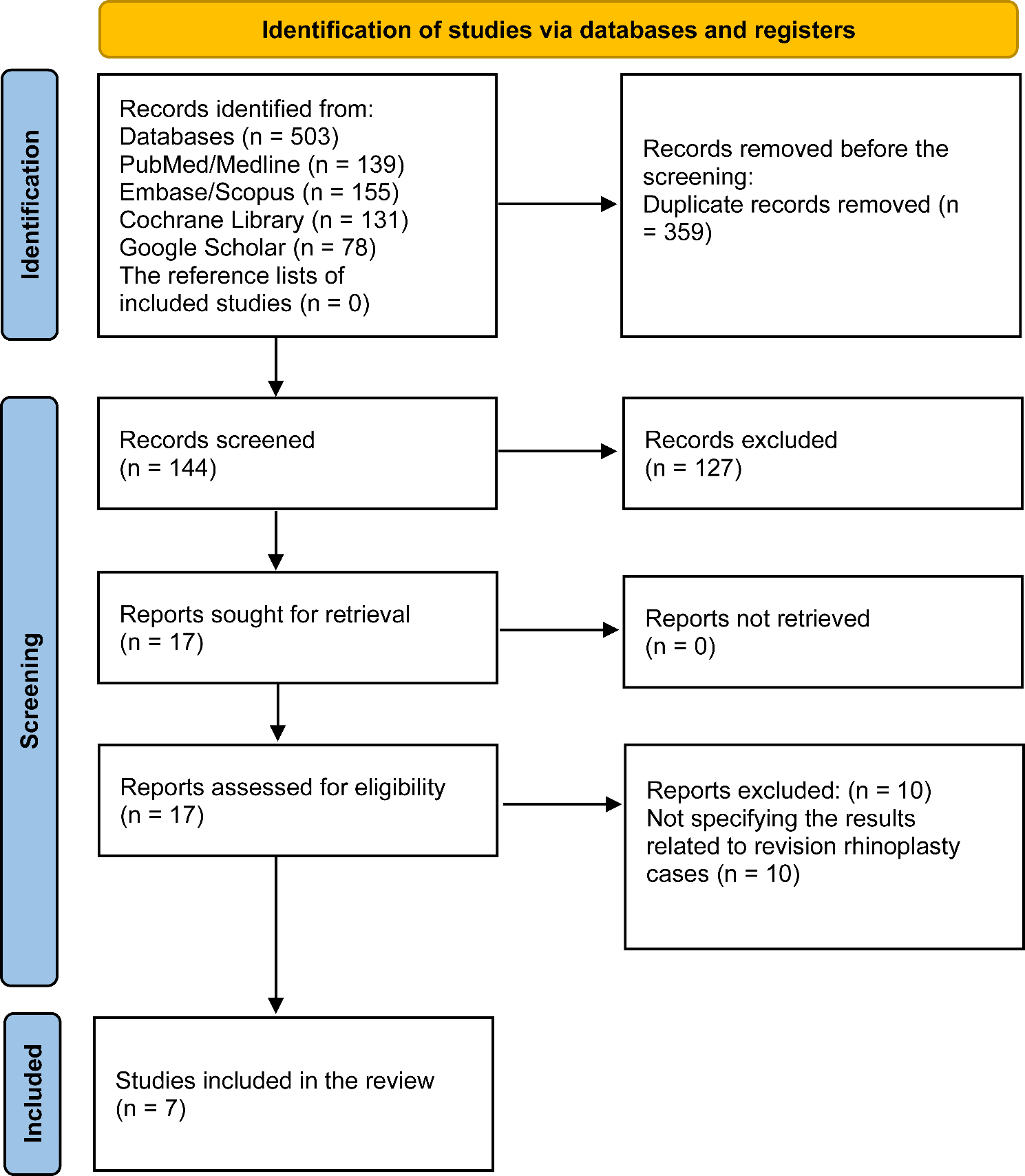

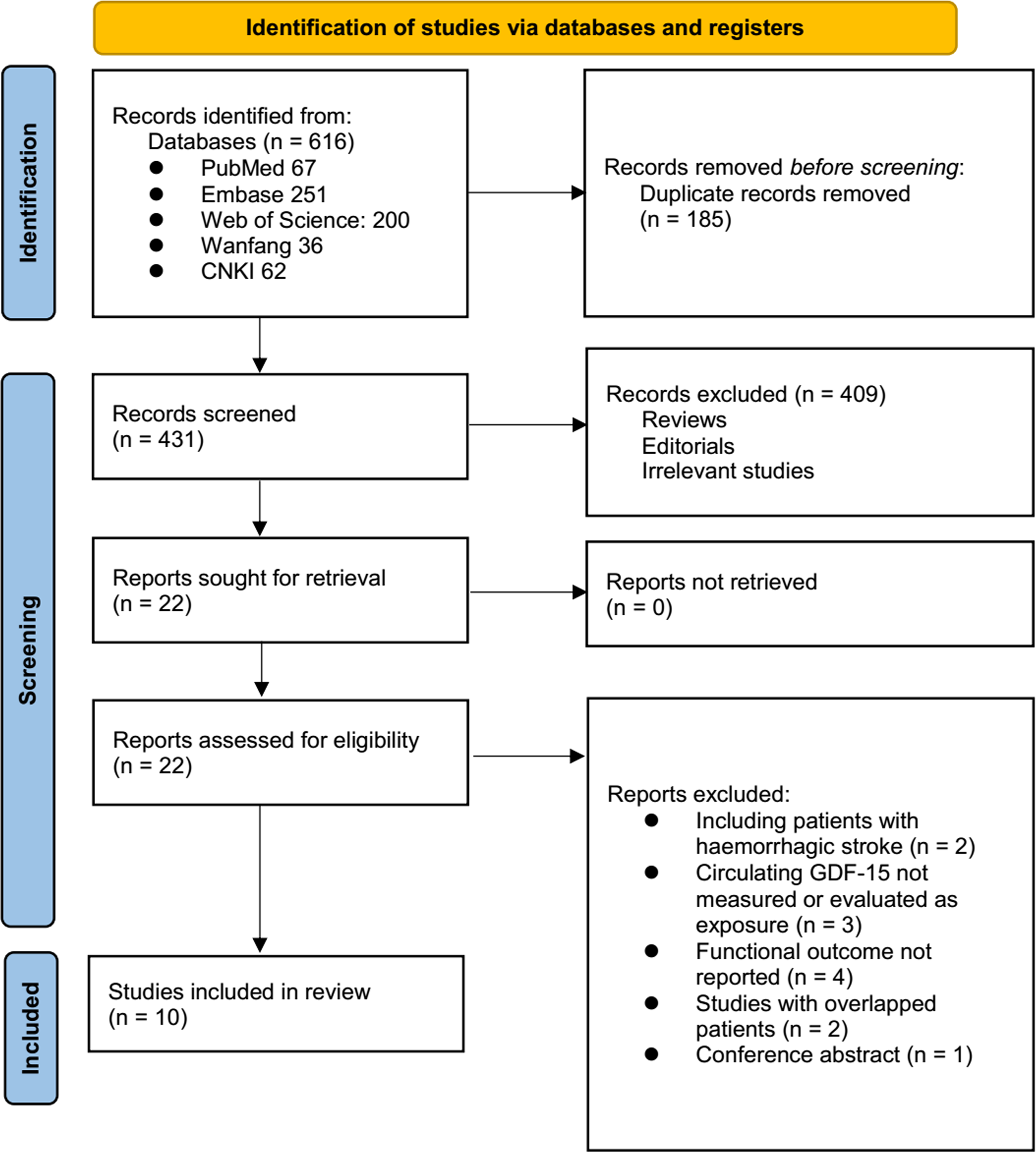





The study inclusion process is illustrated in Fig. 1. In summary, an initial search of five databases yielded 616 potentially relevant records, of which 185 were excluded due to duplication. The titles and abstracts of the remaining records were then screened, leading to the exclusion of 409 studies, primarily because they did not align with the objectives of the meta-analysis. The full texts of the remaining 22 records were reviewed by two independent authors, resulting in the exclusion of 12 studies for reasons detailed in Fig. 1. Ultimately, ten studies [14,15,16,17,18,19,20,21,22,23] were deemed appropriate for inclusion in the quantitative analyses.
Fig. 1
PRISMA flowchart of study identification
Summary of study characteristicsTable 1 presents the overview of the characteristics of the included studies. Overall, four prospective cohort studies [14, 15, 18, 19], five retrospective cohort studies [16, 17, 21,22,23], and one post-hoc analysis of clinical study [20] were included in the meta-analysis. These studies were reported from 2011 to 2022 and performed in Germany, China, France, and Korea. Overall, 4231 patients with AIS were included, with mean ages varying from 58.4 to 74.6 years, and the proportion of men ranging from 39.0 to 64.1%. The circulating level of GDF-15 was measured all within 24 h after stroke onset, with enzyme-linked immunosorbent assay in seven of the included studies [17,18,19,20,21,22,23]. For the other three studies [14,15,16], other methods such as immunoradiometric assay, electrochemiluminescence immunoassay, and radioimmunoassay were used, respectively. The cutoff values for defining a high circulating GDF-15 level were derived via receiver operating characteristic (ROC) curve analysis in three studies [14, 21, 23], via median of GDF-15 in five studies [15,16,17, 19, 22], via the third tertile [18] and the upper limits of healthy individual [20] in the another two studies. The cutoff values for defining a high GDF-15 varying from 493 to 2088 ng/L. The patients were all followed for 3 months among the included studies. The risk of poor functional outcome at 3 months after stroke were reported in all of the included studies, which were defined as the mRS ≥ 2 in four studies [14,15,16,17] and ≥ 3 in six studies [18,19,20,21,22,23]. Accordingly, 1267 (29.9%) of the included patients had poor functional outcome 3 months after AIS. A multivariate analysis was performed in five studies when the association between circulating GDF-15 and poor functional outcome after AIS was evaluated [14, 15, 19, 20, 22], whereas a univariate analysis was performed in another five studies [16,17,18, 21, 23]. The NOS of the included studies were six to nine stars, suggesting overall moderate to good study quality (Table 2).
Table 1 Characteristics of the included studiesTable 2 Study quality evaluation via the Newcastle-Ottawa ScaleResults of the meta-analysis and sensitivity analysisThe pooled results of ten studies using a random-effects model suggested that compared to AIS patients with a low circulating GDF-15 at admission, patients with a high circulating GDF-15 were associated with an increased risk of poor functional outcome at 3 months (OR: 2.60, 95% CI: 1.95 to 3.46, p < 0.001; Fig. 2A) with moderate statistical heterogeneity (I2 = 65%). Further analysis excluding one study at a time consistently demonstrated similar results (OR: 2.38 to 2.84, all p < 0.05).
Fig. 2
Forest plots for the meta-analysis of the association between circulating GDF-15 level at admission and functional outcome after AIS; A, overall meta-analysis; B, subgroup analysis according to study country; and C, subgroup analysis according to study design
Results of subgroup analyses and meta-regression analysesFurther subgroup analyses showed similar results in studies from Asia and Europe (OR: 2.94 versus 1.99, p for subgroup difference = 0.18; Fig. 2B), in prospective and retrospective studies (OR: 2.23 versus 2.89, p for subgroup difference = 0.39; Fig. 2C), in studies with the mean age of the patients < and ≥ 65 years (OR: 3.16 versus 2.14, p for subgroup difference = 0.22; Fig. 3A), in studies with the proportion of men < and ≥ 60% (OR: 2.52 versus 2.79, p for subgroup difference = 0.76; Fig. 3B), and in studies with the cutoff of GDF-15 defined by ROC analysis and the medians (OR: 3.80 versus 2.25, p for subgroup difference = 0.07; Fig. 4A). Interestingly, the subgroup analysis suggested that the association between a high circulating GDF-15 and the risk of poor functional outcome after AIS was stronger for studies with cutoff of GDF-15 < 1200 ng/L as compared to those ≥ 1200 ng/L (OR: 3.52 versus 1.90, p for subgroup difference = 0.003; Fig. 4B), which substantially explained the source of heterogeneity. In addition, a stronger association was observed in studies with poor functional outcome define as mRS ≥ 3 compared to those as mRS ≥ 2 (OR: 3.17 versus 1.85, p for subgroup difference = 0.04; Fig. 5A). Subsequently, consistent results were obtained for studies with univariate and multivariate analysis (OR: 3.03 versus 2.34, p for subgroup difference = 0.33; Fig. 5B). Finally, the univariate meta-regression analyses did not show that study characteristics such as publication year, sample size, mean age of the patients, proportion of men, cutoff value of GDF-15, cutoff mRS for defining a poor functional outcome, or the study quality score in NOS could significantly affect the association between circulating GDF-15 at admission and the risk of poor functional outcome after AIS (p all > 0.05; Table 3). However, publication year and NOS scores have relatively higher adjusted R2 (27.4% and 28.3%, respectively), indicating they may explain more of the between-study heterogeneity compared to other factors. These findings should be interpreted cautiously, acknowledging the lack of statistical significance.
Fig. 3
Forest plots for the subgroup analysis of the association between circulating GDF-15 level at admission and functional outcome after AIS; A, subgroup analysis according to the mean age of the patients; and B, subgroup analysis according to the proportion of men
Fig. 4
Forest plots for the subgroup analysis of the association between circulating GDF-15 level at admission and functional outcome after AIS; A, subgroup analysis according to the methods for defining the cutoff of GDF-15; and B, subgroup analysis according to the cutoff values for defining a high circulating GDF-15 level
Fig. 5
Forest plots for the subgroup analyses of the association between circulating GDF-15 level at admission and functional outcome after AIS; A, subgroup analysis according to the definition of poor functional outcome; and B, subgroup analysis according to the analytic models (univariate or multivariate)
Table 3 Results of univariate meta-regression analysisPublication biasVisual inspection of the funnel plots for the meta-analysis examining the relationship between circulating GDF-15 levels and poor functional outcomes after AIS indicates symmetry, suggesting a low risk of publication bias (Fig. 6). This observation is further supported by Egger’s regression test results (p = 0.45), which also suggest a low risk of publication bias.
Fig. 6
Funnel plots for the meta-analysis of the association between circulating GDF-15 level at admission and functional outcome after AIS
留言 (0)