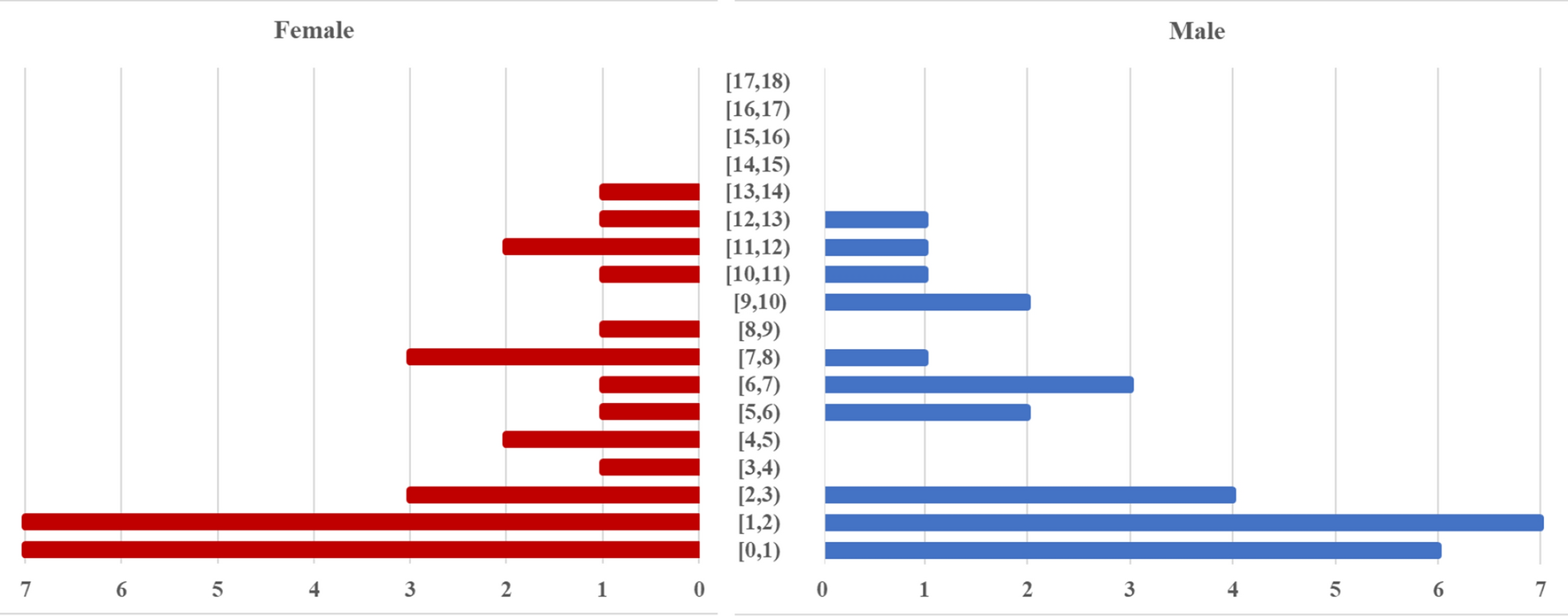
Our study compares the patient-related variables (blood loss, clinical outcomes, complication rate, VAS pain), hospital-related variables (surgical time, length of stay, re-admission rate) and surgeon-related variables (X-ray exposure) at 6 weeks and at 1-year follow-up in patients undergoing microsurgery for LDD. Selecting only patients with LDD gave us important insights into a similar group of patients in respect of a condition which can be operated by both COMS and MITM approaches. Overall, both study groups were comparable according to demographics, indications and comorbidities (all p > 0.05), which was a good basis for further investigations. This was also case for subgroup analysis according to indication.
In our hands, MITM had a shorter surgical time, compared to COMS (by 9.5 min). The results from the literature are mixed. However, Ryang and colleagues demonstrated no difference in operating times [16] while Righesso and colleagues, Huang and colleagues, and Teli and colleagues showed that COMS had a significantly shorter operating time in surgeries in which MITM was used as originally described [9, 13, 23].
In our study, blood loss was also lower in the MITM group (by 28 ml), in line with the findings of Pintea and colleagues and Huang and colleagues and supported by retrospective studies [13,14,15, 24]. In contrast, Ryang and colleagues and Righesso and colleagues demonstrated no difference in estimated blood loss between the MITM and COMS groups [13, 16]. Altogether, the amount of 28 ml difference between groups is clinically irrelevant and when intraoperative bleeding appears, it likely results from epidural veins or the segmental artery in foraminal explorations, which can bleed similarly in both groups. Approach-related significant haemorrhage is rare for both types.
The mean length of hospital stay (LOS) was 4.3 nights in the MITM group, which was significantly lower than in the COMS group (5.2 nights; p = 0.001). Huang and colleagues and Righesso and colleagues also reported a shorter hospital stay for patients treated with the MITM approach [9, 13]. There was no difference in the LOS in the studies carried out by Lau and colleagues [14] and Arts and colleagues [12].
With regard to complications, our study found no significant relationship between the microsurgical approach and the number of complications (p = 0.5). Nor was there any significant relationship found in our study between the microsurgical approach and the re-admission rate (p = 0.08). This applies for the overall as well as stratified analyses of the results for each of the indications except for LDH recurrence. The findings of our study relating to safety and feasibility are also in accord with those of Pintea and colleagues who, with a prospective analysis of MITM vs. COMS, reported that MITM is safe and effective, and those of Clark and colleagues who found no significant differences between complication rate and the microsurgical approach [15, 25, 26].
Subgroup analysis of complications showed a significantly lower rate of LDH recurrence in the MITM group (p = 0.004). In contrast, Ryang and colleagues as well as Huang and colleagues demonstrated no difference in recurrent LDH and cerebrospinal fluid leaks [16] or complications in general [13] while Teli and colleagues reported higher LDH recurrence rates in MITM patients [6]. The remaining complications were equally distributed and showed no significant differences.
All re-admitted patients had revision surgery. Detailed analysis of re-admitted patients in the MITM group vs. COMS group showed re-admissions/revisions due to: recurrence, 2 (1.6%) vs. 17 (5.8%); cerebrospinal fluid leak, 1 (0.8%) vs. 4 (1.4%); wound infection, 1 (0.8%) vs. 4 (1.4%); instability, 2 (1.6%) vs. 5 (1.7%), which was not significant. Differences between the groups according to different diagnoses were not significant either. This supports the hypothesis that these complications may rather occur due to the underlying pathology and are not related to the microsurgical approach [5, 27].
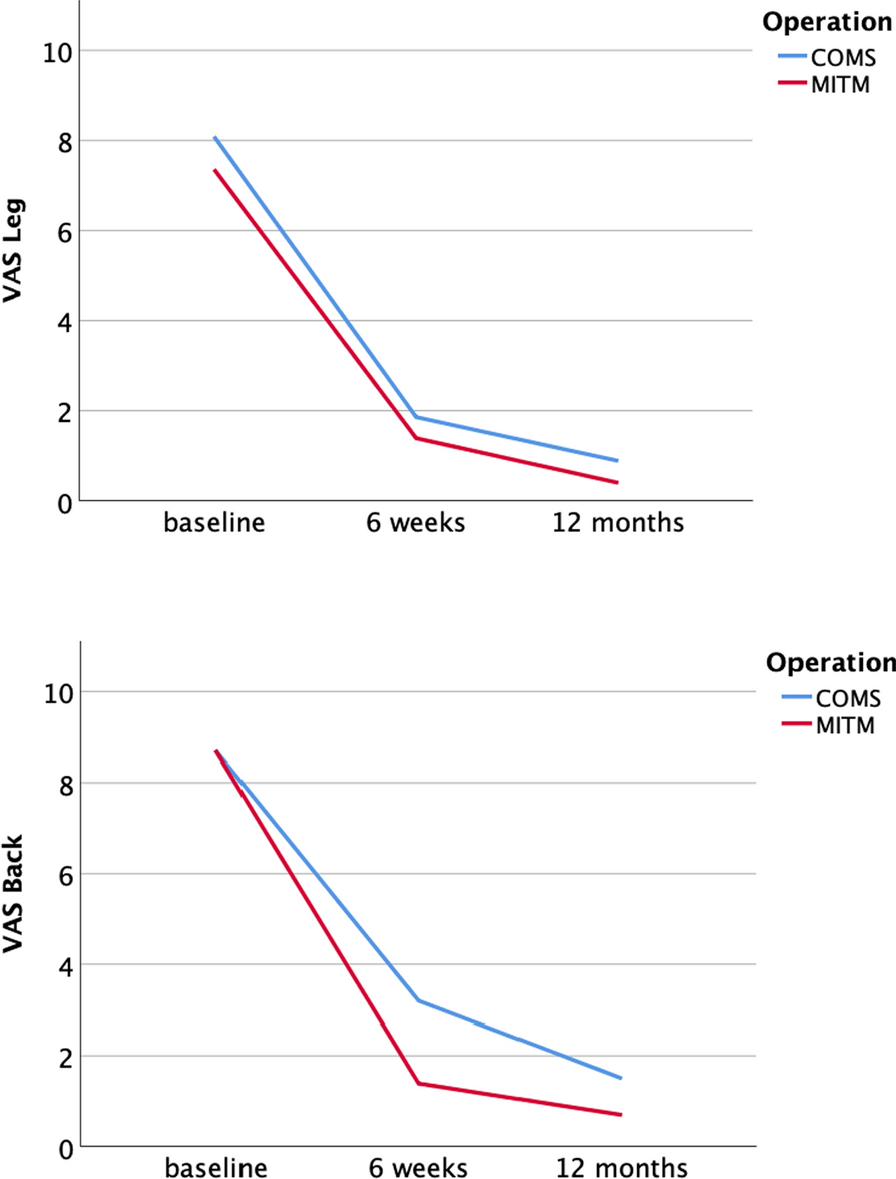
Mean clinical outcome was significantly better in the MITM group for both the Macnab criteria and VAS Scale (VAS Leg/VAS Back) at 6 weeks as well as 1 year postoperatively for any indication. This supports the original hypothesis that the surgical approach does not affect the natural course of disease, but it can reduce the secondary morbidity caused by surgery itself and can contribute to better clinical outcome. As the stratified analyses showed no different results comparing to combined MITM and COMS groups, the longitudinal analyses were performed for these groups combined with no further stratification for better visualization. The longitudinal analysis of VAS Back/VAS Leg showed a significant improvement from baseline to 6 weeks and from 6 weeks to 12 months follow-up. Interestingly, mean VAS Back in the COMS group at 6-week follow-up (3.2 [SD 1.1]) was significantly higher than in the MITM group (1.4 [SD 1.1]), which represents a clinically significant improvement [6] and corresponds with a slightly lower mean Macnab score (1.7 in COMS vs. 1.5 in MITM). This can be explained by the typically longer incision and likely a greater tissue trauma caused by COMS. Splitting the muscles by MITM leads to building of less scar tissue and thus faster healing. Psychological factors might also play big role as the patients aware of having only small incision trust themselves to be more active, less self-limiting, and therefore more satisfied. Patients from the MITM group in our sample felt better and performed better at the 6-week follow-up. This important finding can be helpful in deciding which type of approach to perform in specific types of patients.
The differences in the Macnab scores and both VAS pain scales between both study groups are no-longer as distinct at 12 months postoperative but still showing slight superiority of MITM to COMS in respect of VAS Score and Macnab scores, which is in contrary to two big RCT trials conducted by Pintea and colleagues [15] and Arts and colleagues [12] that showed an inferiority of MITM to COMS on that matter.
Further stratified analysis of both—MITM and COMS subgroups was performed according to indication (LDH, ELDH, LSS and cysts) in order to eliminate a bias that could be caused by differences resulting from different diagnoses leading to surgery. The different diagnoses did not show to have an impact on approach related features (blood loss, operating times and LOS) and proved the MITM to be significantly better (all p < 0.05).
A possible explanation for the findings relating to blood loss and surgery time between the approaches may lie in the level of experience and skill of the surgeons. For every surgeon, the learning curve is an important process at the end of which are more challenging operations and settings. In the study department, the MITM approach is performed by both older residents and attending neurosurgeons, while COMS is one of more frequent teaching operations performed by younger, less experienced colleagues at the beginning of their training so that we cannot fully exclude a systematic bias resulting from the experience of the primary surgeon.
Our results must be interpreted in line with consideration that we are a tertiary teaching hospital for residents in high-income European country with a high standard of care and resources which plays an important role in decision-making, timing of surgery and perioperative treatment as well as postoperative follow-up.
There are no reported values from large, randomized studies that consider the X-ray exposure in the MITM approach. In our study, we saw that the intraoperative mean Rx-dose measured in mGy (1.1 [SD 1.1]) and Gy.cm2 (0.3 [SD 0.3]), as well as mean exposure time (3.6 s [SD 2.0]) was significantly lower in the MITM group (all p < 0.05).
Overall, acceptance and implementation of a new surgical technique into daily praxis is a long process, which requires a thorough investigation providing a valid information on the safety and benefit for patients, institution and surgeons. The results of our study showed that MITM is a safe, feasible and beneficial for all three regardless of indication and confirms a nowadays’ trend towards the minimally invasive surgical approaches in spine surgery [28,29,30].
The strength of this study is that it was a large cohort, included various indications and a long-term follow-up. However, there are some limitations of our study that need to be addressed. First, we acknowledge the retrospective observational design of the study, which cannot eliminate (selection) bias, false or incomplete documentation or missing data. A prospective, randomized study would be a more rigorous tool for comparative studies such as ours. Secondly, as mentioned above, the MITM approach was preferably performed by experienced residents and attendings, whilst COMS is the standard “teaching approach” for operations performed by residents in training and that this could influence the results in terms of surgery time and blood loss.




留言 (0)