
{kind=link}
記住我










Coronary heart disease (CHD), also known as ischemic heart disease (IHD), is a heart disease characterizing with stenosis or occlusion of coronary artery caused by atherosclerosis, resulting in the plurality of world-wide morbidity and mortality. Coronary atherosclerosis is the foremost cause of mortality and loss of Disability Adjusted Life Years (DALYs) globally, which accounting for nearly 7 million deaths and 129 million DALYs annually.1 The boarder epidemiological studies have shown that high serum cholesterol is a key risk factor for CHD.2 In particular, low density lipoprotein cholesterol (LDL-C) has been considered as a casual contributor to CHD according to series of genetic studies, prospective epidemiological studies, Mendelian randomization studies and randomized control trials.3,4 Smoking, hypertension, diabetes, obesity and hereditary factor are also noteworthy factors.5,6 In addition, numerous studies have identified predictors of CHD, such as serum homocysteine, folate and C-reactive protein.7,8 However, there are also some studies suggesting junctional adhesion molecules (JAMs) played a significant role in atherosclerosis via promoting vascular inflammation and leukocyte infiltration.9
JAMs belong to the immunoglobulin superfamily, which is recognized as cell surface and soluble proteins involving in recognition, binding, or adhesion cells.9–11 Current studies have paid attention to four major JAM molecules: JAM1, JAM2, JAM3, JAM4, which first three of them are also known as JAM-A, JAM-B, JAM-C.12 They are expressed at tight junctions of epithelial and endothelial cells, and are variably expressed by smooth muscle cells, platelets, erythrocytes and leukocytes in humans, as well as by fibroblasts and smooth muscle cells in mice.13 The crosstalk between JAMs and integrins contributes to the functions of JAMs.14 Hence, JAMs are involved in the regulation of diverse functions like cell permeability, polarity and proliferation, tumor metastasis, angiogenesis or leukocytes transmigration during tissue inflammation.15 Increasing evidences indicated that JAMs present more and more association with atherosclerosis. In particularly, JAM-C was obviously up-regulated in the atherosclerotic vessel wall by ox-LDL, and in the spontaneous early lesion developed of ApoE−/− mice, JAM-C expression was increased.16 Anti-JAM-C antibody resulted in increased reverse transendothelial migration of monocyte-derived cells, as well as decreased neointima hyperplasia and neointima macrophage caused by wire injury of carotid arteries and an atherogenic diet.17,18 It is worth noting that JAM-C was found in soluble form presenting in serum of patients with rheumatoid arthritis.19 Given the role of JAM-C in vascular inflammation and leukocyte adhesion, its soluble form (sJAM-C) may serve as a circulating biomarker, reflecting the severity of atherosclerosis and coronary artery stenosis. Despite evidence linking JAM-C to atherosclerosis, the potential role of sJAM-C as a biomarker for coronary artery stenosis remains unexplored, representing a critical gap that this study seeks to address. Therefore, this study aims to investigate the relationship between serum sJAM-C levels and the severity of coronary artery stenosis, evaluating its potential as a biomarker for coronary artery stenosis.
Materials and Methods Patients and SamplesThis study was single-center, cross-sectional study. Admission data of patients with suspected CHD between July 2021 and May 2023 were retrospectively assessed in Beijing Luhe Hospital, Capital Medical University. Patients who went coronary angiography as recommended by their physician were included in the study. While patients who met one or more of the following criteria were excluded: (1) patients who suffered from severe cerebrovascular diseases, severe liver and kidney dysfunction, acute infection, malignant tumor, severe diseases of the endocrine and hematopoietic systems, mental diseases, pregnancy status, and patients in lactation, etc; (2) patients with contraindications to coronary angiography or who cannot cooperate with the arterial vascular examination. Duration of diabetes, smoking, alcohol consumption, and medication history were recorded. Among the 637 potential participants, 65 participants with missing blood samples and completed data were excluded, and 43 participants with outlier serum levels of sJAM-C were excluded. Finally, a total of 529 participants were enrolled in this study (Figure 1). All eligible patients were classified into five groups depending on Coronary Artery Disease Reporting and Data System (CAD-RADS).20 CAD-RADS classification criteria were based on the vessels with the most severe stenosis. The coronary artery stenosis severity was further divided into five groups: no visible stenosis, minimal or mild, moderate, severe and occluded. The severe degree of coronary artery stenosis in the 1–45% range is defined as minimal or mild, moderate refers to the degree of stenosis in the range of 50–69%, severe refers to the degree of stenosis in the range of 70–99%, occluded refers to total occlusion. Included patients were divided into five groups, no visible stenosis group, minimal or mild occlusion group, moderate occlusion group, severe occlusion group and occluded group for subsequent study analysis.

Figure 1 Form of participants through the trial.
The study complied with the Helsinki Declaration for investigation of human subjects and obtained ethical approval from the competent Institutional Review Boards of Beijing Luhe Hospital, Capital Medical University. All participants provided written informed consent.
Biochemical MeasurementsSystolic and diastolic blood pressure were measured using a standard mercury sphygmomanometer as described before.21 Venous blood samples were withdrawn from each patient in the morning after overnight fasting. Sera were separated with 1h. Routine laboratory measurements were performed, including total triglyceride (TG, mmol/L), total cholesterol (TC, mmol/L), low density lipoprotein cholesterol (LDL-C, mmol/L), high density lipoprotein cholesterol (HDL-C, mmol/L), C-reactive protein (CRP, ng/mL), hyper-sensitivity C-reactive protein (hs-CRP, mg/L), erythrocyte sedimentation rate (mm/h), and blood cell analysis. Serum samples were stored immediately at −80°C until further analysis.
Assessment of Circulating sJAM-CSerum JAM-C (ELH-JAMC, RayBiotech, Atlanta, GA, USA) level were measured by commercially available human ELISA kits according to the manufacturers’ instruction. The intra-assay coefficients of variation for sJAM-C was less than 10%, while the inter-assay coefficients of variation was less than 12%. This ELISA antibody pair detects human JAM-C. No cross-reactivity with human JAM-A, mouse JAM-A, or mouse JAM-C was observed.
Statistical AnalysisStatistical analyses were performed using SPSS 21.0 software (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov test was used to testing the normality of the data. Variables were expressed as mean ± standard deviation (SD) or median (interquartile ranges). For continuous data, variables conforming to the normal distribution were analyzed by Student’s t-tests for the differences between two groups. Variables that are not normally distributed were used Mann–Whitney test. For comparisons among multiple groups, one-way ANOVA followed by Turkey’s post-hoc analysis was conducted. Binary logistic regression analysis was conducted to explore the association between sJAM-C and coronary artery stenosis. Three models were established and adjusted for a different covariate. Model 1 was adjusted for age and sex, which was a relative cruded model used to explore the based relationship between sJAM-C and coronary artery stenosis. The unhealthy lifestyle or diseases such as smoke, drink, diabetes and hypertension have adverse effects on cardiovascular disease,22 so we adjust for smoke, drink, diabetes and hypertension plus covariate of model 1. And the model 3 was input all variable in model 2 plus TC, TG, HDL-C, LDL-C to adjust for common possible confounding factors. Furthermore, receiver operating characteristic (ROC) curve was performed to estimate the diagnostic value of sJAM-C on coronary artery stenosis and to quantify the diagnostic ability using an area under the curve (AUC). The closer the AUC is to 1, the better the diagnostic effect of the variable. The P values of <0.05 were considered statistically significant.
Results Demographic and Clinical CharacteristicIn this study, we enrolled 529 participants. The demographic and clinical characteristics of the study participants according to the two groups are described in Table 1. Participants in the two groups were comparable in age, sex, drinking, smoking, blood pressure, lipid profiles, blood cells ratios and indicators of liver function. The medium age was 63 years and 51.7% were females in coronary artery stenosis group, which was similar to the no stenosis group. 37.7% participants in coronary artery stenosis groups had diabetes, which was significantly higher than the 23.1% prevalence in the no stenosis group. And the plasma level of TC and LDL-C in participants with coronary artery stenosis was 4.4147 ± 1.07376 mmol/L and 2.7883 ± 0.85974 mmol/L, respectively, and significantly higher than those in no stenosis group. White blood cell, neutrophil, blood platelet, CRP and hs-CRP elevated in coronary artery stenosis, which reflected a higher inflammatory burden in coronary artery stenosis patients (Table 1).

Table 1 Demographic Information and Clinical Characters of Participants
Serum sJAM-C Content was Increased with the Degree of Coronary Artery StenosisCoronary artery stenosis was divided into four groups according to CAD-RADS: minimal or mild (the degree of coronary artery stenosis in 1–45% range), moderate (the degree of stenosis in the range of 50–69%), severe (the degree of stenosis in the range of 70–99%) and occluded (total occlusion). The serum level of sJAM-C in both severe and occluded groups were higher than that in the no stenosis group (p < 0.0001). And the sJAM-C levels in the severe and occluded groups are higher than those in the moderate group, with p-values of 0.0001 and 0.0004, respectively. It is worth noting that the level of sJAM-C was gradually increase in stenosis degree (Figure 2). Taking together, the higher the serum sJAM-C level, the more severe the coronary stenosis.

Figure 2 Serum sJAM-C level in patients without and with different severity of coronary artery stenosis. One-way ANOVA and Turkey’s multiple comparison test were used to determine statistical stage.
Association Between Serum sJAM-C Level and Coronary Artery StenosisThe association between serum sJAM-C level and coronary artery stenosis was described by β value of binary logistic regression analysis (Table 2). In the model 1 (cruded model), the β value for 1-SD increase of sJAM-C levels were 1.266, and the OR value was 3.408 (95% CI 2.164–5.368, p < 0.0001). Due to the unhealthy lifestyle or disease such as smoke, drink, diabetes and hypertension, are risk factors for cardiovascular diseases, we adjusted for these factors in Model 2. The β value for 1-SD increase of sJAM-C level was 1.249, and the OR value was 3.487 (95% CI 2.204–5.516, p < 0.0001). Additionally, the model 3 was input all variable in model2 puls TG, TC, LDL-C, HDL-C to adjust for common possible confounding factors. It was found out that sJAM-C was significantly and positively associated with coronary artery stenosis, and the value for 1-SD increase of sJAM-C levels was 1.127, and the OR value was 3.088 (95% CI 1.922–4.960, p < 0.0001) in model 3.

Table 2 The Association Between sJAM-C and Coronary Artery Stenosis
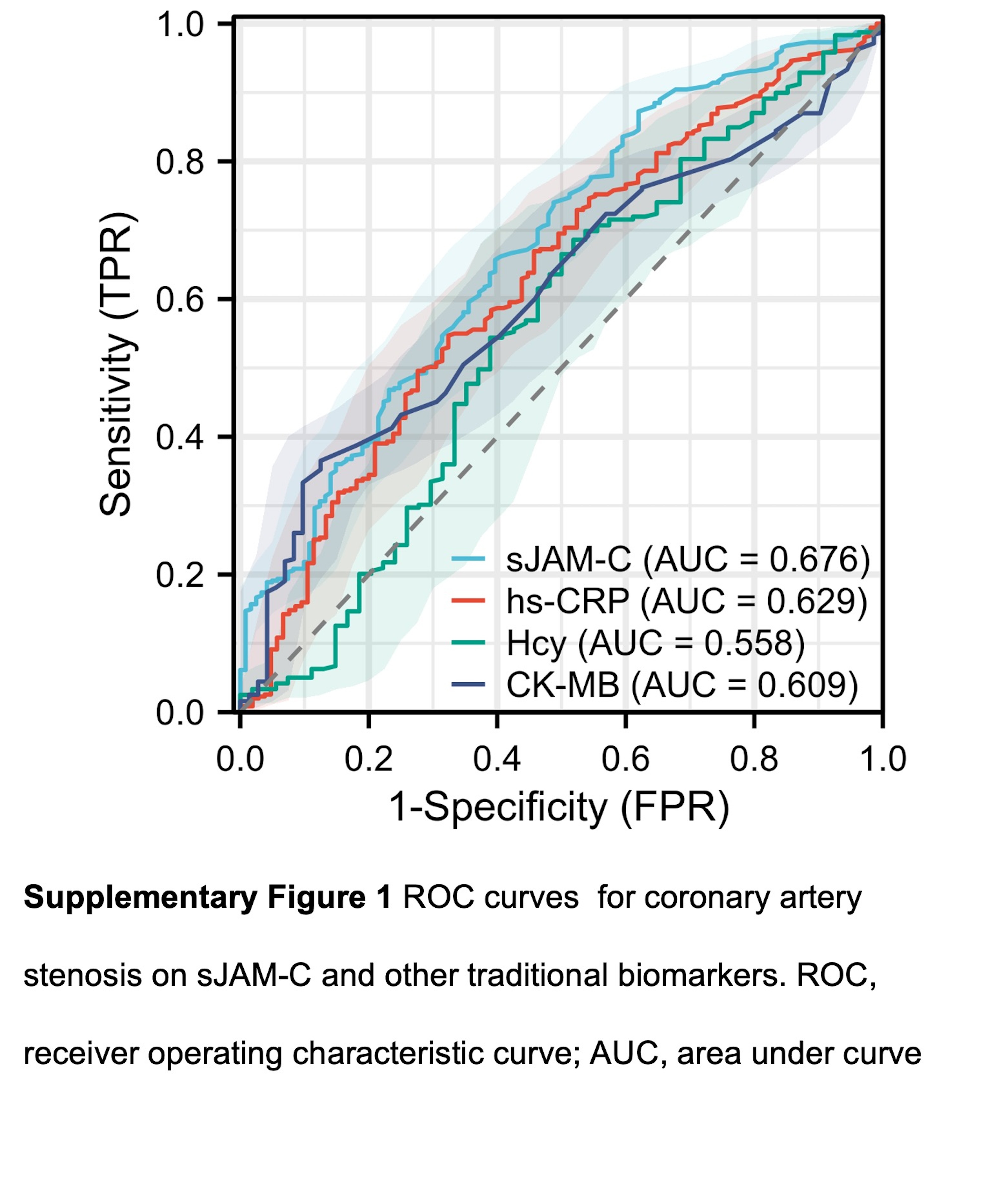
Diagnostic Value of the Level of Serum sJAM-C for Coronary Artery StenosisIn order to quantify the diagnostic ability of sJAM-C between no stenosis group and coronary stenosis group, we conducted ROC curve analysis. The results revealed that sJAM-C has a certain diagnostic ability for coronary artery stenosis (AUC = 0.676, 95% CI 0.622–0.730) (Figure 3). Interestingly, sJAM-C showed better diagnostic ability than other traditional biomarkers, like CK-MB (AUC = 0.609, 95% CI 0.543–0.675), hs-CRP (AUC = 0.629, 95% CI 0.568–0.690) and Hcy (AUC = 0.558, 95% CI 0.466–0.649) in our study (Supplementary Figure 1). The cut-off value of sJAM-C was 18.1 pg/mL, with a sensitivity of 65.7% and specificity of 60.3%, indicating that it may be a potential biomarker of coronary artery stenosis.

Figure 3 ROC curves for coronary artery stenosis on sJAM-C.
Abbreviations: ROC, receiver operating characteristic curve; AUC, area under curve; CI, confidence interval.
DiscussionOur study provided a novel insight into the role of sJAM-C in coronary artery stenosis. In this study, we detected the serum sJAM-C level of 529 patients with or without coronary artery stenosis to explore the association between sJAM-C and coronary artery stenosis. We found that the level of sJAM-C was significantly elevated in patients with coronary artery stenosis. And the higher level of sJAM-C, the higher degree of coronary artery stenosis. Our study not only confirmed the association between sJAM-C and coronary artery stenosis via binary logistic regression analysis but also indicated that sJAM-C showed a certain diagnostic value for coronary artery stenosis. Our findings provide supports for that sJAM-C is a potential biomarker for coronary artery stenosis.
The major pathological basis of coronary artery stenosis is atherosclerosis, which is characterized by lipid deposition in the inner artery.23 The process is initiated by endothelium activation, followed by vascular cell adhesion molecule-1 and intercellular cell adhesion molecule-1 expressing, adhesion of monocytes, inflammation activation and atheroma plaque formation ultimately resulting in CHD.23,24 JAMs regulated the transient interaction between leukocytes and endothelial cells via integrins. Previous studies have reported that ox-LDL increased JAM-C expression and induced disorganization of JAM-C localization on endothelial cells. Furthermore, anti-JAM-C reduced monocyte accumulation at vascular inflammation sites by increasing reverse transmigration rather than reducing transmigration.16,25 These results suggested that JAM-C is associated with CHD. Interestingly, the JAM-C ectodomain can be cleaved and secreted in a soluble form. Given the role of JAM-C in vascular inflammation and leukocyte adhesion, sJAM-C may be a marker of coronary artery stenosis. Nevertheless, the relationship between sJAM-C and coronary artery stenosis has not been proved. Therefore, this study was aimed at the potential connection between sJAM-C and coronary artery stenosis, and whether sJAM-C can be used as a new biomarker for coronary artery stenosis.
Previous studies have demonstrated that the serum level of sJAM-C was elevated in patients with rheumatoid arthritis.19 Coronary artery stenosis is also related to vascular inflammation, and individuals with coronary artery stenosis have low grades of inflammation. Consistent with our study, we found that the level of sJAM-C was increased in patients with coronary artery stenosis, and the sJAM-C levels increased with the severity of the coronary artery stenosis. In this study, we explored the associations between sJAM-C and coronary artery stenosis by binary logistic regression analysis and found sJAM-C had strong association with coronary artery stenosis. In Model 1, we adjusted age and gender to preliminarily explore the relationship between sJAM-C and coronary artery stenosis. Smoking is a traditional risk factor for CHD and contributes to the development of atherosclerosis by causing vascular endothelial dysfunction and inflammatory response. And alcohol consumption of any amount was associated with increased cardiovascular risk.26 Additionally, diabetes and hypertension are closely related to the occurrence of CHD.27,28 Therefore, we adjusted for unhealthy lifestyle and disease status in Model 2. Since cholesterol, especially LDL-C, has been identified as a key risk factor for the development of atherosclerosis, Model 3 includes all variables from Model 2 plus TC, TG, HDL-C, and LDL-C to adjust for common possible confounding factors. It is noteworthy that sJAM-C was significantly and positively associated with coronary artery stenosis for adjusting age, sex, lifestyle, disease status, TG, TC, LDL-C and HDL-C.
We found that after adjusting for confounding factors, sJAM-C remained an independent risk factor for coronary artery stenosis. sJAM-C may be involved in coronary artery stenosis through a variety of mechanisms. However, to date, little is known about the signaling cascade triggered by membrane-bound JAM-C, and this is the first study to show that sJAM-C is elevated in the serum of patients with coronary artery stenosis. Previous studies have demonstrated that JAMs are capable of isotypic and allotypic interactions with neighboring JAM molecules.14,29 Therefore, we speculate that sJAM-C may initiate endothelium activation by binding to membrane-bound JAM-B or JAM-C on the surface of endothelial cells. Of course, there are additional, yet unidentified, sJAM-C receptors present on endothelial cells possibly. These bindings play a crucial role in intercellular signal transduction. In terms of signal transduction, it is reported that sJAM-C can trigger the phosphorylation of Src, p38, and PI3K in human microvascular endothelial cells.19 The Src, p38, and PI3K pathways mediate the occurrence of CHD; thus, this may be the mechanism linking sJAM-C with coronary artery stenosis.30–32 Therefore, we hold the opinion that sJAM-C increase in patients with coronary artery stenosis, may be related to monocytes adhesion and endothelium inflammation activation, which could accelerate the pathology of atherosclerosis. However, the underlying mechanisms need further exploration.
On the other hand, we tested the diagnostic performance of sJAM-C for coronary artery stenosis by ROC analysis. Primary prevention is very important for delaying the progression of atherosclerosis and preventing adverse cardiovascular events, so early identification of coronary artery stenosis is of great value. A number of biochemical indicators are used to predict the occurrence of CHD, including CK-MB, hs-CRP and Hcy. In this study, we compared the diagnostic value of different indicators for coronary artery stenosis and found that the diagnostic value of sJAM-C was better than that of hsCRP, CK-MB and Hcy. sJAM-C is produced by endothelial cell in vessels, and is a more accurate indicator of the extent of coronary artery stenosis. Studies have also shown that sJAM-C is associated with endothelium activation. Therefore, sJAM-C is a better diagnostic indicator for coronary artery stenosis than traditional indicators.
However, there are some limitations in this study. First of all, we have not yet demonstrated in animal models or in vitro that sJAM-C is elevated in response to coronary artery stenosis. We will further explore the mechanism of serum sJAM-C increase in coronary artery stenosis in vivo or in vitro. Second, we found that sJAM-C was associated with coronary artery stenosis, but further is needed to uncover the effect of sJAM-C on coronary artery stenosis. Further research should be undertaken to explore more precise methods for assessing the severity of coronary heart disease, such as intravascular ultrasound and vascular optical coherence tomography. Third, we are short of information on certain comorbidities that could potentially influence sJAM-C, such as stroke and dementia. These conditions are associated with endothelium injury and inflammation and may impact sJAM-C level. The absence of this data limits our understanding of the potential confounding effects of these comorbidities on sJAM-C level in patients with coronary artery disease. Fourth, this study was conducted at a single center, which could limit the generalizability of the findings. Although we match age and gender of the groups, the relatively small sample size may affect the statistical power. Finally, due to the cross-sectional design of our study, it is challenging to establish a causal relationship between serum sJAM-C level and coronary artery stenosis. The level of sJAM-C may be a consequence rather than a cause of coronary artery stenosis. To gain a clear understanding of the role of serum sJAM-C in coronary artery stenosis, large-longitudinal studies and mechanistic investigations are required.
ConclusionIn summary, the serum sJAM-C levels are associated with coronary artery stenosis, and closely related to the degree of coronary artery stenosis. Additionally, sJAM-C demonstrates a certain diagnostic value in coronary artery stenosis. These findings suggest that sJAM-C may be a potential biomarker for coronary artery stenosis for predicting the occurrence and development of CHD.
AbbreviationsAUC, area under the curve; TG, total triglyceride; TC, total cholesterol; LDL-C, low density lipoprotein cholesterol; HDL-C, high density lipoprotein cholesterol; sJAM-C, soluble JAM-C.
AcknowledgmentsThe authors would like to appreciate National Science Funding, Tongzhou District science and technology committee and Beijing Luhe Hospital, Capital Medical University for supporting our project.
Author ContributionsDi Wang participated in the design of the study and performed the ELISA, statistical analysis and drafted the manuscript. Lin Mao collected the clinical data and performed the ELISA. Kun Li provided support for statistical analysis. Lu Wang and Yan Wang offered help in clinical data interpretation. Longyan Yang were major contributor to the design of this study and also revised the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
FundingThis study received support from the National Science Funding in China (81800768 and 82170454), Tongzhou District Science and Technology Project (KJ2023CX036 and KJ2022CX017), and Beijing Luhe Hospital, Capital Medical University, Youth Research Incubation Project (LHYY2023-JC207).
DisclosureThe authors report no conflicts of interest in this work.
References1. Ralapanawa U, Sivakanesan R. Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: a narrative review. J Epidemiol Glob Health. 2021;11(2):169–177. doi:10.2991/jegh.k.201217.001
2. Goldstein JL, Brown MS. A century of cholesterol and coronaries: from plaques to genes to statins. Cell. 2015;161(1):161–172. doi:10.1016/j.cell.2015.01.036
3. Gofman JW, Delalla O, Glazier F, et al. The serum lipoprotein transport system in health, metabolic disorders, atherosclerosis and coronary heart disease. J Clin Lipidol. 2007;1(2):104–141. doi:10.1016/j.jacl.2007.03.001
4. Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European atherosclerosis society consensus panel. Eur Heart J. 2017;38(32):2459–2472. doi:10.1093/eurheartj/ehx144
5. Blankstein R, Budoff MJ, Shaw LJ, et al. Predictors of coronary heart disease events among asymptomatic persons with low low-density lipoprotein cholesterol Mesa (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol. 2011;58(4):364–374. doi:10.1016/j.jacc.2011.01.055
6. Katta N, Loethen T, Lavie CJ, Alpert MA. Obesity and coronary heart disease: epidemiology, pathology, and coronary artery imaging. Curr Probl Cardiol. 2021;46(3):100655. doi:10.1016/j.cpcardiol.2020.100655
7. Gopinath B, Flood VM, Rochtchina E, Thiagalingam A, Mitchell P. Serum homocysteine and folate but not vitamin B12 are predictors of CHD mortality in older adults. Eur J Prev Cardiol. 2012;19(6):1420–1429. doi:10.1177/1741826711424568
8. Wang X, Wu YL, Zhang YY, et al. AK098656: a new biomarker of coronary stenosis severity in hypertensive and coronary heart disease patients. Diabetol Metab Syndr. 2022;14(1):10. doi:10.1186/s13098-022-00783-3
9. Wang J, Chen X. Junctional adhesion molecules: potential proteins in atherosclerosis. Front Cardiovasc Med. 2022;9:888818. doi:10.3389/fcvm.2022.888818
10. Ebnet K, Suzuki A, Ohno S, Vestweber D. Junctional adhesion molecules (JAMs): more molecules with dual functions? J Cell Sci. 2004;117(Pt 1):19–29. doi:10.1242/jcs.00930
11. Kostrewa D, Brockhaus M, D’Arcy A, et al. X-ray structure of junctional adhesion molecule: structural basis for homophilic adhesion via a novel dimerization motif. EMBO J. 2001;20(16):4391–4398. doi:10.1093/emboj/20.16.4391
12. Mendoza C, Nagidi SH, Mizrachi D. Molecular characterization of the extracellular domain of human junctional adhesion proteins. Int J Mol Sci. 2021;22(7):3482. doi:10.3390/ijms22073482
13. Bazzoni G. The JAM family of junctional adhesion molecules. Curr Opin Cell Biol. 2003;15(5):525–530. doi:10.1016/S0955-0674(03)00104-2
14. Lamagna C, Meda P, Mandicourt G, et al. Dual interaction of JAM-C with JAM-B and alpha(M)beta2 integrin: function in junctional complexes and leukocyte adhesion. Mol Biol Cell. 2005;16(10):4992–5003. doi:10.1091/mbc.e05-04-0310
15. Hintermann E, Bayer M, Conti CB, et al. Junctional adhesion molecules JAM-B and JAM-C promote autoimmune-mediated liver fibrosis in mice. J Autoimmun. 2018;91:83–96. doi:10.1016/j.jaut.2018.05.001
16. Keiper T, Al-Fakhri N, Chavakis E, et al. The role of junctional adhesion molecule-C (JAM-C) in oxidized LDL-mediated leukocyte recruitment. FASEB J. 2005;19(14):2078–2080. doi:10.1096/fj.05-4196fje
17. Shagdarsuren E, Djalali-Talab Y, Aurrand-Lions M, et al. Importance of junctional adhesion molecule-C for neointimal hyperplasia and monocyte recruitment in atherosclerosis-prone mice-brief report. Arterioscler Thromb Vasc Biol. 2009;29(8):1161–1163. doi:10.1161/ATVBAHA.109.187898
18. Bradfield PF, Menon A, Miljkovic-Licina M, et al. Divergent JAM-C expression accelerates monocyte-derived cell exit from atherosclerotic plaques. PLoS One. 2016;11(7):e0159679. doi:10.1371/journal.pone.0159679
19. Rabquer BJ, Amin MA, Teegala N, et al. Junctional adhesion molecule-C is a soluble mediator of angiogenesis. J Immunol. 2010;185(3):1777–1785. doi:10.4049/jimmunol.1000556
20. Cury RC, Leipsic J, Abbara S, et al. CAD-RADS 2.0 - 2022 Coronary Artery Disease-Reporting and Data System: an Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Cardiology (ACC), the American College of Radiology (ACR), and the North America Society of Cardiovascular Imaging (NASCI). JACC Cardiovasc Imaging. 2022;15(11):1974–2001. doi:10.1016/j.jcmg.2022.07.002
21. Yang L, Wang Y, Xu Y, et al. ANGPTL3 is a novel HDL component that regulates HDL function. J Transl Med. 2024;22(1):263. doi:10.1186/s12967-024-05032-x
22. Mury P, Mura M, Della-Schiava N, et al. Association between physical activity and sedentary behaviour on carotid atherosclerotic plaques: an epidemiological and histological study in 90 asymptomatic patients. Br J Sports Med. 2020;54(8):469–474. doi:10.1136/bjsports-2018-099677
23. Libby P, Buring JE, Badimon L, et al. Atherosclerosis. Nat Rev Dis Primers. 2019;5(1):56. doi:10.1038/s41572-019-0106-z
24. Jebari-Benslaiman S, Galicia-Garcia U, Larrea-Sebal A, et al. Pathophysiology of Atherosclerosis. Int J Mol Sci. 2022;23(6). doi:10.3390/ijms23063346
25. Bradfield PF, Scheiermann C, Nourshargh S, et al. JAM-C regulates unidirectional monocyte transendothelial migration in inflammation. Blood. 2007;110(7):2545–2555. doi:10.1182/blood-2007-03-078733
26. Biddinger KJ, Emdin CA, Haas ME, et al. Association of habitual alcohol intake with risk of cardiovascular disease. JAMA Network Open. 2022;5(3):e223849. doi:10.1001/jamanetworkopen.2022.3849
27. Yang T, Liu Y, Li L, et al. Correlation between the triglyceride-to-high-density lipoprotein cholesterol ratio and other unconventional lipid parameters with the risk of prediabetes and Type 2 diabetes in patients with coronary heart disease: a RCSCD-TCM study in China. Cardiovasc Diabetol. 2022;21(1):93. doi:10.1186/s12933-022-01531-7
28. Liu Y, Zhu B, Zhou W, et al. Triglyceride-glucose index as a marker of adverse cardiovascular prognosis in patients with coronary heart disease and hypertension. Cardiovasc Diabetol. 2023;22(1):133. doi:10.1186/s12933-023-01866-9
29. Arrate MP, Rodriguez JM, Tran TM, Brock TA, Cunningham SA. Cloning of human junctional adhesion molecule 3 (JAM3) and its identification as the JAM2 counter-receptor. J Biol Chem. 2001;276(49):45826–45832. doi:10.1074/jbc.M105972200
30. Hussain M, Ikram W, Ikram U. Role of c-Src and reactive oxygen species in cardiovascular diseases. Mol Genet Genomics. 2023;298(2):315–328. doi:10.1007/s00438-023-01992-9
31. Fan S, Xiao G, Ni J, et al. Guanxinning injection ameliorates cardiac remodeling in HF mouse and 3D heart spheroid models via p38/FOS/MMP1-mediated inhibition of myocardial hypertrophy and fibrosis. Biomed Pharmacother. 2023;162:114642. doi:10.1016/j.biopha.2023.114642
32. Li F, Peng J, Lu Y, et al. Blockade of CXCR4 promotes macrophage autophagy through the PI3K/AKT/mTOR pathway to alleviate coronary heart disease. Int J Cardiol. 2023;392:131303. doi:10.1016/j.ijcard.2023.131303
留言 (0)