The main findings of this study were a significant increase in both the total number and the IR of emergency calls over the study period. A geographical variation in the IR was found. Men made up just over half of the cases, and the elderly constituted the largest portion of the study population, with some variation across different areas. The most common reasons for emergency calls were unclear problems, chest pain, breathing difficulties, neurological issues, accidents, and minor injuries.
Variations in incidence rate
The notable increase in the volume of emergency calls to the EMDC over the study period underscores several important considerations. The rising trend in emergency calls reflects an escalating demand for EMS within the region. This trend has also been found in other studies. Herr et al. [15] found an overall increase in emergency calls of 9.1% over a three-year period from 2018 to 2021 in Berlin. Campagna et al. [16] found a 34% increase in total number of calls over a four-year period from 2013 to 2017 in Italy, and at the same time emergency call IR increased from 55 to 102 calls/1000 residents/year. This increased demand could stem from various factors, including access to other medical services or changes in healthcare utilization patterns. Thus, a new report found a significant decrease in available general practitioners in Region Zealand during the last 15 years [17]. Moreover, a recent review found that systemic barriers to timely primary care, coupled with patient perceptions of urgency and reliance on emergency services for immediate assistance, lead many individuals to default to ambulance use even for non-critical conditions [18].
Geographical variations
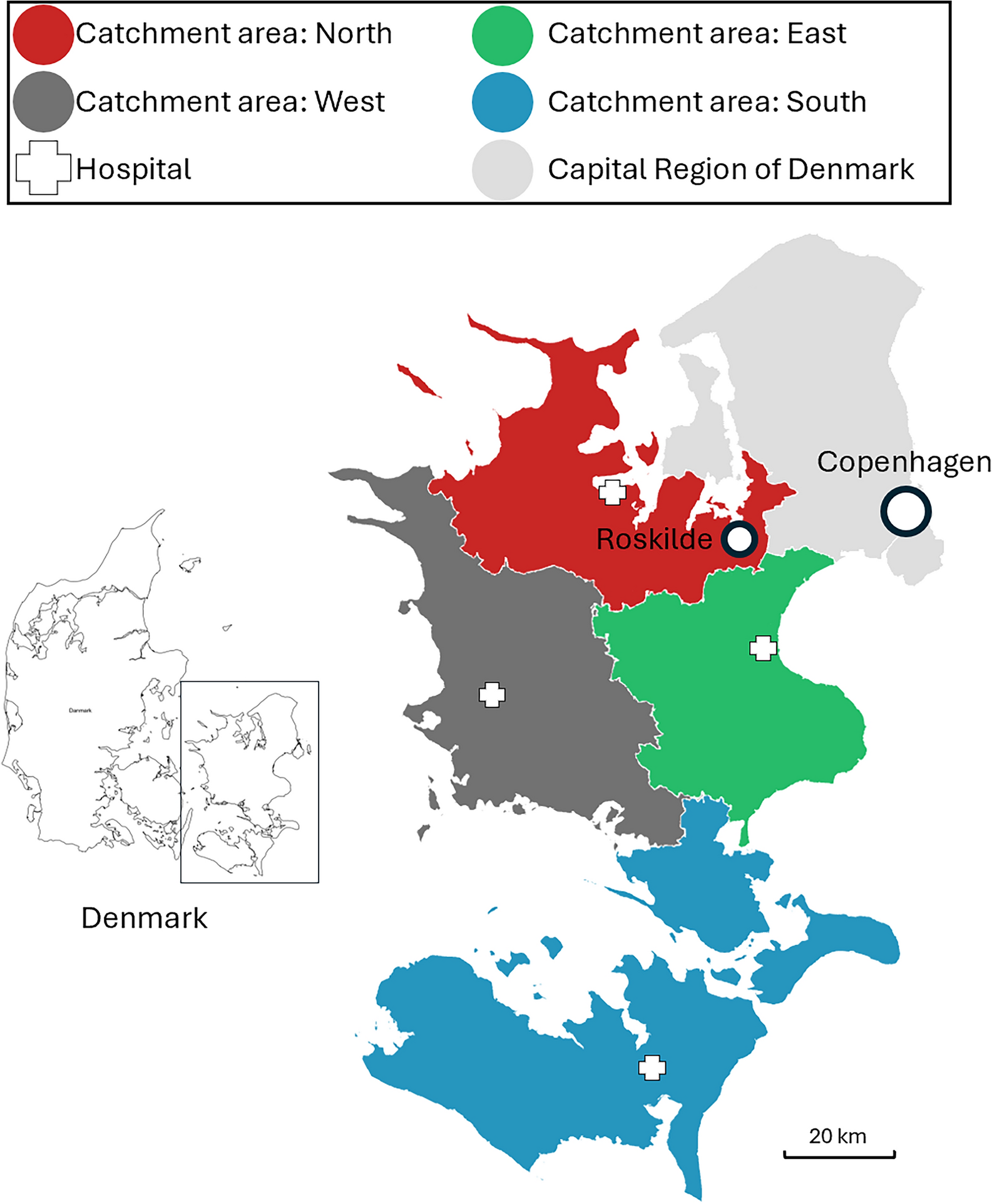
The finding of geographic variations in numbers of emergency calls also merit attention, as they may reflect differences in population density, socioeconomic factors, and healthcare infrastructure across different regions within the study area. The findings are comparable with a study by Hegenberg et al. [19] who found a difference in emergency call IR between rural municipalities and larger cities, with respective 42.8 and 80.7 emergencies/1,000 residents/year suggesting that future EMS planning should be targeted to regional characteristics. In addition, a newly published study from our group, which examines the increase in ambulance missions alongside trends in age composition and comorbidity across the four geographic areas analyzed in this article, found a larger increase in the proportion of elderly in the southern part of the region, which may contribute to the findings in this study [20].
Furthermore, numbers from Statistics Denmark show that the municipalities corresponding to the southern catchment area have a lower level of employment, a lower average income, fewer highly educated people, and a shorter lifespan, pointing to overall poorer health [11]. Finally, a recent report on the region's health profile has shown that there are more citizens with long-term illnesses in the southern part of the area [21].
Contact causes
The pattern of contact causes to the EMS through emergency calls are similar to findings in other studies. In a previous investigation in the Capital Region of Denmark, “unclear problem” was the most frequent cause of contact, accounting for 19% of cases and the five most common known causes were categorized as “wounds, fractures, minor injuries” (13%), “chest pain/heart disease” (11%), “accidents” (9%), “intoxication, poisoning, drug overdose” (8%), and “breathing difficulties” (7%) [12]. In addition, 81% of calls were assigned Emergency levels A and B, which is comparable to our findings.
The categorization of causes of emergency calls has been shown to be associated with mortality. One study found that “unclear problem” was associated with higher mortality for emergency level B calls compared to those with a known cause [22]. Another study found that “unclear problem” was among the three most deadly dispatch categories of causes during emergency calls, along with “breathing difficulties” and “unconscious adult/possible cardiac arrest" [23]. Both studies highlight the need for improvement of emergency call handling and the underlying supportive decision tools. Educational interventions at the dispatch centers may improve the procedure, as shown in a recent study, where categorization of the cause as “unclear problem” by medical dispatchers was markedly reduced after a period of increased focus on specific categorization of causes of emergency calls [24].
Overall, these studies emphasize the need for more accurate dispatch systems to ensure efficient use of EMS resources and optimal patient outcomes. Accurate dispatch is crucial for the effective utilization of limited EMS resources. Various studies have evaluated the performance of different dispatch systems. A systematic review aimed to assess the evidence for medical dispatch systems' accuracy in identifying the level of acuity and specific conditions. The review included 18 studies, finding a very low to low level of evidence for dispatch system accuracy [25]. One observational study of trauma patients transported to major trauma centers assessed dispatch accuracy by evaluating the sensitivity, under- and overtriage rates. While most patients requiring specialized care were assigned the highest priority by dispatch centers and EMS professionals, significant undertriage rates existed at the same time, indicating suboptimal prehospital triage accuracy for trauma patients [26]. Another study examined the Geneva emergency medical dispatch system (EMD), revealing good specificity but low sensitivity in dispatching emergency physicians. This study suggested using the dichotomy between immediate life-threatening emergencies and other emergencies as a reference standard for future performance assessments [27]. Research in Norway validated the Norwegian dispatch tool as an effective predictor of patients not needing pre-hospital interventions, particularly for low-acuity cases. However, it also highlighted the challenge of evaluating adherence to protocols due to the necessity of medical expertise in the triage process [28]. Lastly, a study analyzing 6,416 EMS dispatches found discrepancies between EMD and EMS priorities, with the EMD often overestimating the urgency of dispatches. While the EMD was consistent in identifying non-urgent cases, its overestimation of urgent cases could impact the availability of EMS for truly urgent missions, suggesting a need for improved accuracy to enhance EMS efficiency [29]. Notably, the dispatchers in this study were highly trained nurses or paramedics, reflecting a high level of medical expertise. This high level of competence is further supported by their continuous professional development, ensuring their skills and knowledge remain aligned with evolving standards in emergency medical care, which should be considered.





留言 (0)