Our study demonstrates that men with Fabry disease are more likely to progress to incident renal decline over at least six years, despite no significant inter-sex differences with respect to traditional cardiovascular and/or renal risk factors (Table 1). Out of 395 participants with Fabry disease, approximately 33% were CKD-free at baseline. Further analysis of 260 participants showed that half of this cohort did not have CKD at entry into the study, with approximately 25% going on to develop incident CKD over a follow-up of > 11 years. Overall, men had significantly higher incidence rates of initiating disease modifying treatments, non-fatal cardiovascular events and all-cause mortality, as well as a greater rate of decline in eGFR and progression to KRT. Further sub-cohort analysis revealed that advanced age, higher uACR (> 2.3 mg/mol), and history of ischaemic heart disease and/or transient ischaemic attack were associated with faster eGFR progression, irrespective of sex. Moreover, those going on to develop incident CKD were on average eight years older, had pre-existing ischaemic heart disease, and experienced a higher rate of eGFR progression than those who remained CKD-free at the end of follow-up. It is worth noting that our study accounts for both age-related physiological decline (‘slow or natural progressors’ in eGFR in addition to including ‘intermediate’ and ‘fast progressors’, which is above and beyond the acceptable age-related decline of approximately −1 ml/min/year) [10]. We acknowledge that another key factor influencing eGFR progression is the timely start of disease modifying treatment. Whilst our database records the start time of these therapies, it does not always confirm the timeliness of their initiation in terms of clinical disease activity, as this can be influenced by the referral process to our specialist Tertiary centre. It is well-documented in the literature that the interval between disease presentation and diagnosis can span 7 to 10 years, which we have captured in our follow-up duration.
A further important finding from this study is that individuals exhibiting elevated uACR or decreased eGFR, even when these values remain within clinically accepted ‘normal’ ranges, are at increased risk of developing CKD. This observation underscores the importance of vigilant monitoring of these biomarkers. For instance, a subtle increase in uACR from 1 to 2 mg/mmol, or a decline in eGFR from 89 to 80 ml/min/1.73m2, should prompt suspicion of potential CKD progression and might necessitate early intervention, including the initiation of disease-modifying treatments. Such proactive management strategies could potentially mitigate the progression to overt CKD.
It has been previously shown that a urine protein-to-creatinine ratio (uPCR) of > 1000 mg/g (> 100 mg/mmol) in Fabry disease significantly increased the risk of developing ESKD, irrespective of whether patients received enzyme replacement therapy [11]. We further characterised baseline participant demographics and outcome measures according to quantified uACR cut-offs, demonstrating that individuals with uACR > 30 mg/mmol were also more likely to experience outcomes of non-fatal cardiovascular events, all-cause mortality, and require KRT.
Our study indicates that even small increases in uACR may predict renal decline in those developing CKD. Building on our findings, there may be a role for the initiation of newer drugs used in renal care, such as Sodium-glucose co-transporter-2 (SGLT2) inhibitors; upon detecting proteinuria in Fabry patients there is a case for early intervention with SGLT2 inhibitors in order to slow eGFR progression. The ongoing DEFY study could provide insights into the use of SGLT2 inhibitors in Fabry treatment protocols [12].
We show that uACR > 30 mg/mmol is associated with a statistically significant increased risk of developing ESKD, thus confirming the importance of regular uACR testing as part of Fabry clinical care. Interestingly, age was an independent risk factor for rapid rate of eGFR decline, whilst other established risk factors for developing CKD such as hypertension and diabetes were not found to be of significance in this study. This is at odds with a paper published by Nasu et al. which found elevated systolic blood pressure was associated with a faster decline in eGFR in patients with Fabry disease [13]. We acknowledge this is likely due to the relatively low number of patients with hypertension (22.9%) and diabetes (2.7%) at baseline, who would then continue to develop renal sequelae from these conditions, irrespective of having Fabry disease.
Participants taking RAAS inhibitors in our study were shown to have reduced rates of eGFR decline; this is in keeping with published data of patients with proteinuria, in whom these drugs have long demonstrated a renoprotective effect [14]. A higher proportion (42.5%) of patients in the rapid progressor group received a RAASi, as indicated. The main European Fabry Working Group recommendation is timely initiation of disease modifying treatment in all patients with confirmed Fabry disease who demonstrate any level of albuminuria, or who have kidney failure, and this has been incorporated into the UK Fabry guidelines [15]. Given that detectable levels of albuminuria and reduced eGFR are associated with faster decline in eGFR and worse outcomes, there is a case for the initiation of disease modifying treatments in Fabry patients who are at higher risk of developing kidney dysfunction.
Evaluating this study within the wider context, our findings agree with the current literature, and show a consistent correlation between declining eGFR and adverse cardiovascular and renal events in Fabry disease [16,17,18,19,20]. Indeed, men, who typically represent the classical and severe phenotype, have greater uACR at baseline (4.7 v 1.86 mg/mmol) and lower eGFR values (100 v 109) than women. During follow-up, male subjects also exhibit a greater decline in eGFR. Furthermore, those who have a faster progression in decline of eGFR also go on to require KRT, with a higher prevalence of Ischaemic heart disease and increased all-cause mortality.
This study is one of the largest cohort studies of Fabry patients that is inclusive of genetic data, medications, baseline co-morbidities and renal outcomes over ten years of follow-up. However, we acknowledge that Fabry disease is a multi-ethnic condition, and a key limitation of our study was that most of our cohort were of White British ethnicity. This study was conducted in accordance with the ethical standards of the institutional committee and with the 1964 Helsinki Declaration and its later amendments. Informed consent was obtained from all individual participants included in the study. No animal studies were conducted as part of this research. Our data encompass more than 20 years, during which treatments have evolved and been modified according to patient response. Consequently, we were unable to distinguish differences in outcomes based on individual disease-modifying therapies. Moreover, smaller subgroup sample sizes render it challenging to draw definitive conclusions to change clinical practice and guidelines; thus, there is scope for future work incorporating larger, multi-ethnic populations.
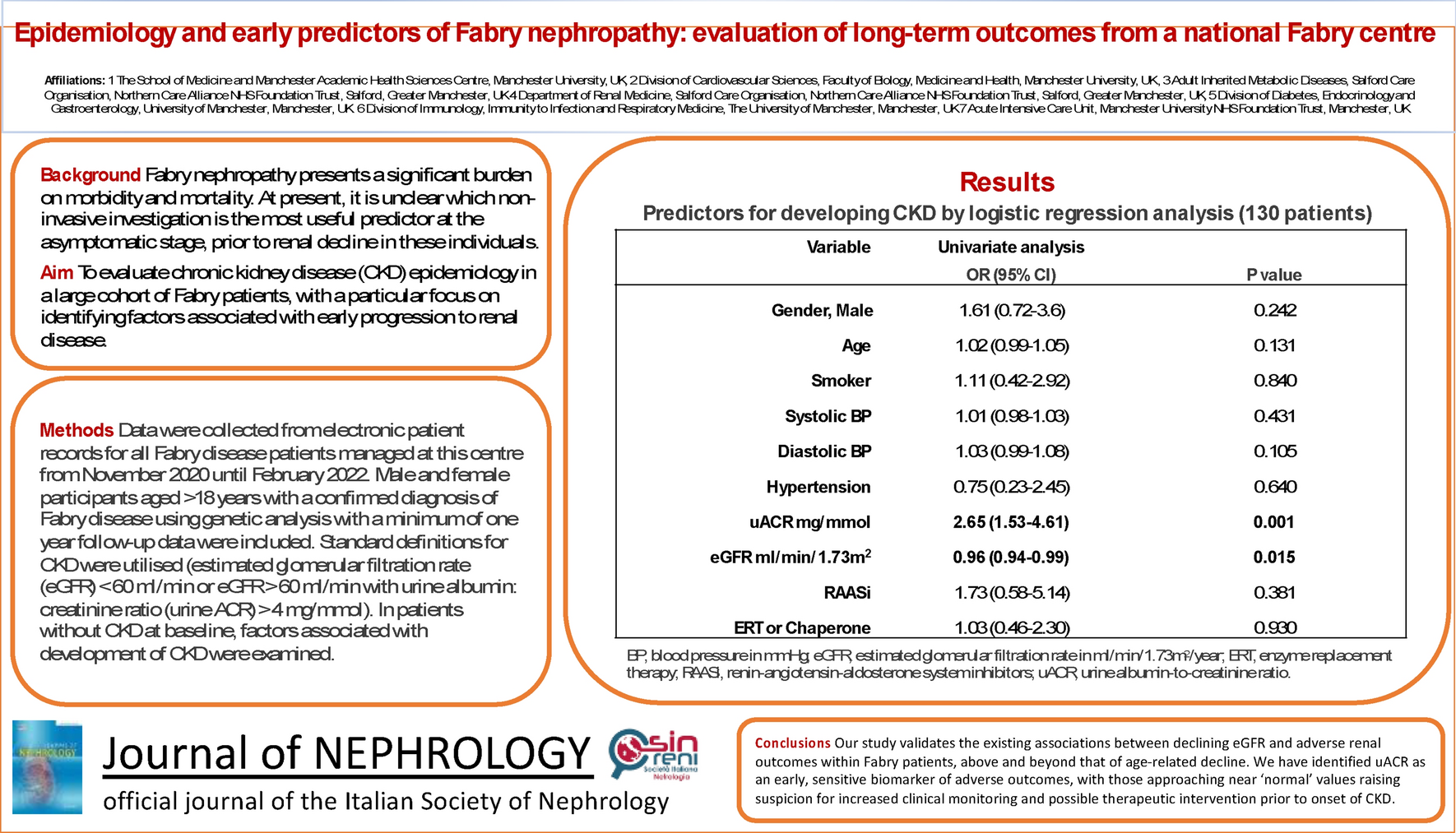
In conclusion, our study validates the existing associations between declining eGFR and adverse renal outcomes within Fabry patients, above and beyond that of age-related decline. We have additionally identified uACR as an early and sensitive predictive biomarker of adverse renal outcomes, with those approaching near ‘normal’ values raising suspicion for increased clinical monitoring and possible therapeutic intervention prior to the onset of CKD.


留言 (0)