
記住我






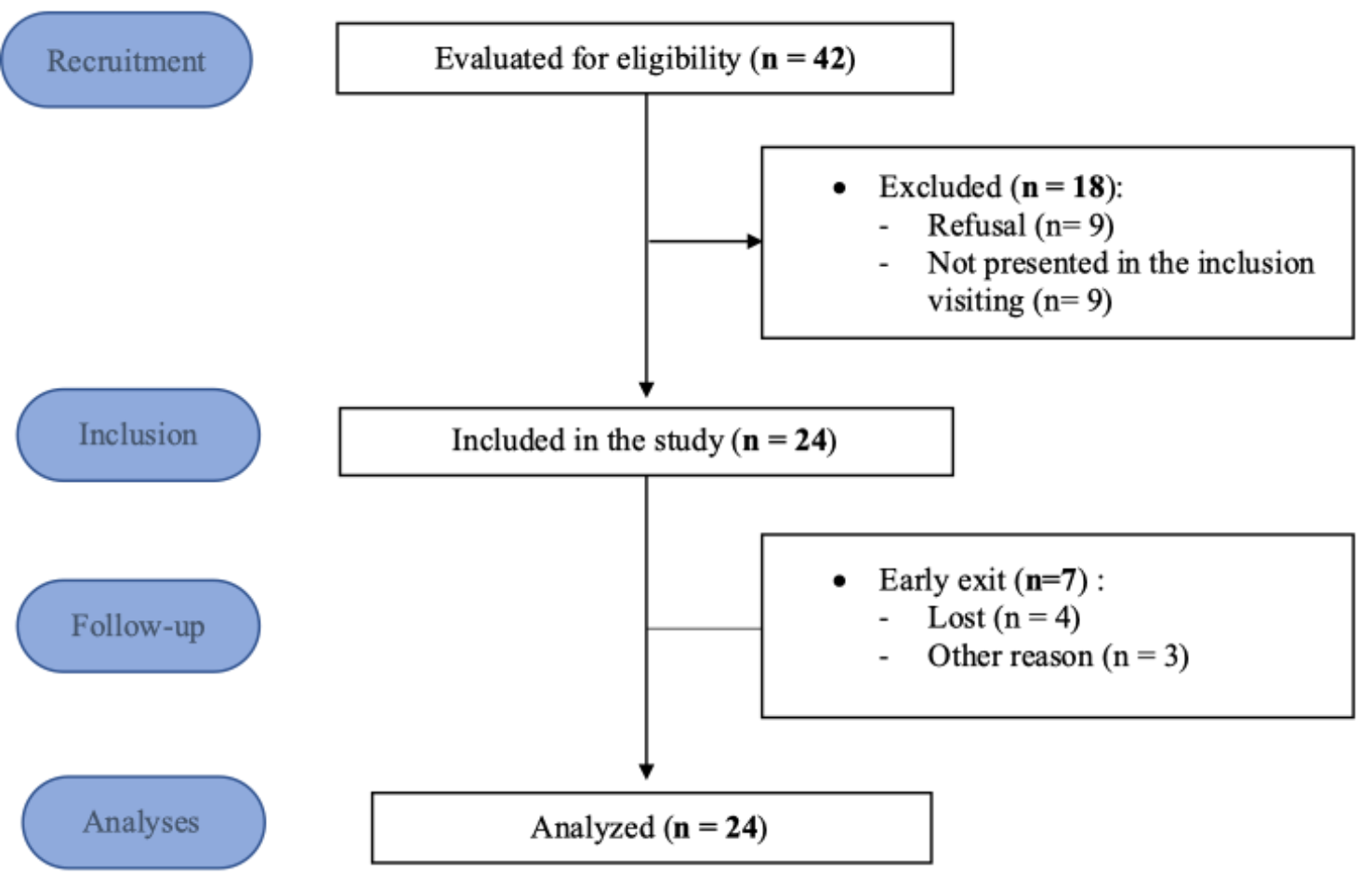
Participants (N = 10) were on average 47.0±10.7 years old. See Table 1 for further demographics information.
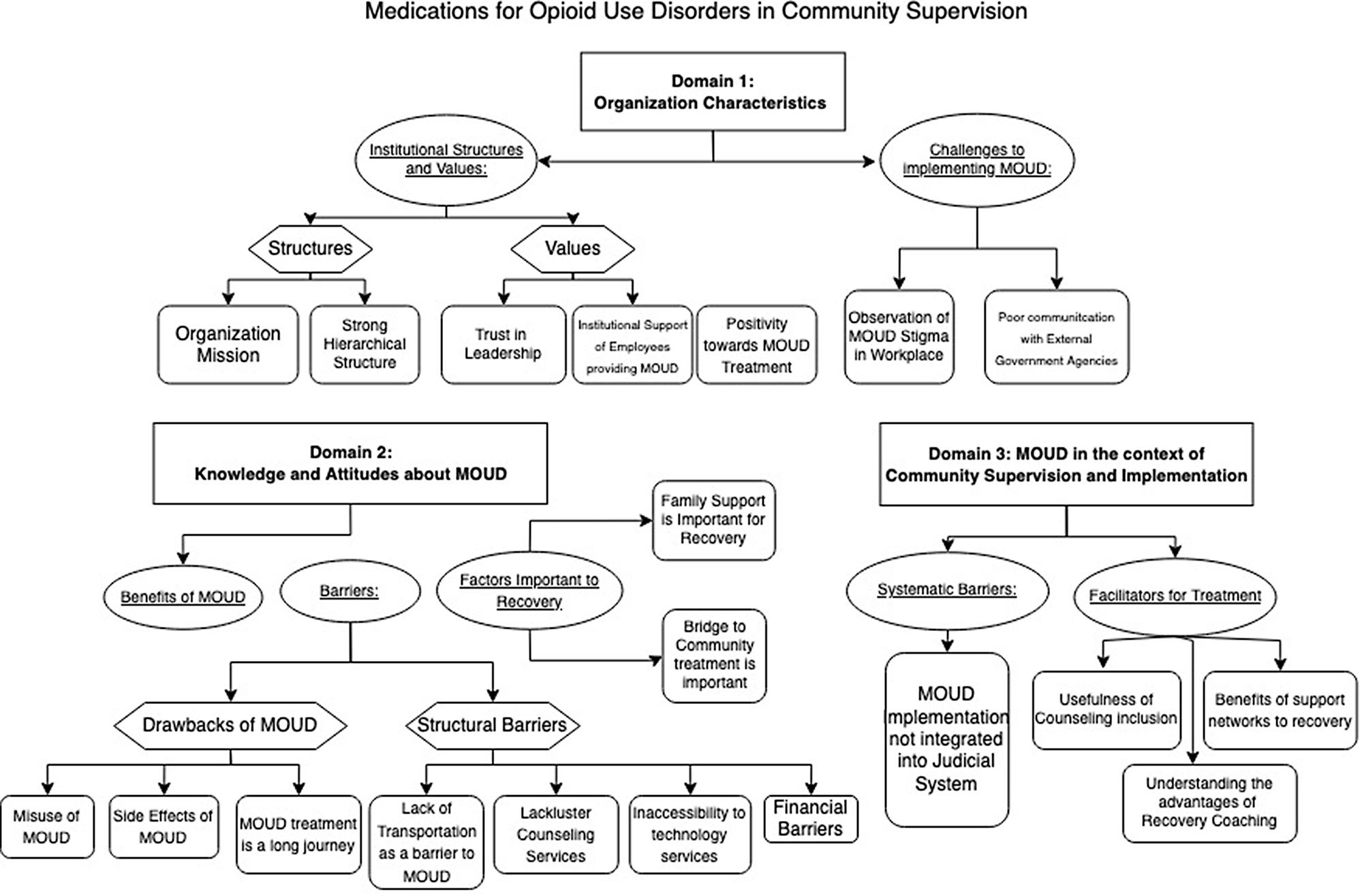
Table 1 Participant DemographicsQualitative analyses revealed a plethora of factors related to MOUD treatment and usage among persons on probation. To help organize our findings, we report individual themes under broad domains around which they cluster (Fig. 1).
Fig. 1
Illustration of Themes and Codes
Domain one: organization characteristicsThe first domain of themes that emerged encompass how characteristics of providers’ organizations influenced MOUD treatment. Participants described how a variety of organizational-level features could both facilitate and hinder MOUD recovery trajectory.
Sub-theme: institutional structuresOrganization missionParticipants identified several organizational characteristics which impacted the use of MOUDs. For instance, the organization mission could facilitate utilization of MOUD for treating MOUD. As one participant described:
I think, in my own words, and not reading from a script, the organization’s mission would be an individualized approach that best serves their needs. So, essentially a patient-centered approach to opiate use disorder. (1009)
Other comments on their organizational mission include an emphasis on community safety and post-release success:
I think the biggest priority is community safety. But the second biggest is offended change and trying to make sure that people succeed when they are either released from or get probation in the court system. (1001)
Strong hierarchical structureParticipants also emphasized how there is a strong hierarchical structure in the department of corrections. For example, one participant said:
It still tends to be a hierarchical situation because the department of corrections does have kind of a semi-military attitude. (1005)
Sub-theme: institutional valuesTrust in LeadershipParticipants describe how employees trust in their organizational leadership in their initiatives/policies.
Yeah, I would say I trust our (leadership). You could call them supportive. They try to think of things help in outreach and stuff like that. (1008)
And
From the higher executive levels from the director’s office, and the executive team up they (are) always looking at a better way to do things and what works and making the necessary changes that we need to do that are appropriate for our department to succeed and do better. (1004)
Institutional support of employees providing MOUDAnother important factor in MOUD usage described by participants was the institutional support of employees in providing MOUD. For example, multiple participants described how their superiors supported them and facilitated them providing care to clients on probation:
I think my colleagues do feel supported (to provide MOUD) from the institutional standpoint. Because everyone is offered the same continuing education, access to conferences and resources as far as that goes. We meet as providers, discuss cases, discuss protocols in terms of how we plan on titrating doses… (1009).
Such efforts by upper management appeared to be a deliberate effort to optimize care for those with MOUD. These anecdotes demonstrate that by creating an open and trusting environment for providers, they could “strategize” the best ways to treat those with MOUD.
As one supervisor described their approach:
…at my site specifically, I try to create an environment where they’re free to talk about their concerns and share problems…How can we make this more productive for everybody? It’s just something that I can do to help as a program director. (1008)
Positivity towards MOUD treatmentParticipants described how their institutions utilized MOUD and are positive towards the use of MOUD when working with people who are incarcerated. For example:
I (think) the addition of MOUD inside the facilities and using that as a model for when they’re released…has made a pretty big difference. (1001)
Sub-theme: challenges to implementing MOUDParticipants also described several factors which could hinder the utilization of MOUD at their organizations. Such factors included forces from both within and outside of their institutions.
Observation of MOUD Stigma in the workplaceDespite the overall positive attitudes towards MOUD, participants also suggested that some stigma towards MOUD also existed within their organizations. One participant described how:
I think that I wish and hope that the community…I’d just like to see the stigma de-stigmatized. It’s heart-wrenching when they come in and they’re either like, “I’m not like the rest of your patients,” or the other day, we had somebody who was like, “Well, I don’t really want to come in every day because I might know somebody.” (1008).
And
I would say some probation officers do not agree with it. They feel like it’s just continued use. They think Methadone is just a poor substitute for the heroin or fentanyl use. They won’t agree to saying that someone completed treatment if they’re in that kind of program instead of a residential treatment program or completing at an outpatient level without using anything. (1006)
Poor communication with external government agenciesAnother barrier to MOUD utilization was potentially poor communication between agencies. Participants described how a lack of communication between organizations made it difficult to coordinate care. For example, through a lack of clear responsibilities between agencies:
Here it’s all their own entities and battles and it’s not a lot of agencies working together as they should, in my opinion. (1003)
Domain two: knowledge and attitudes about MOUDWe examined participants’ knowledge, attitudes, and experiences on/with MOUD.
Sub-theme: benefits of MOUDMost participants described how MOUD is an effective treatment for OUD. This is best represented by the following:
Well, I would imagine that if more people are successful on MOUD, you’re going to have less overdoses. You are going to have less people in need of medical care due to drug use or overdose. If somebody is taking care of themselves…hopefully, that’s going to trickle down to mean less ER visit.. (1004)
Participants also describe that methadone, buprenorphine/naloxone, and injectable extended-release naltrexone are effective methods of MOUD. Unique quotes pertaining to each type of medication is captured below:
Methadone: I think it probably works better for people that feel like they need to go every single day…people that are very or more routine-oriented. And I don’t know if actually going there and getting it every day helps them keep more cognizant of their use or if it’s a support to them, but I think people that probably are at highest risk…would be the benefit of Methadone. (1007)
Suboxone: Suboxone has less restrictions than methadone in regard to prescriptions and amount of medication they can hold on one time. So, if they’re working early hours or something like that, that conflicted with the clinic schedule…it’ll give them that flexibility that they’re looking for to be able to keep their work schedule. (1008)
Vivitrol: I have positive experiences in it working for clients. I feel like it’s less common as say Methadone (1004);
and
He’s been on the Vivitrol for I think two or three years successfully, no relapses. He comes in every four to six weeks, no issues. It’s a good treatment modality, but I think it really just needs to be selected for the right person, and the right person needs to be motivated for it. (1009)
Sub-theme: factors important to recoveryParticipants discussed factors that were important to recovery. The common thread underlying these factors were: (1) that family support was key for recovery, and (2) bridge to community treatment was important:
I think educating offenders’ families (is good), it’s a really broad stakeholder thing, not everybody has to have the same level of understanding, but just enough to know that this is not a harmful thing… family support is really critical. (1002)
And
…From the beginning they talked about wraparound services. We have a strong discharge planning unit, that tries to bridge the gap between incarceration and community. We’re trying to use the continuation of services…so they have appointments when they (get) out. (1003)
Sub-theme: MOUD drawbacks, and barriersParticipants discussed the drawbacks of MOUD, as well as structural barriers to the implementation of MOUD.
Drawbacks of MOUDIn general, participants perceived that MOUD can be misused, their side effects, and that the recovery journey is long.
When MAT[MOUD] first came around…when you hear Methadone, we had a lot of examples of offenders who would be sitting in front of you and they would be dozing off and their eyes would be shutting…they’re just nodding off.so it was not a good experience for us. (1004)
Participants discussed how recovery is a long journey for clients on MOUD. Participants expressed concern that prolonged length time receiving MOUD may indicate that clients were misusing/dependent on MOUD:
I remember her saying, she used to say to her doctor, I don’t want to be on this anymore, I want to be off this, but he would refuse …And then I can remember, she would say that she would wean herself off of it… She didn’t feel supported when she wanted to initially come off it…I want to say that it was a battle to get off it. This was not a six-month process. She was on it for a few years. And I know she wasn’t happy about that. (1004)
Barriers to MOUD uptakeParticipants described barriers to MOUD uptake, including the lack of reliable transportation that was potentially a deterrent to receiving MOUD, lackluster counseling services where MOUD counseling sessions were identified to be short and disengaging for patients, a lack of accessibility to technology services (that potentially can also be seen as a solution to transportation barriers), and financial barriers:
Transport: The worst part about it, especially Methadone, was the fact that he had to go somewhere every morning and get it. So, for those people who didn’t have transportation or had to rely on somebody else for transportation, it was very difficult for some people to get to some of those clinics. (1001)
Counseling: I think more counseling or counselors at these programs are needed. I think they all have very high caseloads, so they don’t spend a lot of time with the offenders, and I don’t think they have as much as an impact on them…I feel like they also need the counseling part… (1006).
Technology Accessibility: Interviewer: In terms of access, transportation is a problem. Do you think that could be resolved by video conferencing technologies? Respondent: Yes. To an extent. With the DOC population, a lot of them don’t … I don’t even have phone numbers for … I have so many homeless people on this caseload and their phone numbers change all the time…technology could be a problem for some. (1007)
Financial Barriers: For methadone treatment specifically…(some patients) are just kind of in this weird bracket where, they make this a little too much to qualify for Medicaid, but they’re not really making enough to really support a monthly premium and then reaching those deductibles and things like that. Some of them… by the time they get the deductible, they could have paid full fee treatment the entire year and never reached the deductible. (1008)
Domain 3: MOUD in the context of community supervision and implementationThe final domain addresses the ways in which knowledge and attitudes towards community supervision influence the implementation and effectiveness of MOUD therapies.
Participants described how the current judicial system may not prioritize MOUD implementation as part of their processes:
Most of the time, it seems like it (MOUD) is done on their (Clients’) own. It’s very rare that somebody is mandated to MOUDFootnote 1. That’s one thing that I have in my experience, I can only think of one person that like part of their parole was to be on Methadone. There are a lot of clients who are on methadone, buprenorphine, naltrexone who are on probation or parole, but I have not necessarily seen that being mandated by the legal system. They will mandate outpatient counseling, mental health counseling and treatment but it’s very rare for MOUD. (1010)
Just as how participants described how there were lackluster counseling services as an adjunct to MOUD, when participants were asked about how counseling can benefit populations in community supervision while on MOUD, they discussed the known benefits of counseling for addiction management:
The benefits are as far as counseling…have always been really beneficial. We do mental health services and medication for mental health, and mental health counseling…majority of the clients are very happy by those services that I’ve provided. (1010)
Participants also discussed the potential benefits of peer support specialists, such as the formation of a personal connection to someone with similar lived experience:
A lot of them are recovered addicts… It’s not on so much of a professional level but it’s more on where the person’s at, more at their level. But they will reach out and keep reaching out and engage with the person and be there for the person. (1007)
Social support was further highlighted to have a beneficial and critical role for the success among individuals on probation and MOUD.
I think support from all levels, from the treatment agency, from your family, from your Probation Officer, from whatever counselor you’re seeing…from every single agency that you deal with, you need support. (1001)
留言 (0)