
記住我
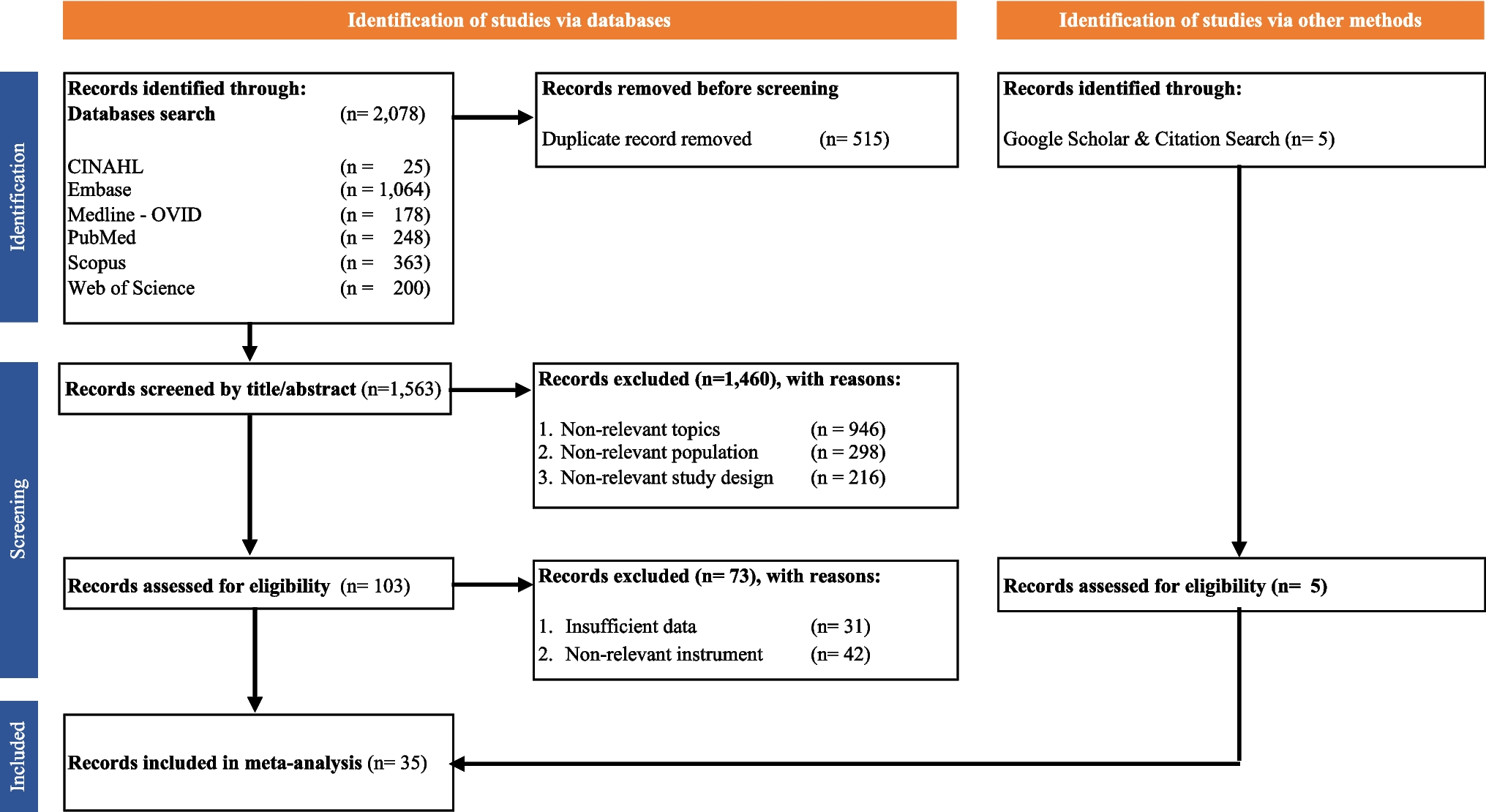
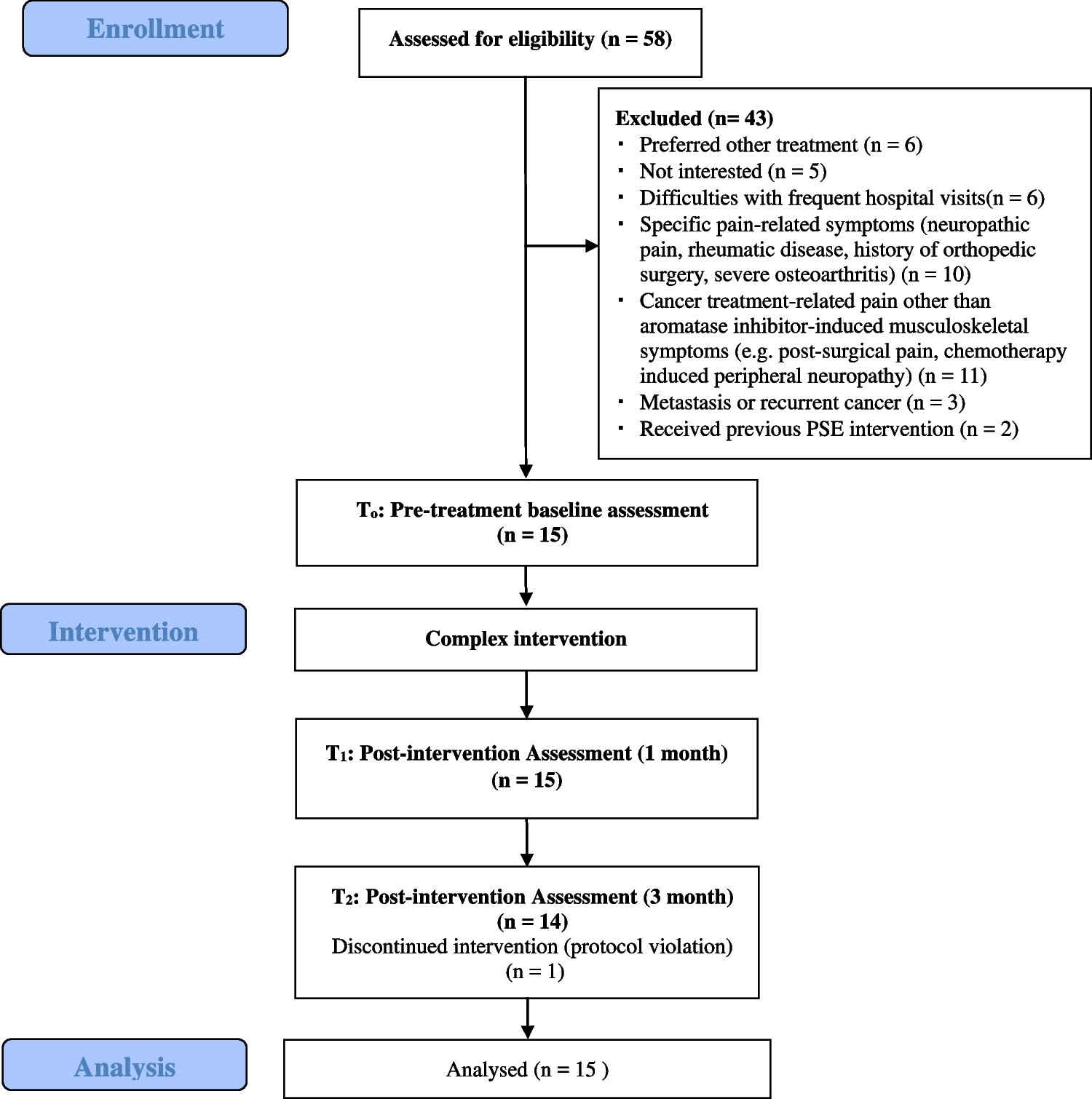
The search yielded 3716 studies. After title and abstract screening and removal of duplicates, 113 abstracts were retrieved for full-text evaluation. After examining full text, 84 publications were retained. Figure 1 shows the PRISMA flowchart of the study selection process. Sample and intervention characteristics are summarised in Fig. 2. Study characteristics are detailed in Supplemental Materials 3.
Fig. 1
PRISMA flow diagram including screening and reasons for exclusion during second round of title and abstract screening
Fig. 2
Distribution of peer-reviewed studies reporting non-pharmacological supportive care interventions of people with advanced cancer: 2013 to 2023
Sample characteristicsSample sizeThe sample size of the studies ranged from 6 to 349 participants, with a mean of 76 participants. The mean age of participants was 61.3 years. Eleven studies (13.1%, n = 11) had all female participants, 6 studies (7.1%, n = 6) had all male participants, and 67 studies (79.8%) included men and women. One study did not identify whether participants were male or female [26].
Cancer typeForty-five studies focused on a single cancer type, including lung cancer (16.7%, n = 14), breast cancer (14.3%, n = 12), prostate cancer (7.1%, n = 6), melanoma (4.8%, n = 4), gastrointestinal tract cancer (3.6%, n = 3), colorectal cancer (3.6%, n = 3), ovarian cancer (2.4%, n = 2) and nasopharyngeal cancer (1.2%, n = 1). A population of mixed cancer types was the most common overall (46.4%, n = 39).
Study designStudy typeStudy designs included randomised controlled trials (RCTs) (73.8%, n = 62), single-arm interventional studies (15.5%, n = 13), mixed methods studies (3.6%, n = 3), two-arm interventional studies (2.4%, n = 2), retrospective clinical control trials (CCT) (2.4%, n = 2) and pilot studies (2.4%, n = 2).
Study settingsIntervention settings were varied and, in some instances, included multiple locations (6%, n = 5). Single-intervention locations include hospitals (45.2%, n = 38), outpatient clinics (16.7%, n = 14), participant homes (15.5%, n = 13), academic settings (9.5%, n = 8), gym or exercise area (4.8%, n = 4) and hospice (2.4%, n = 2).
Study lengthThe average intervention duration was 10 weeks, with a range of 3 days to 56 weeks.
Study mode of deliveryStudies were conducted in person (83.3%, n = 70), online (14.3%, n = 12), or a combination of both (2.4%, n = 2). Interventions were conducted individually (89.3%, n = 75), through group interventions (95.2%, n = 8), or a mix of both (11.9%, n = 1).
Intervention types and outcomesMost studies investigated a single intervention (92.9%, n = 78) and six studies (7.1%, n = 6) investigated multi-modal interventions. Only 34 studies (40.5%, n = 34) reported adverse events. Of these, most recorded no adverse events (33.3%, n = 28) or fatigue or distress directly related to the intervention (7.1%, n = 6). Thirty-two studies (38.1%, n = 32) showed statistically significant improvements in investigated interventions addressing psychosocial and physical supportive care needs through improvements in symptom burden and quality of life. Only one study reported adverse events as a primary outcome [27].
Physical activity–based interventionsTwenty-six studies (31%, n = 26) focused on physical activity–based interventions alone, with twenty-one RCTs, three single-armed interventional studies and two two-armed interventional studies [28, 29]. Interventions included endurance [30, 31], strength [32] and resistance training [29, 33] with thirteen studies using more than one type of physical training (15.5%, n = 13) [26, 28,29,30, 32, 34,35,36,37,38,39,40,41]. Two studies explored isometric training of vertebral muscles [42, 43]. Other modalities included aerobic exercise [44, 45], very low interval training [46], walking interventions [47] and multifaceted programs prompting patients to exercise via text messages [48].
Two studies (2.4%, n = 2) investigated the feasibility of yoga interventions to improve quality of life. A couples-based Vivekananda Yoga (VKC) was tested in a single-armed feasibility trial on patients and their caregivers, assessing pre- and post-intervention levels of fatigue, sleep disturbances, psychological distress and relational closeness [49]. The other was an RCT focusing on mindful yoga techniques [50].
Of the twenty-six studies investigating physical activity–based interventions, certain studies demonstrated improvements in activity levels [29, 41, 48, 51], strength [30, 38], mobility [32], endurance [30] and reductions in pain and fatigue [38, 39]. High adherence rates were observed in programs suggesting feasibility and acceptability [34, 39]. Some interventions [35, 50] showed no significant change in fatigue, suggesting limited efficacy in addressing this symptom (p > 0.05). Multidimensional interventions [36, 41] provided further insight into exercise capacity improvements, highlighting the potential benefits of these interventions (p < 0.05). Further studies [26, 43] highlight the importance of high completion rates in attaining positive outcomes. Mixed findings and negative outcomes were also evident including challenges in recruitment and participation [46, 52].
Primary outcomes for the twenty-six studies investigating physical activity–based interventions, included activity levels [29, 41, 48, 51], strength [30, 38], mobility [32], endurance [30], lung capacity [36, 40], quality of life [26, 28, 42, 44] as well as reductions in pain and fatigue [26, 38]. Of the eight studies reporting feasibility, feasibility primary outcome criteria were completion rates [39, 43], adherence and attendance [34, 45, 46], adverse events [33] and satisfaction [47, 53].
Psychosocial-based interventionsPsychosocial-based interventions include targeted interventions that address fear of cancer recurrence, mindfulness and distress through approaches such as cognitive behaviour therapy (CBT). Twenty studies (29.8%, n = 25) investigated psychosocial-based interventions, including fourteen RCTs, four single-armed interventional studies, one single-arm mixed methods study and one retrospective study. These programs reported significant reductions in depression [54,55,56], spiritual well-being [57, 58], death-related distress [55, 59, 60], sleep [61] and physical symptom distress [62,63,64]. Feasibility studies reported on satisfaction [52], acceptability[65] and adherence [66].
CBT protocols were used in six studies for patients with insomnia, anxiety, depression and fatigue [52, 54, 61, 66,67,68] including CBT via a mobile app to improve anxiety, depression and quality of life [67]. Acceptance and Commitment Therapy (ACT) was investigated for functional well-being and fatigue in sessions conducted in-person or via telephone [61, 69]. One study focused on the combined effect of CBT and ACT on the impact on insomnia [61]. Other modalities applied Meaning-centred Psychotherapy (MCP) to address existential distress and spiritual well-being [58]. Several interventions aimed to reduce cancer-specific distress and improve quality of life including Cognitive Behavioural Stress Management (CBSM), ACT [61,62,63, 70] and Managing Cancer and Living Meaningfully (CALM) [56, 71, 72]. One study investigated logotherapy to help individuals acquire meaning in their lives [60] while Dignity Therapy (DT) [59, 73] was used to encourage self-reflection as a means to achieve spirituality and identify a purpose in life.
CBT-based interventions were associated with improved mood and quality of life, particularly for those with insomnia and fatigue (7.1%, n = 6). Significant improvements in fatigue were noted with at-home delivered CBT intervention [52]. A study that delivered CBT via a mobile app also found significant improvements in anxiety, depression and quality of life when compared to baseline [67]. A CBT feasibility study reported high adherence to lessons (70%) accompanied with high treatment satisfaction [66]. CBT sessions delivered concurrently with chemoradiotherapy also demonstrate lower depression and anxiety scores twenty-four months after completion [74]. CBT focusing on ACT reported significant improvements in sleep efficiency, sleep latency, worry and depression from baseline to 6 weeks [61]. CBT focusing on stress reduction and management reported fewer depressive symptoms, intrusive thoughts and improvements in emotional wellbeing [72].
Two feasibility studies (2.4%, n = 2) investigated interventions for fear of cancer recurrence. One acceptability and feasibility RCT (Fear-Less: A Stepped-Care Program) stratified participants according to need to individual sessions delivered by a clinical psychologist or to a self-management group, compared to usual care [65]. In the self-management group, 13/21 participants had a reduction of Fear of Cancer Recurrence (FCR) and 5/7 participants in the individual psychologist session group. The stepped-care intervention was found to be acceptable and feasible. The other study was a nurse-led single-armed mixed methods study exploring the feasibility of a fear-conquering videoconferencing sessions. The intervention met feasibility and acceptability criteria with a reduction score of 8 points and 19.1 points for fear of progression and cancer-related distress respectively [75].
留言 (0)