
記住我


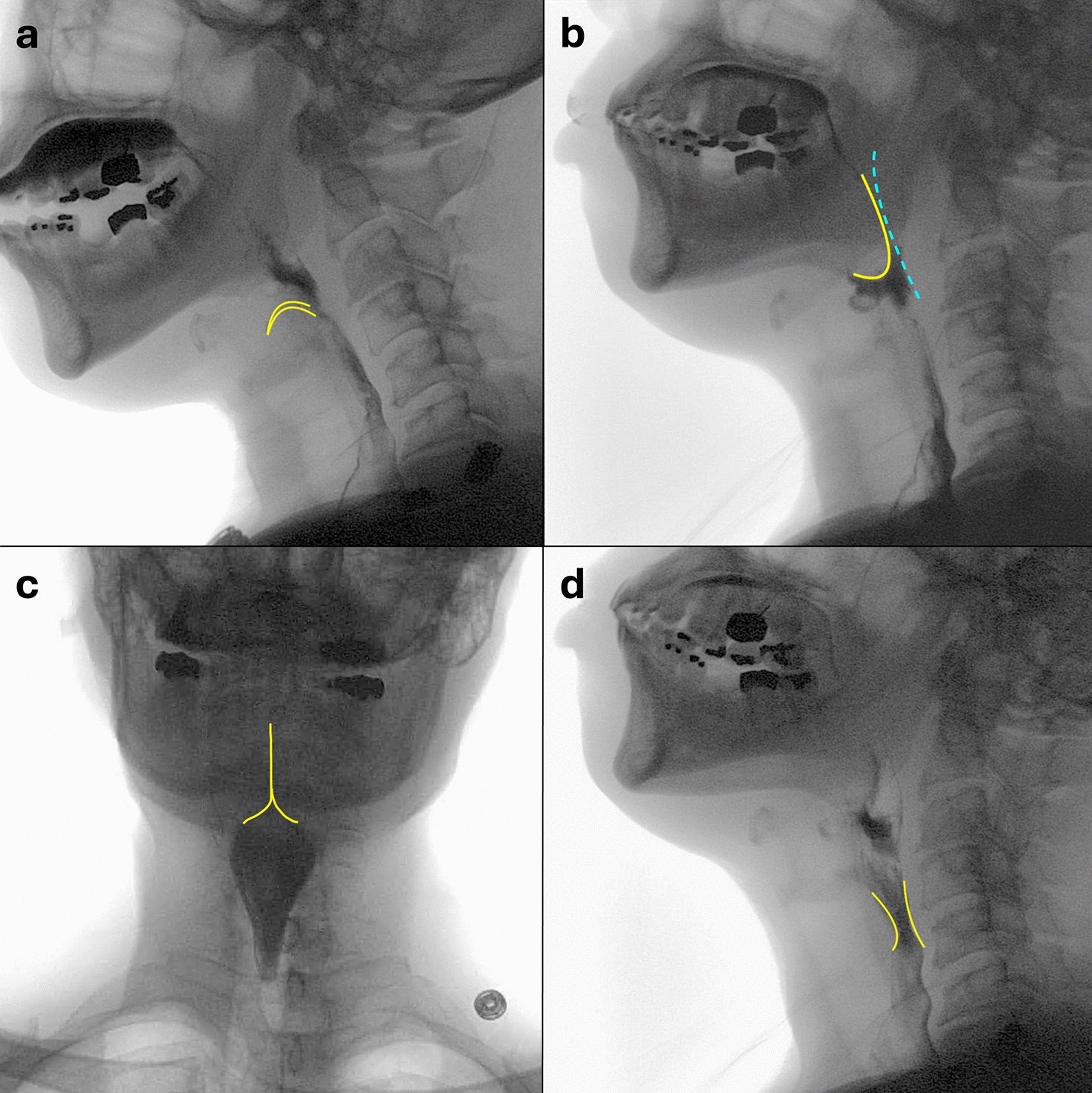


The role of the radiologist during a MBSS is multifaceted and includes to be able to accurately detect functional and structural abnormalities. It is important for the radiologist to be familiarized with key anatomical landmarks of the pharynx (Fig. 2a, b). The pharynx is divided into the nasopharynx, oropharynx, and hypopharynx. The nasopharynx is bound inferiorly by the soft palate and the oropharynx is bound inferiorly by the hyoid bone or base of the epiglottis, with the pharyngoepiglottic fold is its true dividing landmark. The tongue base extends from the mouth to the valleculae. The epiglottis is superior and posterior to the valleculae. The hypopharynx includes the piriform sinuses which are the lateral boundary of the hypopharynx and extends to the cricoid cartilage [34, 35].
Fig. 2
Lateral and AP images of the pharynx demonstrating typical anatomy encountered during a MBSS. a. Tongue base, b. Epiglottis, c. Vallecula containing a small amount of residual barium, d. Hyoid bone, e. Laryngeal vestibule coated in barium, consistent with laryngeal penetration, f. Piriform sinuses containing a small amount of residual barium, g. Vocal cords coated in barium, h. Barium coating the anterior aspect of the trachea, consistent with tracheal aspiration
Airway penetrationDuring the MBSS, the radiologist and SLP should assess for functional and structural abnormalities in the oral, pharyngeal, and esophageal phases of swallowing [24]. While the presence of laryngeal penetration and tracheal aspiration should be assessed, the cause for the airway penetration should also be determined. Airway penetration may occur prior to, during, or after the swallow. Laryngeal penetration occurs when contrast enters the laryngeal vestibule and tracheal aspiration occurs when contrast enters the trachea. A widely applied metric for grading the degree of airway penetration and the patient’s response is the Penetration-Aspiration Scale [32]. When aspiration or penetration are detected, the SLP may perform compensatory swallow strategies to minimize or improve the degrees of penetration or aspiration, including chin tuck, head turn, or breath-hold maneuvers.
It is anticipated that dysphagic patients may aspirate during a MBSS, as one of the primary objectives of the study is to identify and address the underlying causes of airway invasion. The customized barium contrast used in a standardized protocol is administered in small, controlled amounts. It is non-water soluble, thereby reducing the risk of chest infections. However, efforts should be made to minimize the volume of aspiration while maximizing the diagnostic value of the study. A key question that radiologists and speech pathologists face is: "How much aspiration is too much?"—a point at which the study may need to be discontinued. A patient's tolerance to aspiration varies depending on individual clinical circumstances. For instance, frail elderly patients with limited mobility and a non-productive cough may be at higher risk for developing chest infections due to chronic microaspiration. In contrast, more physically active patients, such as those recovering from head and neck cancer, who retain strong respiratory defenses, may tolerate routine aspiration during eating and drinking without progressing to aspiration pneumonia. Thus, there are no rigid stopping rules for MBS based solely on the amount of aspiration. Instead, a careful balance must be struck between the clinical condition of the patient and the sufficiency of the information obtained for accurate diagnosis and treatment planning. This decision is best made collaboratively by the examiners based on the individual patient’s clinical presentation.
Structural abnormalities in the pharynx and cervical esophagusWhile there is a wide range of functional abnormalities impacting pharyngeal swallowing, there are many structural abnormalities that may be encountered during an MBS exam.
The cricopharyngeal musculature is an important demarcation at the pharyngoesophageal junction and makes up the upper esophageal sphincter. It consists of the inferior constrictor muscle, the cricopharyngeal muscle, and circular fibers of the proximal cervical esophagus. The cricopharyngeus is closed between swallows and relaxes upon swallow initiation to allow the bolus to pass from the pharynx into the cervical esophagus [34]. A prominent posterior indention may be seen at the level of the cricopharyngeus and if mild, may be within the realm of normal or not clinically signification. However, if the cricopharyngeal “bar” results in significant luminal narrowing, it may result in dysphagia (Fig. 3a).
Fig. 3
a Lateral image shows a cricopharyngeal bar (arrow) that narrows the cricopharyngeal junction by approximately 50%. b Lateral image shows a Zenker’s diverticulum (arrow) posterior and superior to the narrowed cricopharyngeus. c Oblique image shows a Killian–Jamieson diverticulum arising inferior to the cricopharyngeus and extending in an anterior and lateral fashion. d AP image demonstrates a thin cervical esophageal web (arrow). e Lateral image shows a post cricoid defect (arrow), a normal finding along the anterior aspect of the hypopharynx. f Large anterior cervical osteophytes (arrow heads) prevent inversion of the epiglottis (arrow)
A Zenker’s diverticulum (Fig. 3b) is thought to form as a result of pulsion forces through an anatomic weak point (Killian’s dehiscence) at the pharyngoesophageal junction. This forms due to cricopharyngeal dysfunction which creates elevated intraluminal pressure [34, 36]. A Zenker’s diverticulum is located posteriorly or slightly to the left of midline and superior to the cricopharygeus. A Zenker’s diverticulum can be a source of food stasis that may cause multiple symptoms and complications, including dysphagia, halitosis, cough, and aspiration. Since the Zenker’s diverticulum is thought to arise from failure of the cricopharyngeus to relax, treatment is aimed surgical correction of the diverticulum along with a cricopharyngeal myotomy [37].
A Killian-Jameson diverticulum (Fig. 3c) protrudes through a muscular gap in the anterolateral wall of the proximal cervical esophagus, inferior to the cricopharyngeus [36]. Killian-Jameson diverticula are thought to form through this sidewall weakness, also known as the Killian-Jamieson space [35, 36]. Killian-Jameson diverticula are smaller and less common that Zenker’s diverticula [36]. Most are asymptomatic and rarely require treatment.
An esophageal web (Fig. 3d) is a thin membranous structure that can occur anywhere in the esophagus, but most commonly occurs in the cervical esophagus [38]. Most are considered idiopathic but can be seen in association with gastroesophageal reflux and Plummer-Vinson syndrome. The symptoms in patients can vary based on the degree of luminal narrowing caused by the web. On a barium swallow, a web appears as a thin (2–4 mm) transverse linear filling defect in the cervical esophagus along the anterior wall and often circumferentially. Cervical esophageal webs should not be mistaken for a normal post cricoid defect (image 3e). Post cricoid defects are caused by redundant mucosa or a submucosal venous plexus along the anterior wall of the hypopharynx that changes morphology upon swallowing [39, 40].
Anterior cervical osteophytes are common, and can occasionally be a cause of dysphagia predominantly through direct hypopharyngeal or esophageal compression, inflammation, or nerve impingement. Osteophytes/syndesmophytes in diffuse idiopathic skeletal hyperostosis (DISH) of the cervical spine may also result in pharyngeal dysphagia (DISHphagia) and may prevent inversion of the epiglottis which increases the risk for aspiration (Fig. 3f) [39]. Management of symptomatic cases typically involves conservative approaches such as anti-inflammatory and analgesic medications, postural adjustments, and dietary modifications. When these conservative measures prove insufficient, surgical resection of the osteophytes may be pursued, which has been shown to improve quality of life in some patients [41].
Cervical soft tissue assessmentPrevertebral soft tissue thickening (Fig. 4a and b) is a non-specific finding with a broad differential, including infection (such as retropharyngeal abscess), inflammation (e.g., longus colli calcific tendinitis), congenital conditions (like an abnormal retropharyngeal carotid artery course), as well as acute traumatic injuries and post-operative causes such as a hematoma and/or post-operative edema. Since this region is included in the field-of-view for MBSS studies, it should be routinely evaluated, as it may account for the etiology of the patient’s symptoms [42]. Amongst adults, the prevertebral soft tissue thickness at C2 should measure ≤ 7 mm or half of the vertebral body width, and at C7 it should be ≤ 22 mm or the width of the adjacent vertebral body [43]. Given the wide variety of causes for prevertebral soft tissue thickening, it is important to use correlative imaging studies to determine the potential etiology. In the absence of correlative imaging or relevant history (e.g., recent cervical spine fusion surgery), additional imaging may be warranted.
Fig. 4
Abnormal prevertebral soft tissues on MBSS in 3 separate patients. A First patient, 1-day post-anterior cervical discectomy and fusion (ACDF) complaining of dysphagia. Prevertebral soft tissue thickening is present anterior to the fusion hardware (arrow). Laryngeal flash penetration is subtly present as well (arrowhead). On follow-up MBSS performed 6 days later (not shown), the soft tissue thickening had significantly decreased and no laryngeal penetration or aspiration was demonstrated. In the absence of an underlying fluid collection, prevertebral soft tissue swelling after ACDF will usually peak around 2–4 days and then gradually improves/decreases, resolves within 6 weeks. B Second patient complaining of neck pain and dysphagia, without recent surgical or trauma history. Prevertebral soft tissue thickening is present (arrow). Further clinical and imaging evaluation was recommended, which revealed discitis osteomyelitis due to methicillin-susceptible Staphylococcus aureus. C Third patient with history of asthma complaining of chest and neck pain, as well as dysphagia. Subtle linear lucency tracking along the prevertebral soft tissues (arrows), consistent with retropharyngeal emphysema. Chest radiograph demonstrated pneumomediastinum (not shown). Acknowledgement: Cases 2 and 3 are courtesy of Dr. Sarah Shaves, Eastern Virginia Medical School
Similar to prevertebral soft tissue thickening, the presence of extraluminal gas (Fig. 4c) within the soft tissues of the head and neck observed during MBSS studies can result from various causes. These include head and neck infections, recent surgery, and conditions that originate in the thoracic region and ascend through the communicating fascial planes [44]. Identifying the etiology is crucial because some of these conditions can be life-threatening and may require immediate surgical intervention. Thus, careful evaluation and correlative imaging studies are essential for accurate diagnosis and timely management.
Cervical soft tissue densities can include normal calcifications associated with the aging process, evident in structures such as laryngeal cartilage and adjacent ligaments [43]. In contrast, certain densities may reflect pathological conditions, such as carotid artery calcifications or the presence of foreign bodies. Carotid calcifications can be indicative of an elevated stroke risk and may affect both treatment responses and patient prognosis. Although rare in adults, foreign body ingestion poses significant risks, potentially leading to severe complications like laryngeal and/or pharyngeal injuries, which can result in critical outcomes such as abscesses or mediastinitis. Consequently, precise diagnosis of foreign bodies is crucial, and should be included in the differential of cases of unexplained prevertebral soft tissue swelling and/or soft tissue gas [43, 45].
Squamous cell carcinoma (SCC) of the larynx and complicationsSquamous cell carcinomas (SCC) comprise the vast majority of primary malignancies in the head and neck and may arise from the supraglottic larynx (extending from the epiglottis to the true vocal cords), glottis (true vocal cords), or subglottis (extending from the inferior surface of the true vocal cords to the cricoid cartilage) [46]. Laryngeal SCC most commonly arises in the supraglottis or the glottis region and less commonly in the subglottis (Fig. 5a) [46]. Risk factors include alcohol use, tobacco, and chronic gastroesophageal reflux. Symptoms include dysphagia, hoarseness, odynophagia, otalgia, and bleeding. The imaging appearance of these tumors vary from exophytic, nodular surface irregularity for well-differentiated tumors, to ulceration of the pharyngeal wall which can occur with poorly differentiated tumors [46]. Treatment of SCC involves a multidisciplinary approach consisting of chemotherapy, radiation, and surgery. Early-stage cancers are amenable to vocal-cord sparing surgery and other conversation laryngeal surgeries.
Fig. 5
a Lateral image of a modified barium swallow demonstrates an irregular mass centered at the epiglottis and extending to the larynx which was later proven to be a squamous cell carcinoma (arrows). b This patient had a prior history of laryngeal squamous cell carcinoma and underwent total laryngectomy with free flap reconstruction. This AP image demonstrates an irregular stricture (arrow) along the right lateral aspect of the distal end of the neopharynx that was proven to be secondary to squamous cell carcinoma recurrence. c A band of scar tissue or “pseudoepiglottis” (arrow) at the tongue base after total laryngectomy. If the pseudoepiglottis impedes the flow of liquid and food, then it may lead to formation of a diverticulum proximal to it. Long segment benign stricture (dashed arrow) is also present throughout the neopharynx in this patient that was likely secondary to a post radiation stricture. d This patient had a history of laryngeal squamous cell carcinoma and underwent a total laryngectomy with free flap reconstruction. A TEP was placed for voice restoration (white arrow), and the patient subsequently complained of coughing upon swallowing. Black dashed arrow shows leakage of barium through the TEP resulting in tracheal aspiration
For locally advanced cases, a total laryngectomy may be performed, which involves resection of the hyoid bone, cricoid and thyroid cartilages, vocal folds and epiglottis, with closure and reconstruction of the anterior defect with muscle and skin [34, 47]. On MBSS, the neopharynx appears as a featureless tube extending from the base of the tongue to the cervical esophagus [34]. Complications can occur with total laryngectomy cases such as benign strictures, malignant strictures (Fig. 5b), and pharyngocutaneous fistulas. Following total laryngectomy, a “pseudoepiglottis” may form as a result of scar tissue developing at the tongue base that may enlarge over time due to the pull of the tongue and the pharyngeal constrictors as the patient swallows (Fig. 5c) [48]. This may narrow the entrance to the neopharynx and obstruct transit of the bolus, leading to formation a diverticulum [47, 48].
After total laryngectomy, one of the major challenges a patient encounter is loss of voice. Patients may undergo voice rehabilitation, with placement of a tracheoesophageal prosthesis. The tracheoesophageal prosthesis (TEP) is a one-way valve device which is positioned between the trachea and esophagus. When the patient covers the tracheostomy and exhales, air is forced through the TEP through the esophagus which then vibrates and produces sound. Typically, there is a low rate of complications, but occasionally complications do occur. If the TEP is too small, it could cause leakage around the prosthesis (Fig. 5d). If it is too large, then it may cause obstruction of the esophagus and impairment in phonation. The TEP may dislodge and can be aspirated.
留言 (0)