Given the disadvantages of ICGA and EDI-OCT, alternative approaches to assessing the course of VKH disease are needed. In this study, we assessed the clinical value of the automated measurement capabilities of SS-OCT to measure choroidal thickness (quantitative approach) in the follow up of patients with chronic VKH (convalescent and quiescent patients). We found that choroidal thinning and improved vision were associated with treatment, while increasing thickness and worsening vision were associated with posterior relapse. During follow-up, increases in choroidal thickness and worsening VA were associated with posterior relapse. Overall, 41.6% of asymptomatic (no changes in visual acuity) recurrences in the convalescent group and 25% in the patients with quiescent VKH were detected by SS-OCT. Importantly, in the recurrent VKH group, 14.6% of relapses were also asymptomatic and in the quiescent VKH group 25% of the relapses were asymptomatic. By contrast, all relapsed eyes showed signs of inflammation on ICGA. Moreover, we found the importance of measuring extrafoveal choroidal thickness as well to detect recurrences. Our findings suggest SS-OCT may be a valuable adjunct to ICGA to detect posterior segment recurrence and to evaluate treatment response in patients with VKH disease [20, 21]. All recurrences diagnosed with tomography showed signs of inflammation on ICGA. These results are consistent with a previous study by our group in patients with acute VKH [22] in whom no changes in VA were observed in over half of eyes in which relapses were diagnosed by SS-OCT. Finally, these results are also in line with several other previous studies [19,20,21].
We and several other groups [22, 23, 26,27,28] have found that choroidal thickening, which may be related not only to inflammatory infiltration but also to increased exudation18, is often but not exclusively found in acute VKH. The results of the present study suggest that chronic relapsing cases also present choroidal thickening. An important advantage of the present study and the aforementioned studies is that those studies did not evaluate choroidal thickness over time as a follow-up measure.
We hypothesized that we could use SS-OCT to measure changes in choroidal thickness to detect posterior relapses. In asymptomatic patients with recurrent VKH, the first sign of relapse was an increase in choroidal thickness (detected by SS-OCT) without loss of VA (all relapses were confirmed with ICGA). Thus, although ICGA is necessary to confirm the relapse, SS-OCT can detect recurrent disease without the need for this invasive, time-consuming procedure. Moreover, while ICGA provides a qualitative diagnosis of choroidal inflammation, SS-OCT yields an objective, quantitative diagnosis of that inflammation (evidenced by the increase in choroidal thickness). Notably, personalized follow-up with SS-OCT scanning allowed us to diagnose pathologic increases in choroidal thickness in all eyes with posterior recurrences (even asymptomatic ones), all of which were subsequently confirmed by ICGA. These results are in line with the findings of our previous study [22] in acute patients, in which SS-OCT was used to detect asymptomatic posterior recurrences, similar to previous reports [22, 23, 27, 28, 30,31,32,33].
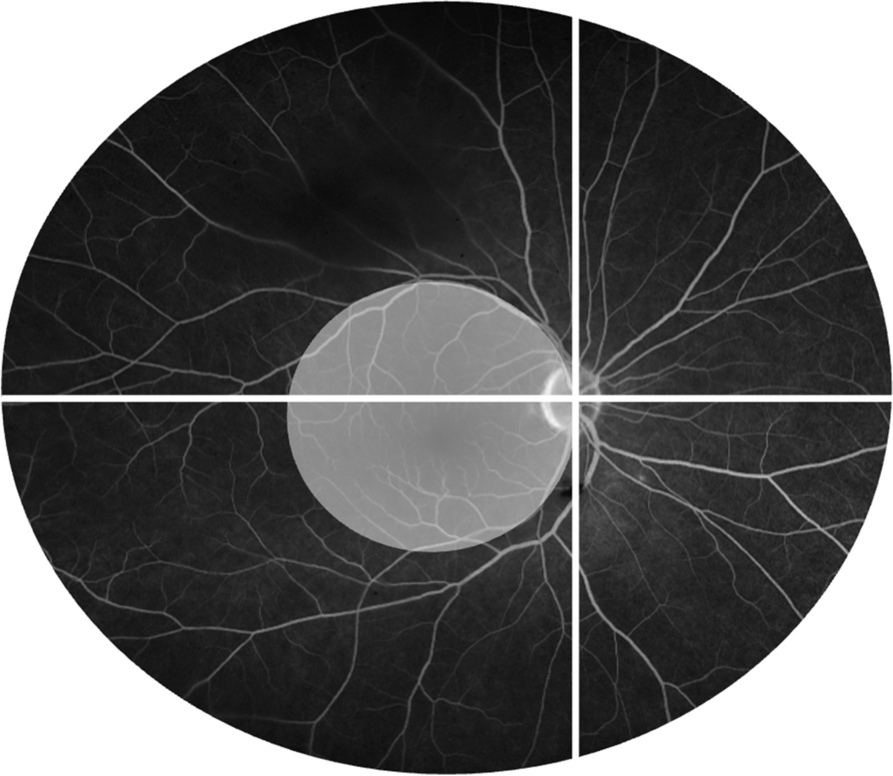
The tendency for choroidal thickness to decrease in convalescent/chronic VKH patients has been described by several other authors [19, 23, 30, 34]. In our study, the decrease was seen after relapse, but we found no significant differences between choroidal thickness at baseline and at study end in either the relapsed or quiescent groups, indicating that these relapses did not affect choroidal thickness. However, in quiescent patients, choroidal thickness was significantly thinner than in controls at both the baseline and final evaluation. Furthermore, we are unaware of other articles having published any cases of choroidal thickening starting from such thin choroids as the ones illustrated in Fig. 4. It was previously thought that thin choroids could not thicken pathologically even in the event of inflammation, or that even if they thickened, they could not surpass the thickness of a healthy choroid. Nevertheless, this case shows how even an extremely thin choroid can thicken up to 435 µm during a relapse. Interestingly, this case also shows how despite noteworthy choroidal thickening, VA was unaffected. It also exemplifies how posterior relapses do not necessarily have to involve the foveal region. Therefore, it is imperative to determine choroidal extra-foveal thickness using SS-OCT to detect any possible asymptomatic relapses.
Nakayama et al. [26] evaluated eight patients with a recent diagnosis of VKH. In that study, the authors measured choroidal thickness manually with EDI-OCT, defining a recurrence as an increase in choroidal thickness > 100 µm from previous measurements. In our study, we defined the relapse as the minimum increase in thickness required to induce a decrease in VA and the presence of inflammatory signs on ICGA, or without any loss of vision but with an increase ≥ 50 µm in choroidal thickness combined with the presence of inflammatory signs on ICGA. The 50 µm cut off point was based on the mean SD in the various published studies [8, 10, 30, 35]. Nakayama and colleagues found that VKH patients had an increased SFCT at baseline, with a mean increase of 578 μm vs. 666.9 μm in acute patients in our previous study [36]. By contrast, baseline SFCT in the present study was within the normal range in healthy controls (302.3 μm); 302 μm in the relapsing group and 243 μm in the quiescent one. Nakayama et al. also found that choroidal thickness decreased with treatment, consistent with our findings. However, they also found a rebound in choroidal thickening in three patients (5 eyes) during corticosteroid tapering but without evidence of increased inflammation (at one year follow-up with manual measurements). By comparison, in our study, five patients (10 eyes) in the acute group, five patients (10 eyes) in the recurrent group, and one patient (one eye) in the quiescent group presented asymptomatic relapses. We suspect the higher relapse rate observed in our study versus Nakayama et al. may be due to our longer follow-up (36 vs. 12 months). Moreover, our results are largely consistent with previous studies [9, 10, 22, 23, 26, 30, 37, 38].
Nishisho et al. [35] evaluated short-term changes in choroidal structure following adalimumab treatment for refractory, non-infectious uveitis, finding that using EDI-OCT, the SFCT appeared to be an effective choroidal imaging biomarker especially in VKH disease. SFCT decreased significantly from baseline to the values observed at two months (p = 0.007).
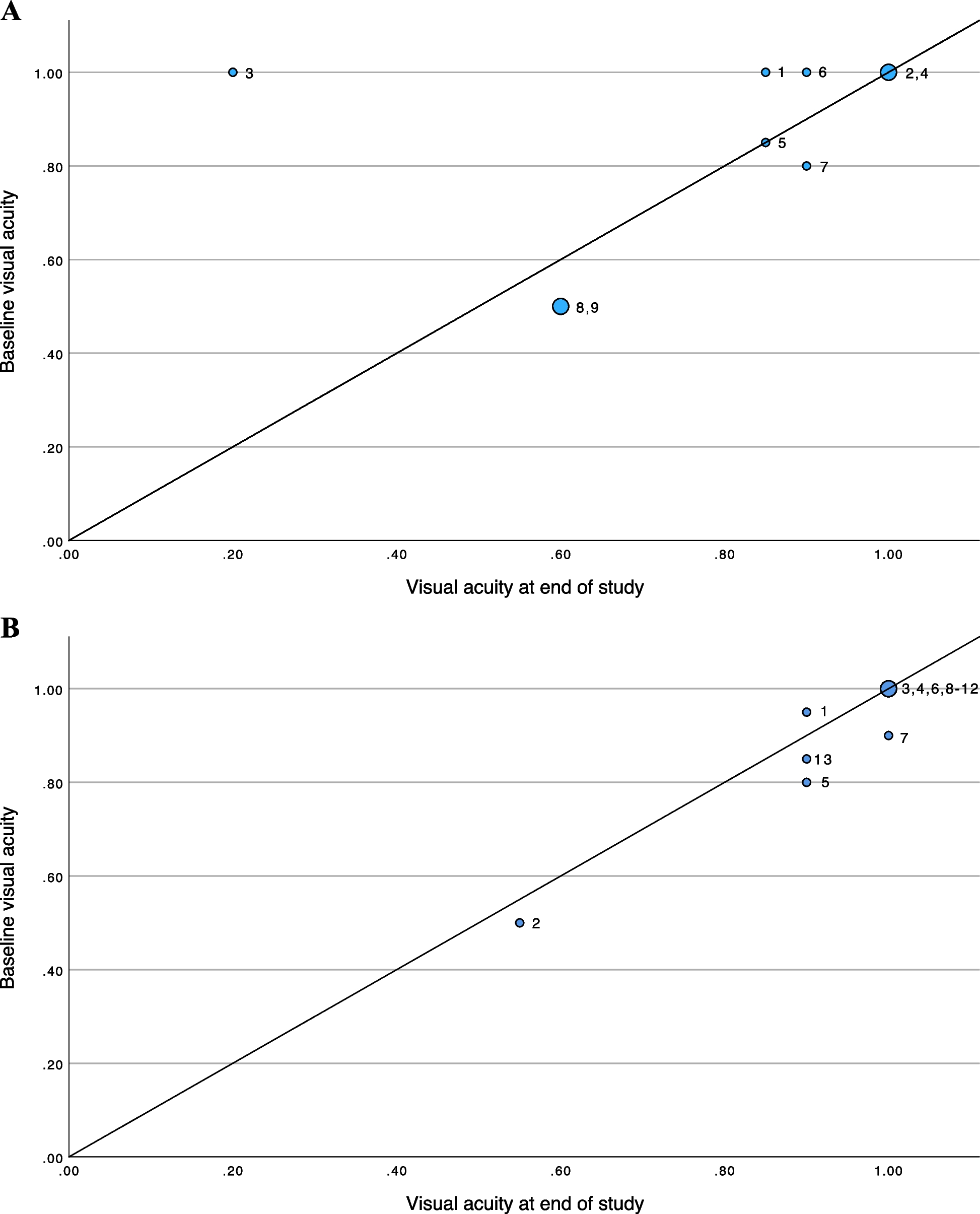
We did not find any correlation between the amount of visual loss and the increase in choroidal thickness in the patients with recurrent VKH. Generally, our results suggest that patients with more relapses and a thinner choroid will have a worse VA than patients with fewer relapses and a thicker choroid, presumably due to loss of tissue integrity with each additional relapse. Thus, choroidal thickening does not necessarily seem to imply a worsening of VA in a patient with few relapses. In addition, recurrences did not seem to affect the patients’ final VA, regardless of whether the patient was in the relapsing or quiescent group; by contrast, patients in the acute group had a better VA at study end.
We found a higher percentage of posterior recurrences than other published studies, probably because we were able to detect increases in choroidal thickness that were previously overlooked. In addition, our findings show that asymptomatic relapses tend to decrease over time.
When a relapse was detected in the recurrent group, in most cases the step-down treatment was discontinued, however, treatment was increased in some patients depending on the extent of vision loss and the degree of inflammation. Step-down treatment was resumed once choroidal thickness and VA were normalised compared to previous values. In the quiescent group, we restarted treatment in only one patient with decreased VA and choroiditis, which resolved by the next follow up visit. None of the other patients required treatment.
Finally, it is well-known that the presence of a hypopigmented fundus (sunset glow) could be attributable to unidentified (and thus, untreated) posterior recurrences [39], which is why routine use of ICGA during follow up is recommended in VKH patients3. However, given the aforementioned drawbacks of ICGA, the use of this modality should be minimized. In this regard, monitoring SFCT with SS-OCT may offer a valuable complement to ICGA. Although we used ICGA to confirm the presence of inflammation in all cases of relapse, we found that SS-OCT was quicker, easier and safer than angiography. Although we do not know how many asymptomatic relapses the patients may have had prior to inclusion in the study, the high rate of sunset glow fundus observed was not unexpected given that asymptomatic relapse appears to be associated with sunset glow fundus.
Study strengths and limitations
The main limitation of this study is the small sample size. Another limitation is that—despite the recurrent nature of this disease—we did not perform standardized monthly follow-up appointments in all patients. Rather, examinations were individualized according to the severity of each case. Another potential limitation is the cut-off value of ≥ 50 µm before performing the ICGA, as this may have led to an underdiagnosis of recurrences; however, this cut-off was selected to limit ICGA choroidal assessments to avoid performing unnecessary angiographies.
To our knowledge, this is the first study to use the automated measurement features of SS-OCT to measure choroidal thickness in patients with recurrent and quiescent VKH. Moreover, this prospective study includes the largest sample to date of Caucasian, Western European patients with VKH. Although other studies [23, 26, 30] have measured choroidal thickness in acute and chronic VKH, those studies were conducted in Japanese patients using EDI-OCT or SS-OCT [19] with manual measurement. Ours is the first study to present data on automated—and therefore objective—measurement of choroidal thickness obtained during the course of this disease, and also the only one that includes quiescent patients.








留言 (0)