Participants
Participants were volunteers recruited from two older adult residencies after approval by the management of the establishments. They read and signed an informed consent form and the General Data Protection Regulation (GDPR) information. Thirty-eight older adults (Mage = 80.15 years; ± SD = 7.21 years) completed the study.
Ethics
The study was conducted in the summer of 2023 with approval (Permission No. 2023/55) from the Faculty of Education and Psychology Research Ethics Board (REB) Eötvös Loránd University. Further, the work conformed to the ethical guidelines of the British Psychological Society (BPS) Code of Human Research Ethics (British Psychological Society [BPS], 2021). Additionally, the work followed the Helsinki Declaration (World Medical Association, 2013) principles of research with humans.
MeasuresDemographics and Cardiovascular Indices
Demographic and initial physiological measures included age, gender, body weight, height, resting heart rate, and diastolic and systolic blood pressure. All participants were 60 or over (age range 60 to 94 years), and two-thirds (n = 25) were women. Their mean (± SD) weight and height were 78.00 ± 13.04 kg and 169.53 ± 12.19 cm, respectively. Their mean resting heart rate was 64.24 ± 7.99 bpm, systolic blood pressure 125.71 ± 12–72, and diastolic blood pressure 79.42 ± 13.31 mmHg. A medical doctor or the head nurse of the residence screened the volunteers before participating in the study by evaluating their mental and physical conditions. Only participants with medical clearance were permitted to participate in the study.
Risk of Fall (ROF)
We measured the ROF with the Berg Balance Test (BBT; Berg et al., 1989). This test assesses a person’s functional balance via their performance on 14 distinct activities commonly encountered in daily life. These activities measure the individual’s ability to sustain positions of increasing difficulty while gradually reducing the support base. The scale comprises three key dimensions: maintaining a position, adjusting posture in response to voluntary movements, and reacting to external disturbances. Each activity is scored on a five-point scale ranging from zero to four (zero indicating inability to perform and four indicating independence), with specific criteria outlined for each score level. Scores range from zero to 56 and are based on factors such as the duration of position maintenance, reach distance of the arms, or time taken to complete a task. The tested persons get a lower score if they require supervision, prompting, or assistance during an activity or fail to meet time or distance requirements. This test could predict the ROF (Park & Lee, 2016), however there is discord concerning its predictive accuracy (Lima et al., 2018). Nevertheless, a relatively recent study comparing six methods of ROF assessment revealed that the BBT was the most accurate (83% (95% CI [70⎯91]), which was followed by two others with only 67% predicting accuracy (Menezes et al., 2020). Notable is that a higher score on the BBT is associated with a lower ROF.
Psychometric Assessment
Connor-Davidson Resilience Scale (CD-RISC-10)
Resilience was tested with the 10-item Connor-Davidson Resilience Scale (CD-RISC-10: Connor & Davidson, 2003). Participants responded on a 5-point Likert scale, ranging from ‘0’ (not true at all) to ‘4’ (true nearly all the time), yielding a total score between 0 and 40, with higher scores indicating greater resilience. A sample item from CD-RISC-10 is: “I am able to adapt when changes occur.” The Cronbach’s alpha (α) of the scale is 0.80 (Connor-Davidson, 2003).
Well-being Questionnaire (WHO-5)
The WHO-5 (World Health Organization, 1998). consists of five positively phrased statements reflecting perceived well-being during the past two weeks. A sample item is: “I have felt cheerful and in good spirits.” People answer the five positively worded items of the WHO-5 on a 4-point Likert scale, ranging from ‘0’ (never) to ‘3’ (always). Thus, the total score is between 0 and 15. A higher score mirrors greater subjective well-being. The internal reliability of the WHO-5 is 0.85 (Topp et al., 2015).
Perceived Stress Scale (PSS-4)
The PSS-4 measures individuals’ perceptions of life stress retrospectively in the past two weeks. It is rated on a 5-point Likert scale ranging from ‘0’ (never) to ‘4’ (very often), thus yielding a score between 0 and 16. Positive items assess coping efficacy, while negative items measure feelings of hopelessness, which are associated with depression (Hewitt et al., 1992). Higher PSS scores are related to adverse health effects (Klein et al., 2016). Despite its brevity, the PSS-4 has good psychometric properties (Warttig et al., 2013). Its internal consistency (Cronbach’s α) ranges from 0.84 to 0.86 (Cohen, 1983).
Satisfaction with Life Scale (SWLS)
This scale is rated on a 7-point disagreement-agreement scale and consists of five items, such as “In most ways, my life is close to my ideal.” A total SWL score is calculated by summing or averaging the scores across the five items. A higher score reflects more life satisfaction. Its internal reliability is 0.81 (Diener et al., 1985).
Subjective Happiness Scale (SHS)
Happiness was measured using the Subjective Happiness Scale (Lyubomirsky & Lepper, 1999). This scale comprises four items rated on seven points related to the state of happiness; however, one item inquiries about the state of unhappiness is reverse scored. Higher scores indicate greater subjective happiness. The scale’s internal consistency is 0.86.
Objective Physical Measures
The FFFT assessed functional fitness (Jones & Rikli, 2000; Rikli & Jones, 1999, 2013). It included six measures that we complemented with handgrip strength test (Migaj et al., 2022):
1.
Lower body strength(FFFT1) − 30s chair test, complete stand up and sit down (assess the number of repetitions).
2.
Upper body strength(FFFT2) – lifting 2 (women) or 3.5 (men) kg dumbbell while sitting on a chair and doing full arm bends and stretches (assess the number of repetitions in 30 Sect. ).
3.
Upper body flexibility(FFFT3) - fingers touching behind the back (back scratch) (assess +/- cm).
4.
Lower body flexibility(FFFT4)- forward bend from chair to extended leg (chair sit-and-reach) (assess +/- cm).
5.
Complex movement coordination (agility, balance, and walking speed[FFFT5]) - standing up from a chair and avoiding a buoy 2.44 m away (8 feet) and returning to the chair (assess the duration in seconds).
6.
Endurance (physical effort([FFFT6]) – For safety reasons (Różańska-Kirschke et al., 2006), the six-minute walk test was replaced with the two-minute step-in-place test (assess the number of total steps completed in two minutes), raising each knee to the point halfway between the patella (kneecap) and iliac crest (top hip bone).
7.
Handgrip strength (added to the FFFT) based on Migaj et al. (2022) - squeezing a dynamometer with the dominant hand in a sitting position with an extended elbow and the shoulder joint flexed to 90 degrees (assess the best of three trials).
The FFFT is safe for inactive and physically active older adults; by examining everyday motor patterns, researchers can get an insight into the six functional fitness indices described above (Różańska-Kirschke et al., 2006). Finally, we calculated BMI by dividing participants’ weight (kg) by height (m) squared.
Procedure
Participants were tested individually in a quiet, spacious room in their older adult residence. After completing the questionnaires presented in shuffled (random) order, the first author, a movement therapist, explained and demonstrated the FFFT to the participants before each of the six trials. After completing the six FFFT trials and the dynamometer test, the participants were debriefed and thanked for participating.
Data Analyses
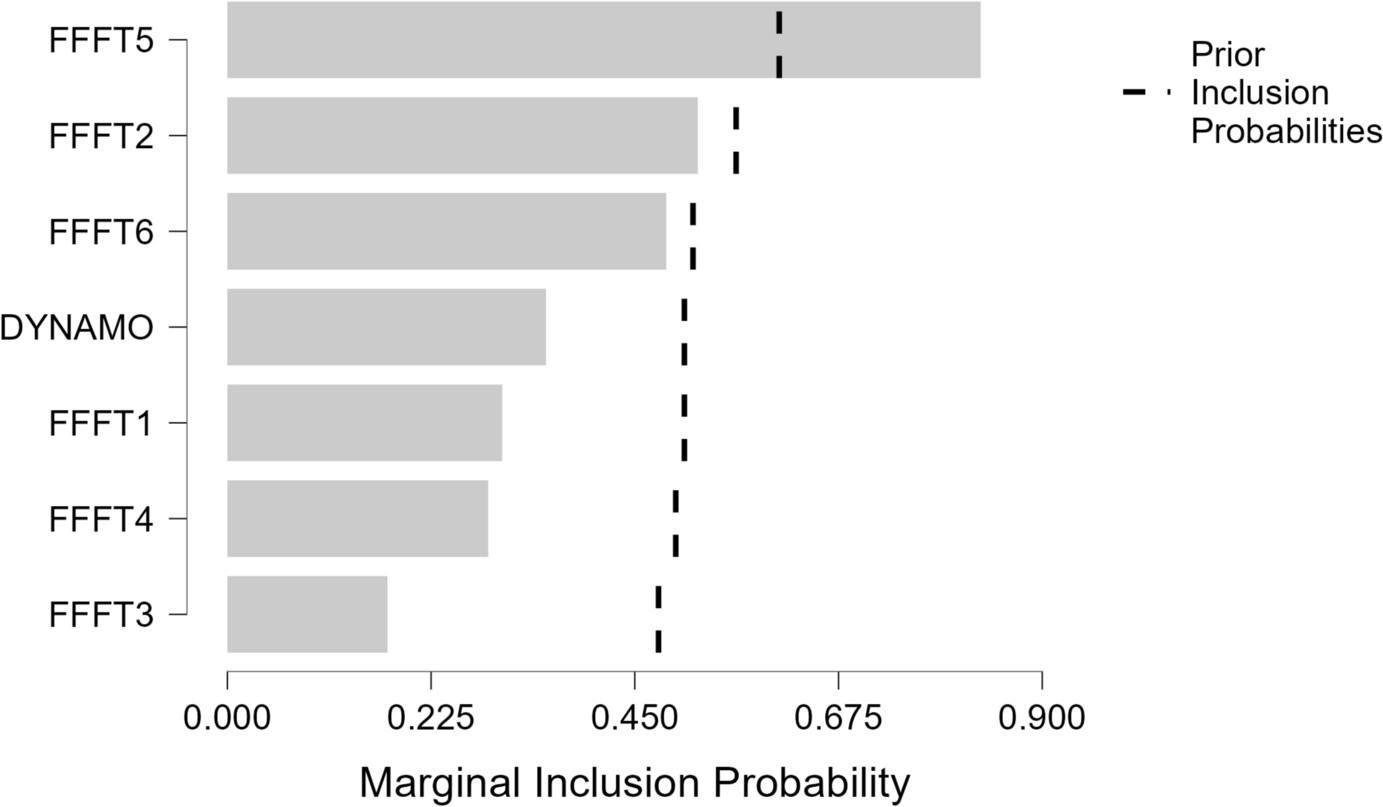
We analyzed the data with the JASP 0.16.0.0 statistical software (JASP Team, 2024). We performed Spearman rank correlations to examine the relationships between ROF, FFFT, handgrip strength (objective predictors), and psychological measures (subjective predictors). Subsequently, due to the relatively low sample size, we used Bayesian linear regression with Markov Chain Monte Carlo (MCMC) sampling, which is justified by the relatively small sample and expected correlated predictors in physical (de Souza Santos et al., 2011) and psychological (Byun & Jung, 2016) measures. Further, this simulation method can provide estimates of posterior distributions of regression coefficients, permitting inference about the uncertainty in parameter estimates. Overall, the Bayesian regression with MCMC was presumed to yield robust inference, allowing model comparison and granting flexibility in model specification. Last, we tested whether subjective predictor(s) might mediate the relationship between objective FFFT measures and the ROF. Data on which this research is based is available at the Mendeley data repository (DOI: https://doi.org/10.17632/57swztzrt8.1).







留言 (0)