
記住我








We searched PubMed and Google Scholar for published articles that discussed contributions to the COVID-19 pandemic response attributed to SPHs. Owing to the limited literature, we developed a reporting template that we shared with members of the SPHs in different countries to provide a summary of their contributions as well as documents and links to country-specific information they were aware of. The template had several sections including the research conducted, response committees engaged in, policy support provided, technology and innovations created, and other roles and contributions made by SPHs in the country. The template was shared widely through the Association of Schools of Public Health network which has a wide membership of faculty across the continent to provide a broader regional picture of the contributions of SPHs in Africa. We extracted relevant information from the published articles, documents and grey literature onto a Microsoft Excel form which we synthesised around relevant themes. The presentation of the themes was supplemented by detailed case studies as shared by the SPHs.
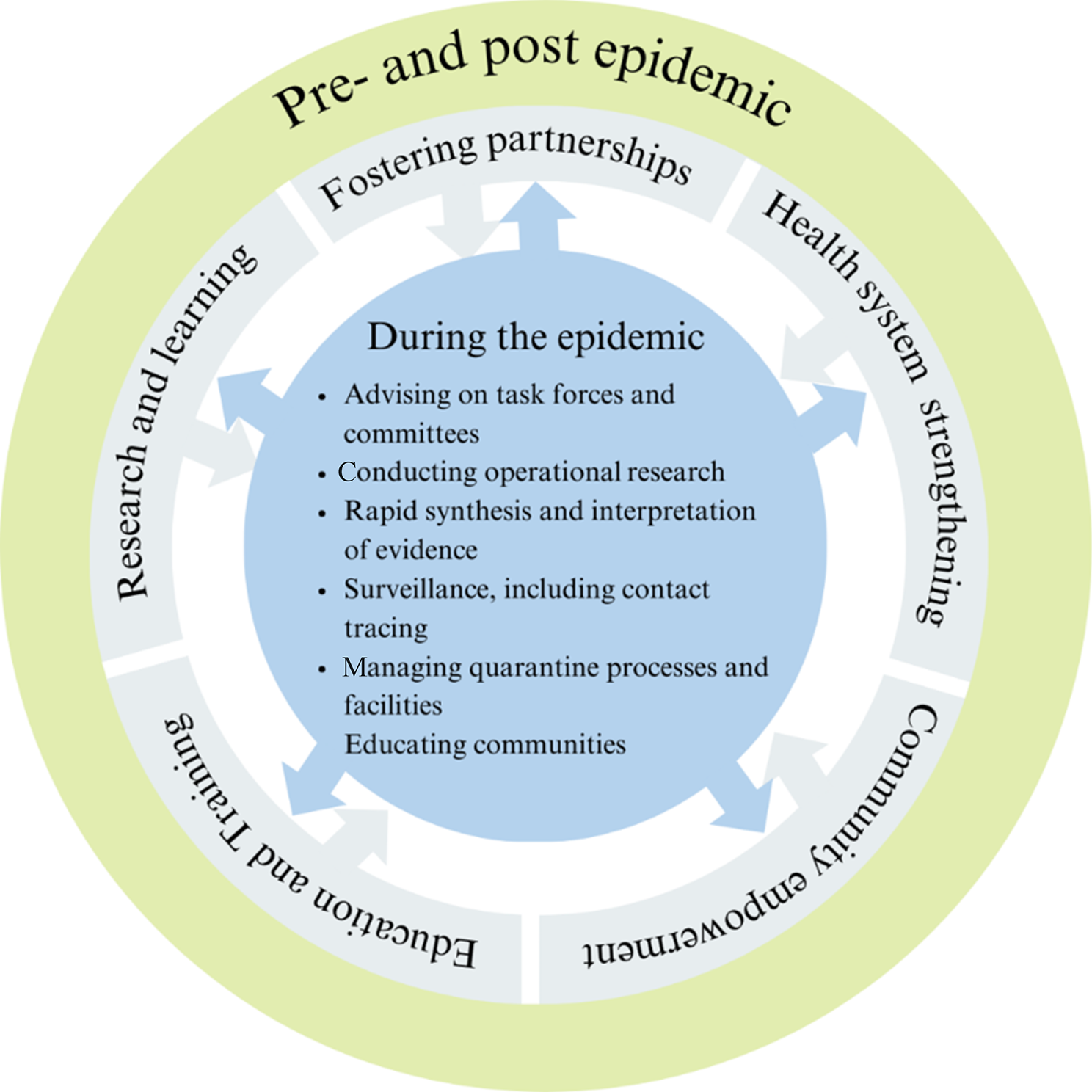
Contributions of the schools of public healthTo support the response to COVID-19, governments worked closely with SPHs especially those within the public universities to support various roles and functions. Most of these SPHs have a clear and close working relationship with the government through their ministries of health where they support public health programming as members of technical working groups, and through research and programme evaluations, evidence synthesis, capacity strengthening, and development of policy guidelines and other documents. On the other hand, the ministries of health contribute to the work of the SPHs through technical expertise, access to resources including data, reports and policies, and support in programme implementation. The SPHs also work closely with local, regional and international organisations through various networks bringing together expertise, mobilising funding, and sharing experiences informing regional policies and practice. Relying on these relationships and amidst the considerable disruptions in routine performance of their functions caused by COVID-19, SPHs continued to perform essential functions to support controlling the outbreak. The roles that SPHs played during the pandemic included: advising task forces and committees, supporting COVID-19 policies at sub-national and national levels, research, training, and supporting field activities such as contact tracing as detailed in the following sections and summarised in Fig. 1.
Fig. 1
Roles played by SPHs in Africa pre-, during, and post- the COVID-19 pandemic
COVID-19 task forces and advisory committeesAcross the continent, the response to COVID-19 was organized around task forces and committees, most of which were multidisciplinary and multisectoral with varying functions and levels of decision-making. Faculty of SPHs such as in DRC, Nigeria, Ethiopia, South Africa, Senegal, and Uganda were part of Presidential and National task forces overseeing the COVID-19 response in their countries. In some cases, SPH faculty chaired or co-chaired these committees at national, regional, or provincial levels such as in Malawi where a faculty member co-chaired the Presidential Task Force on COVID-19 alongside the Minister of Health. SPHs’ experts were also part of COVID-19 response committees such as the Scientific Advisory Committee, which reviewed the evidence and made policy recommendations to guide the national task forces and the Emergency Operations Centers. Faculty at SPHs also contributed to the core response pillars as they were charged with effective coordination and management of COVID-19 interventions such as Surveillance and Laboratory, Case Management, Infection Prevention and Control (IPC), and Risk Communication. For example, faculty from the Muhimbili University of Health and Allied Sciences SPH in Tanzania were part of the Case Management, IPC & Water Sanitation and Hygiene. In Nigeria, SPH faculty contributed to the IPC, Epidemiology and Surveillance, and Risk Communication Pillars.
Summarizing evidence and policy supportAs one of their key roles, SPH faculty on the COVID-19 response committees identified, reviewed, and synthesised the rapidly evolving global and local evidence and customized it to the local context to inform policy decisions in their respective countries. SPH faculty also supported the review of the performance of various COVID-19 response interventions. These efforts informed key decisions and plans regarding public health and social measures to adopt, their timing and duration, as well as effective treatment regimens. SPHs also worked with ministries of health to translate their data into policies, guidelines, and recommendations. For example, the Universities of Ghana, Makerere, Cape Town, and Nairobi SPHs conducted modelling of the impact of the COVID-19 pandemic and the effect of potential response measures, providing critical information for policymakers to guide decision-making. Researchers at the University of Pretoria significantly contributed to the COVID-19 response by establishing a databank that provided real-time updates and factual information on the pandemic [17]. This initiative aimed to empower decision-makers and the general public with accurate data and statistics through an interactive dashboard, enhancing the understanding of the pandemic’s impact in South Africa. By automating data collection and validation, and offering a user-friendly platform, the group leveraged data science to address social challenges, ensuring resource pooling during crises and promoting transparency to combat misinformation [17]. In Uganda, the national COVID-19 vaccines committee which included three SPH professors was charged with the responsibility of determining which vaccines to procure and expediting their acquisition and distribution across the country [18]. In addition, faculty from the Makerere SPH led the revision of the guidelines for maintenance of essential health services during epidemics in Uganda. The University of Nairobi’s SPH also supported the process of drafting the COVID-19 response bill on behalf of the Kenyan government to protect the rights of citizens during the pandemic.
ResearchSPHs across Africa conducted research to enhance the understanding of the novel SARS-CoV-2 virus and inform policy and interventions within countries and across the continent. For example, SPH researchers in DRC, Ghana, Nigeria, South Africa, and Uganda led and conducted knowledge, attitudes, and practices surveys, rapid assessments, seroprevalence surveys, and studies on the feasibility, safety, and efficacy of potential COVID-19 treatments. The University of Pretoria SPH conducted research on a wide range of themes including genomics, health and socioeconomic consequences of pandemic measures, and vaccine acceptability (Table 1). SPH researchers also conducted operational research to provide real-time evidence to inform the COVID-19 response on the continent across several themes, including the impact of public health and social measures on COVID-19 and non-COVID-19 outcomes, and on health system governance and resilience. Building on their long-standing collaboration, a Makerere University-led partnership of five SPHs in Africa assessed aspects of COVID-19 testing [19], surveillance [20], maintenance of essential health services [21,22,23], consequences of public health and social measures [24, 25], and uptake of vaccines [26, 27] in the DRC, Ghana, Nigeria, Senegal, and Uganda. Recommendations from this research informed improving coordination of the laboratory network in Nigeria and developing and updating testing and surveillance guidelines for West Africa Health Organization member states. In Uganda, the study findings informed the revision of maintenance of essential health services guidelines [28] and instituting continuity of essential health services as a separate epidemic response pillar. The Addis Ababa SPH in Ethiopia conducted monitoring of hand hygiene, physical distance, and respiratory hygiene in 14 main cities of the country. In Nigeria, the Lagos State University Department of Community Health and Primary Health Care led the COVID-19 daily data update and dissemination in the state for decision-making. Makerere University in Uganda through government funding financed over 110 research and innovation projects, addressing questions critical to the COVID-19 response [29]. SPHs also provided data analysis support to analyse the large volumes of surveillance, contact tracing, laboratory and health facility data collected by the ministries of health. Overall, research across the continent supported improvements in response operations, the deployment of public health and social measures and the rollout of vaccines.
Table 1 University of Pretoria’s COVID-19 research contributionsTrainingSPHs supported the COVID-19 response through training conducted at different levels. In the DRC, Kinshasa SPH trained field epidemiology fellows who were deployed to conduct surveillance and contact tracing. The institution also provided short online courses to frontline health workers to prepare them to receive their first cases of COVID-19 and build their capacity to conduct surveillance. In Nigeria, SPHs alongside field epidemiology graduates and fellows trained health workers on the COVID-19 control pillars (coordination, surveillance, laboratory, and data management) prior to the confirmation of the first case. At the Ibadan SPH, faculty trained rapid response teams at subnational levels about surveillance and IPC. In Uganda, Makerere University initiated a community of practice on IPC for health workers, targeting 2,000 healthcare workers/IPC focal persons from 764 health facilities in 130 districts across the country. The university also trained over 1,000 community health workers (CHWs) to conduct health promotion activities on COVID-19 [30]. Another round of training reached over 900 CHWs and 500 community leaders, with over 19,000 community members vaccinated during the organized COVID-19 vaccination outreaches (Table 2). Makerere SPH together with the College of Veterinary Medicine developed and offered a one-month course on pandemic preparedness following the One Health approach targeting responders, frontline implementers, crisis communicators, social scientists, and agriculturalists [31]. The Tropical Institute of Health’s proactive approach, grounded in community-based data collection and action, extensive training, and strategic collaborations contributed to managing the COVID-19 crisis in Western Kenya. Evidence indicated that the incidence of confirmed COVID-19 infections and deaths was lower in the Institute’s intervention area compared to the control county [32]. The University of Botswana SPH trained cleaning staff at the university on IPC and raised awareness about preventing COVID-19. The other roles SPHs undertook included offering training to media practitioners on COVID-19 interventions and how to communicate decisions to the public. SPHs also offered orientation for district staff on data collection tools and reporting systems.
Table 2 Makerere University SPH intervention enhanced uptake of COVID-19 vaccines in Wakiso District, UgandaField support for surveillance and contact tracingSPHs provided field support to the COVID-19 response. SPH faculty served in the incident command structures where they were deployed to coordinate the regular meetings at national and subnational levels. In Uganda, for example, 26 Master of Public Health students and 25 field epidemiology trainees were part of the COVID-19 workforce conducting surveillance and contact tracing in the community and screening people at points of entry (Table 3). Across countries, staff, students, and field epidemiology fellows also supported rapid response and alert management systems, conducting epidemiological investigations of cases and contacts, managing quarantine sites, and overseeing reporting and line listing. Several faculty of the University of Ibadan SPH including the students of the Field Epidemiology Training Programme supported both state and national emergency operations centres and pillars of COVID-19 response including Epidemiology and Surveillance, Laboratory, and Case Management pillars. Public Health postgraduate students were also deployed to screen international travellers, conduct risk communication with passengers, and monitor persons of interest. In Namibia, field epidemiology and public health (bachelors and masters) students considerably contributed to the establishment of the National Emergency Operations Centre where COVID-19 surveillance activities were performed. The Centre also supported the preparation of integrated support visits to border regions and the strengthening of the coordination and management of response interventions at regional/district levels.
Table 3 Makerere University SPH - Master of Public Health alumni and residents supported COVID-19 response in UgandaDevelopment of technologies and innovationsSPHs and collaborators contributed to innovations to support the containment of the COVID-19 pandemic. In Uganda, Makerere SPH collaborated with the Ministry of Science, Technology, and Innovation and Kiira Motors Company to develop a low-cost ventilator that can be locally produced [33]. In Nigeria, a collaboration with a non-governmental organization led to the production of hand sanitizers that were donated to the Enugu State Ministry of Health and the University of Nigeria Teaching Hospital [34]. The University of Namibia SPH in collaboration with Namibia Breweries Limited and other stakeholders developed a local hand sanitizer solution initially for university staff and students, but later expanded with private sector interest [35]. The university donated four Philips Respirator Machines to the Ministry of Health and Social Services to support the government’s response to COVID-19. The University of Namibia also introduced a smart phone application for self-reporting of COVID-19 symptoms and another for contact tracing. SPH faculty from the University of Western Cape working with social justice activists and community workers supported the establishment of Community Action Networks which supported and guided communities’ response to the pandemic and associated impacts. Several Community Action Networks were then initiated across Cape Town and were instrumental in dealing with hunger during COVID-19 through initiatives such as community kitchens.
Public education and awarenessFaculty of SPHs made significant contributions in raising COVID-19 awareness and filling the information void during the response through mass and social media platforms. SPHs such as Ghana SPH developed and disseminated messages to counter misinformation and some provided hotlines for the public to call in. The Tropical Institute of Community Health and Development in Kenya embarked on an extensive community awareness campaign where they trained Community Health Volunteers on preventive measures, equipping them with knowledge and skills to educate the wider community. The Addis Ababa SPH staff educated the public on hand hygiene, physical distancing and respiratory hygiene through a Television program titled “Tenawo be Bebtewo” meaning “your health at your house” advocating for obtaining health related information though watching TV. Working with the Tanzania Public Health Association and the World Health Organization, the Muhimbili SPH sensitized 240 older persons on COVID-19 preventive measures in districts in the Kilimanjaro region to enhance their engagement in COVID-19 response. The school also developed information, education, and communication materials for educating the public on COVID-19 prevention and control and held weekly sessions on X (formerly Twitter) spaces. The University of Nairobi SPH through the Elimika Youth Programme provided youth and students with mental health services and information about the pandemic using technology to share facts and reduce misinformation. Across countries including Botswana, DRC, Kenya, Namibia, Nigeria, South Africa, Tanzania, and Uganda, faculty of the SPH frequently conducted newspaper, radio, and television interviews to share information about COVID-19 not only with the general public but with other experts including through opinion pieces and commentaries. These efforts by the SPHs resulted in improved awareness among communities, fostering adherence to preventive measures such as mask-wearing, hand hygiene, and social distancing.
Other contributionsSPHs also played a critical role in advising and preparing workplaces for reopening during COVID-19 through developing standard operating procedures and training materials, creating a close partnership with the private sector. SPHs convened meetings, conferences, and symposia to share knowledge, expertise and experiences to improve COVID-19 response efforts. The University of Namibia SPH held a global symposia on responses to TB and COVID-19 aiming to improve health and research collaboration. In South Africa, Tanzania, and Uganda, SPHs organized weekly webinars to unite multidisciplinary scientists and facilitate discussions on topical issues about COVID-19. In Malawi, faculty from the Kamuzu University of Health Sciences School of Global and Public Health under the Society of Medical Doctors offered expert opinions in court as amicus curiae (friends of court) when COVID-19 lockdown measures were challenged. Within their universities, faculty of the SPHs provided guidance on standard operating procedures. Several faculty members also engaged with other higher education institutions to develop COVID-19 prevention and control plans. SPH colleagues offered psychosocial support to colleagues and university students.
ImplicationsDuring the COVID-19 pandemic, SPHs in Africa contributed to addressing key gaps in the response and supported local, national, and regional responses. The SPHs undertook critical research to inform policy decisions, supported field activities, trained frontline healthcare professionals on pandemic response, and provided technical assistance to governments and health agencies. Performing these tasks relied on previously formed relationships with the ministries of health, and in undertaking them, they forged new relationships, interactions, and expectations that will influence future programming. On the other hand, working closely with the SPHs lent the government and their ministries of health additional credibility and trust at a time when it was critical, but low, in the public. The collaborative efforts supported buy-in for the response, especially for the implementation of interventions as well as mobilization and lobbying for resources to support the response. Moreover, academic institutions being considered independent, were critical in advocating for evidence-based positions in the policy and decision-making processes. The close working relationship between the government and academia improved transparency and accountability in the response or its perception in most countries. The interaction, however, also came along with potential risks of collective responsibility and accountability with potential repercussions for individual and institutional reputations. In the future, institutions will need to put in place safeguards on how to navigate these relationships to maximise their potential and minimize their negative consequences.
SPHs in Africa bolstered themselves as an important stakeholder in epidemic preparedness and disease response relying on their expertise, legitimacy, and credibility and building on previous efforts and contributions to past outbreaks. This further illustrated the significant role of SPHs in low- and middle-income countries as previously highlighted [10, 36]. SPHs supported national responses to the COVID-19 pandemic by leveraging their expertise as academic institutions. As centres of knowledge generation and evidence synthesis, SPHs guided the policies and interventions that were implemented during the pandemic taking on mostly advisory and strategic roles and in other instances leading important committees. The closer the SPHs were to the decision-making entities, the more prominence and recognition they received amidst more scrutiny and accountability. Both students and faculty contributed directly to the response by training health workers, conducting surveillance and contact tracing as well as engaging in public education. As centres of training, SPHs were a resource for health personnel, directly contributing to the human resource needs during the COVID-19 response. Beyond typical academic roles, SPHs also exerted their expertise to support effective policy and decision-making and strengthen health systems. To achieve these roles, SPHs collaborated with multiple disciplines and stakeholders within and outside of the universities, highlighting the significance, versatility, and interconnectedness of public health with other health and non-health sciences. SPHs also relied on their strong partnerships with the ministries of health, civil society organizations, and other partners, funding from external sources, access to data, abundant skills and expertise, and their pool of trainees to enhance their contribution to the response. The roles played by the SPHs during the pandemic were facilitated by their mandates, functions, and investments. Most of the SPHs also had prior experience supporting previous epidemics and contributing to addressing broader public health challenges in their countries – all of which prepared the SPHs to respond to the COVID-19 pandemic. Amidst the contribution of the SPHs during the COVID-19 pandemic, several challenges existed. The slow and bureaucratic nature of government systems, limited access to funding for activities, the closure of learning institutions, and public misinformation and distrust all impeded the pace of SPHs’ work and minimized their contribution. The fast-changing pace of the pandemic and priorities around it also meant that some SPHs’ work and innovations, even when critical, were not continued and/or sustained.
Although the contributions of SPHs across the continent are presented collectively, countries and regions on the continent experienced the pandemic in different ways which shaped the unique contributions observed and interrogated in the different countries. For example, North and Southern Africa were noted to have had the most devasting COVID-19 impacts [37]. The other factors that impacted the SPHs contributions were related to the level of the country’s development [37, 38], capacity of SPHs including staff expertise and technology access, availability and functionality of national public health institutes [14], existence and strength of field epidemiology programmes [15] and level of collaboration and/or embeddedness with other non-governmental sectors [16]. Moreover, the country’s governance and broader geopolitical context [39] influenced the level and type of engagement with the SPHs. The contribution of SPHs was likely greater in countries that were stable with effective, inclusive, and accountable institutions with a high level of population trust. Whereas COVID-19 negatively impacted globalization [40], it was clear that the collaborative regional networks of SPHs provided avenues for expertise, experience, and resource sharing which impacted country-level response and supplemented government-to-government interaction.
Across SPHs, inequity in capacity and resources exists across regions and countries which impacts their outputs. Indeed, the contribution as presented in this article was not uniform across the continent, countries, and schools. Strong and well-established SPHs situated within public universities tend to be more resourced, networked and more involved in their country’s public health preparedness and response plans. On the other hand, some countries do not have SPHs while others have newly established and under-resourced schools, undermining their contribution to disease prevention and health promotion efforts. It is thus critical to bridge the existing equity gaps and enhance the capacity of SPHs across the continent to conduct training and research, as well as support public health functions. Indeed, with greater capacity and support, the contribution of the SPHs to the COVID-19 response could have been more robust and greater. Strengthened SPHs are crucial to robust and sustainable outbreak preparedness and response. More broadly, well-equipped, and functional SPHs are important to support the continent to deal with the new, emerging, and complex public health challenges that it faces. Indeed, the African continent bears a huge burden of disease influenced by transitions in disease epidemiology, demography, and their dynamic political and socio-economic context [41]. The continent is also prone to epidemics of infectious diseases [42] as well as natural and man-made disasters [43] and bears a large burden of climate change effects [44, 45]. SPHs across the continent thus require dedicated and sustained support from governments, funders, the private sector, non-governmental organizations, and the public to achieve their mandate with sustainability, equity, effectiveness, and efficiency as guiding principles. This is especially critical for the SPHs to play their proactive disease prevention role as opposed to the largely reactionary function whenever extreme events occur. Indeed, whereas a large burden of disease on the continent is preventable, the role of disease prevention and health promotion, paramount for the achievement of universal health coverage and ensuring the health and well-being of the population, is usually given less attention [46, 47]. Other efforts are required to improve the coordination of SPHs, strengthen collaboration among schools, harmonize training and curricula such as for field epidemiologists and public health graduates, and enhance capacity for advanced research. These efforts would position SPHs to undertake their important roles, such as building quality and skilled workforce, and support the health systems on the continent and beyond. The efforts would also contribute to Africa CDC’s new public health order [48] to address structural public health deficiencies and strengthen public health institutions as well as other continental and global agenda.
Whereas this paper has focused mostly on the functions of the SPHs and areas where their contribution was strongest, there were collaborative efforts and contributions from the other health sciences schools and other disciplines across universities. The literature review also focused on sub-Saharan Africa and aspects of response from North Africa may not be represented. The examples highlighted are also not meant to be exhaustive but rather illustrative to provide key insights. We also cannot speak of the effectiveness of the activities implemented which future research should look into.
留言 (0)