Study design
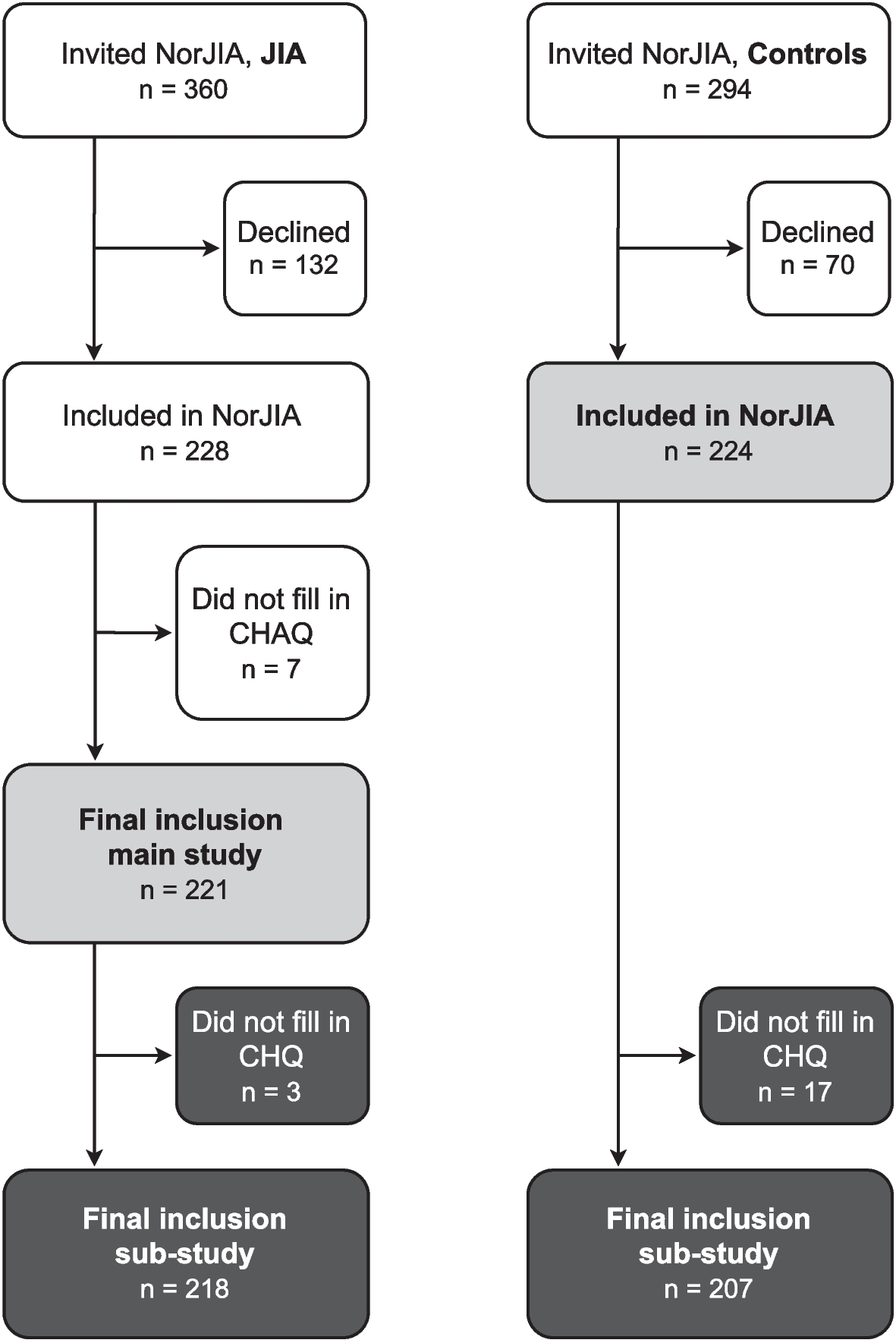
The NorJIA study is a prospective, multicenter, observational study, https://norjia.com/. Cases were recruited from out-patient clinics at the pediatric departments of St. Olavs University Hospital in Trondheim, Mid-Norway, Haukeland University Hospital in Bergen, Western Norway, and University Hospital of North Norway in Tromsø, Northern Norway. The participants with JIA, who had random disease durations, were examined twice, two years apart (± 3 months). The baseline clinical examinations were set between 2015 and 2018. Inclusion criteria were children between the age of 4 and 16 years meeting the International League of Associations for Rheumatology (ILAR) criteria for JIA [13], with parents’ or legal guardians’ (in this article collectively referred to as parents) informed consent. The lower cut-off of 4 years was determined as the lowest age we could ask a child and his/her parents to participate in a comprehensive study consisting of two consecutive study days with various examinations. There were no exclusion criteria.
The matched population-based control cohort consisted of children without JIA, matched 1:1 for sex and age. They were recruited from dental offices related to the Center for Oral Health Services and Research, Mid-Norway (TkMidt), the Oral Health Center of Expertise in Western Norway (TkV), and the Public Dental Health Service Competence Center of Northern Norway (TkNN). The children were called in for a free dentist appointment according to the Norwegian public dental service policy and could therefore be considered a random sample from the general population. The study design of this study is cross-sectional, using data from the baseline examination. For this particular study, the inclusion criteria were participation in the baseline visit of the NorJIA study with a completed CHAQ. In sub-analyses, participants, both those with JIA and controls, with a completed CHQ were included.
Data collection
The NorJIA study included extensive clinical, laboratory, radiological, and oral examinations at baseline and after two years’ follow-up. It also included several PROMs, including CHAQ and CHQ. Relevant data from the baseline study visit included: Sex, age at disease onset and at study visit, parental education level, ethnicity, anthropometric data, blood test results, JIA category according to the ILAR classification criteria [13], joint status evaluated by the physician at the study visit (including number of active joints), disease status at the study visit according to Wallace and the American College of Rheumatology (ACR) criteria [14, 15], and medication (past and present). Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were assessed at the clinical examination. Other blood tests such as human leukocyte antigen B27 (HLA-B27), rheumatoid factor (RF), and anti-nuclear antibody (ANA) were all measured around the time of the diagnosis and registered in the NorJIA database. RF and ANA were measured twice at least three months apart; for ANA an indirect immunofluorescence assay on HEp-2 cells was used. In addition to the clinical examination, either the patient (if the patient was nine years or older), or the parents (if the child was younger than nine years), filled out the CHAQ form. In addition, pain as well as overall well-being, were reported by the participants (patient or parents, as above) on a visual analogue scale (VAS). They also reported duration of morning stiffness. Parents of both participants with JIA and sex- and age-matched controls (regardless of the patient’s age) filled out the CHQ.
Measures
Parental education level was reported by the parents of both children with JIA and controls, and subsequently divided into four levels: Primary and middle school (7 to 10 years of education), high school (11 to 13 or 14 years), less than five years of university education, and five or more years of university education. The last two levels will be collectively referred to as parents with higher education. The grouping was defined according to the parent with the highest education level.
Body mass index (BMI) was calculated using the following formula: Weight (kilograms)/[height (metres)]2 and subsequently adjusted for sex and age according to the International Obesity Task Force (IOTF) cut-off values to provide an Iso-BMI stratification that allows for comparison with adult BMI groups: Underweight (BMI < 18.5), normal (BMI ≥ 18.5 and < 25), overweight (BMI ≥ 25 and < 30), obesity (BMI ≥ 30) [16, 17].
Patient-reported outcome measures
Patient-reported physical disability was assessed with CHAQ. This questionnaire evaluates the patient’s everyday physical functioning during the previous week, through 30 items divided into eight domains: Dressing, arising, eating, walking, hygiene, reach, grip, and activities. The need for assistance in the form of aids, devices, and help from another person for physical functioning are also registered. According to their questionnaire responses, a global CHAQ score was calculated for each patient. This score ranges from zero (no or minimal physical disability) to three (very severe physical disability) [11, 18]. The CHAQ is cross-culturally validated and translated into many languages, including Norwegian [19]. Patient/parent-reported disease-related pain during the last week was measured on a 21-numbered circle VAS, where zero equals “no pain at all” and 10 equals “very severe pain”. The VAS pain score is extensively used both in clinical follow-up and in research, both in the form of a continuous 10 cm scale and a 21-numbered scale [20]. The patient’s global assessment of disease impact on overall well-being (PatGA) is a tool where the patient/parent scores the influence of the disease on the patient’s everyday life during the last week on a 21-numbered circle VAS from 0–10, where zero represents “no influence at all” and 10 “severely influenced”. This tool is extensively used, both in clinical follow-up of JIA and in research [10, 20]. Morning stiffness during the last week was reported by the patient (≥ 9 years old) or parents (for children < 9 years old) in minutes. The generic 50-item Child Health Questionnaire-Parent Version (CHQ-PF50) – in this article referred to as CHQ – includes questions about topics such as general health, physical functioning, physical pain, mental health, as well as the impact on both the patient, parents, and family in general, reported for the last four weeks [11, 12]. The responses were compiled into a summarized score with a scale from 1 to 100, where higher scores indicate a higher level of functioning and well-being comparable to norm scores (50 ± 10) from the general U.S. population. The responses are used to calculate a Physical Summary Score (PhS) and a Psychosocial Summary Score (PsS), also with norm scores (50 ± 10).
Physician-reported outcome measures
The physician’s global assessment of disease activity (PhysGA) was reported by the physician on a 21-numbered circle VAS from zero to 10 where zero equals “no activity” and 10 equals “high activity” [20].
Composite disease activity measures
Disease status was defined according to Wallace et al. [14] with modifications according to the ACR endorsed criteria [15]. Inactive disease was accordingly defined as no active arthritis or uveitis, no systemic manifestations of JIA, normal acute inflammatory markers (ESR or CRP) or, if elevated, not attributable to JIA, physician’s evaluation indicating no activity (PhysGA = 0), and morning stiffness < 15 min.
Medication
This study focused on the patients’ past and current use of disease-modifying antirheumatic drugs (DMARDs), including synthetic DMARDs (sDMARDs) and/or biologic DMARDs (bDMARDs). Synthetic DMARDs included methotrexate, hydroxychloroquine, cyclosporine, and mycophenolate mofetil. Biologic DMARDs included etanercept, infliximab, adalimumab, tocilizumab, abatacept, certolizumab, golimumab, and rituximab.
Statistical analysis
To describe the clinical characteristics and disease activity of the cohort, either mean and standard deviation (SD) or median and 1st to 3rd interquartile ranges (IQR) were used for continuous variables. Absolute frequencies and percentages were used for categorical variables. For proportions, we estimated percent point differences with 95% confidence intervals using the prtest command in STATA.
To study patient-reported physical health in the JIA cohort compared to the matched control cohort, the mean Physical Summary Score (CHQ PhS) and the mean Psychosocial Summary Scores of the Child Health Questionnaire (CHQ PsS) of the JIA cohort was compared to the control cohort using t-test for independent samples. CHQ scores were also dichotomized into normal (CHQ ≥ 40) and poor (CHQ < 40) physical or psychosocial health.
To evaluate the association of patient- and physician-reported outcome measures with patient-reported physical disability (CHAQ > 0), we used logistic regression analyses and adjusted for sex, age, disease duration, and Iso-BMI chosen by a priory knowledge, to estimate the adjusted odds ratio (OR) with 95% confidence interval (CI). The CHAQ scores were dichotomized into 0 (no disability) or > 0 (disability) and used as the main outcome variable. The other variables were categorized as follows; VAS pain (0 = no pain, > 0 = pain), PatGA (0 = no disease influence on well-being, > 0 = disease influence on well-being), morning stiffness (< 15 min = no substantial morning stiffness, ≥ 15 min = substantial morning stiffness), PhysGA (0 = no disease activity, > 0 = disease activity), and past and present medication (no DMARDs, DMARDs). We categorized disease status according to Wallace et al. [14, 15] into three condensed levels; remission off medication, inactive disease, and active disease. Remission off medication = remission off any antiarthritic or anti-uveitis medication for ≥ 12 continuous months. Inactive disease = inactive disease on medication < 6 months or off medication < 12 months, or remission on medication (inactive disease on medication for more than six months). Active disease = flare or continuous active disease. JIA categories were dichotomized to oligoarticular persistent JIA or all other JIA categories. Statistical analyses were carried out using STATA version 16, software (STATA Corp., College Station, Texas, USA).







留言 (0)