The patella is a crucial component of the extensor mechanism that aids in knee extension. Patella fractures account for 1% of all fractures and frequently disrupt the extensor mechanism [1]. The surgical treatment aims to repair the extensor mechanism, promote knee function and restores articular congruity to minimize the risk of subsequent knee arthritis [3, 10].
The first and utmost step of patella fractures surgery was reduction, regardless of the kind of devices applied [11, 12]. Traditional reduction technique were relayed using pointed clamps [3, 13]. Nevertheless, there were several limitations and drawbacks during the reduction process using pointed clamps. Firstly, during the reduction process, multiple reduction attempts and intraoperative fluoroscopy may be needed, especially when confronted with a comminuted fracture and without exposing the articular surface. Secondly, it consistently applied the fixation devices after reduction by pointed clamps, and it is possible that a reduction loss may occur during this period. Thirdly, it would be challenging for pointed clamps to effectively secure the fracture segments during reduction of the comminuted fracture [7]. In order to address the aforementioned issues, various reduction strategies were proposed by scholars. Yong and Yin et al. pointed out that a medial parapatellar approach to visualize the patellar articular surface directly was favorable to the surgeries [14, 15]. Gardner et al. believed that a lateral arthrotomy could be used to ensure articular surface congruence and achieve satisfactory clinical results [16]. It has been suggested that due to anatomic and blood supply factors, a lateral arthrotomy may be considered if it is necessary to obtain direct visualization of the articular surface [1]. Nonetheless, the utilization of turn-over reduction techniques is likely to result in an injury to the media/lateral patellar retinaculum, and the lateral incision may pose a potential disadvantage for potential total knee arthroplasty [1]. Furthermore, these methods still required the use of pointed clamps and could only solve partial problems. Besides direct reduction methods, Chen et al. proposed nice knots as an auxiliary reduction technique for displaced comminuted patellar fractures [17]. Jiang et al. presented a three-dimensional strapping reduction technique for the treatment of patellar fractures [7]. It has been revealed that in comparison to towel clamp reduction, the utilization of three-dimensional strapping reduction in the treatment of patellar fractures offers advantages such as a shorter operation time and fluoroscopy time, improved knee function after surgery, and satisfactory fracture healing.
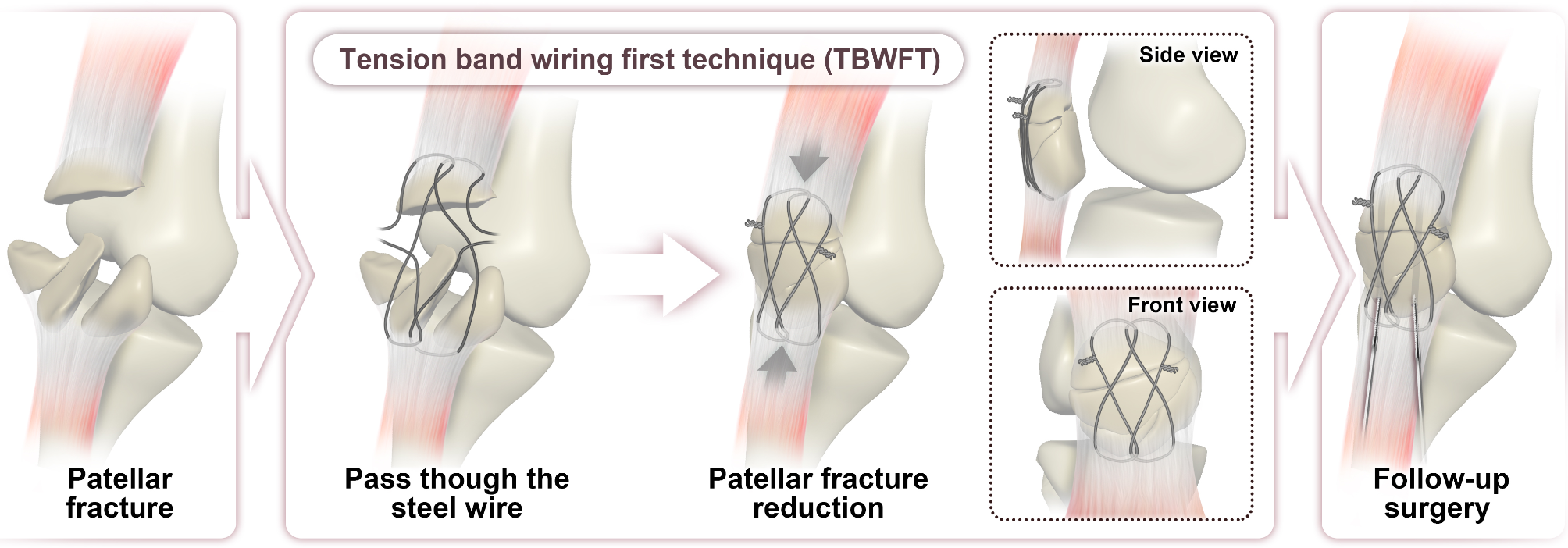
According to the AO Group, the tension band technique has been a mainstay of surgical treatment of patellar fractures [8, 18]. Two parallel K-wires were placed longitudinally through the center of the patella, while a flexible wire was passed posteriorly to the K-wires and was tensioned anteriorly in a figure-of-8 configuration. It was theoretically designed to convert anterior tensile forces into a compressive force across the articular surface as the knee flexed [9]. The tension band wire was typically applied following the reduction of patellar fracture. We proposed that the tension band wire could be applied prior to reduction and utilized as a reduction tool. During the tightening process of the tension band, the wire decreased the distance of fracture segments until they disappeared. Meanwhile, the upper surface of patellar was strongly pulled to the underneath of wire, and the articular surface could get reduced indirectly without exposed the articular surface directly. Our study demonstrated that TBWFT significantly reduced the operative time and X-ray exposure times compared to the TRT group. Additionally, it tended to decrease the articular steps. There are several major advantages to TBWFT. Firstly, it proved to be a time-saving and straightforward technology, particularly for novices. Secondly, it was unnecessary to open the patellofemoral joint, thereby preventing any further artificial damage to the retinaculum. Thirdly, TBWFT utilized the soft tissue around the patella to reduce fracture segments, which is especially suitable for comminuted patellar fractures and avulsion fractures. Fourthly, in our operation, the final fixation mainly relied on titanium cable. Nonetheless, we retained the tension band wiring both during and subsequent to the operation, thereby minimizing the potential for reduction loss prior to cable application. Furthermore, it provided stronger reduction strength compared to “nice knots” and “three-dimensional strapping reduction method” and it provided with additional fixation strength in the presence of titanium cable.
The primary advantage of TBWFT was favorable towards reduction. There is no significant difference between the two groups in bone healing time, knee ROM, or knee function. These results further demonstrated that reduction will determine the final clinical results when the same fixation device is applied.
The main complication of the TBWFT and TRT group was soft tissue irritation, which was associated with the application of tension band devices in our surgery [18,19,20]. However, there was no significant disparity observed between the two groups because we always buried the wire end into soft tissue deep.
This study had several limitations. Firstly, the current study was a short-term retrospective study that involved a limited number of cases from a single institution. It is anticipated that TBWFT will be implemented in other institutions and that a more considerable number of cases will be enrolled. Secondly, there may exist the possibility that TBWFT would display more advantages in treatment of comminuted patellar fractures or C3 type fractures. Therefore, future research might focus on enrolling more cases with C3 type fractures. Thirdly, it was imperative to conclude the biomechanical analysis to evaluate the strength imparted by the supplementary tension band wire. Fourthly, it is reasonable to investigate the utilization of non-metallic suture-based fixation for the reduction and fixation of patellar fractures in order to mitigate the soft tissue irritation induced by metallic implants [21,22,23].









留言 (0)