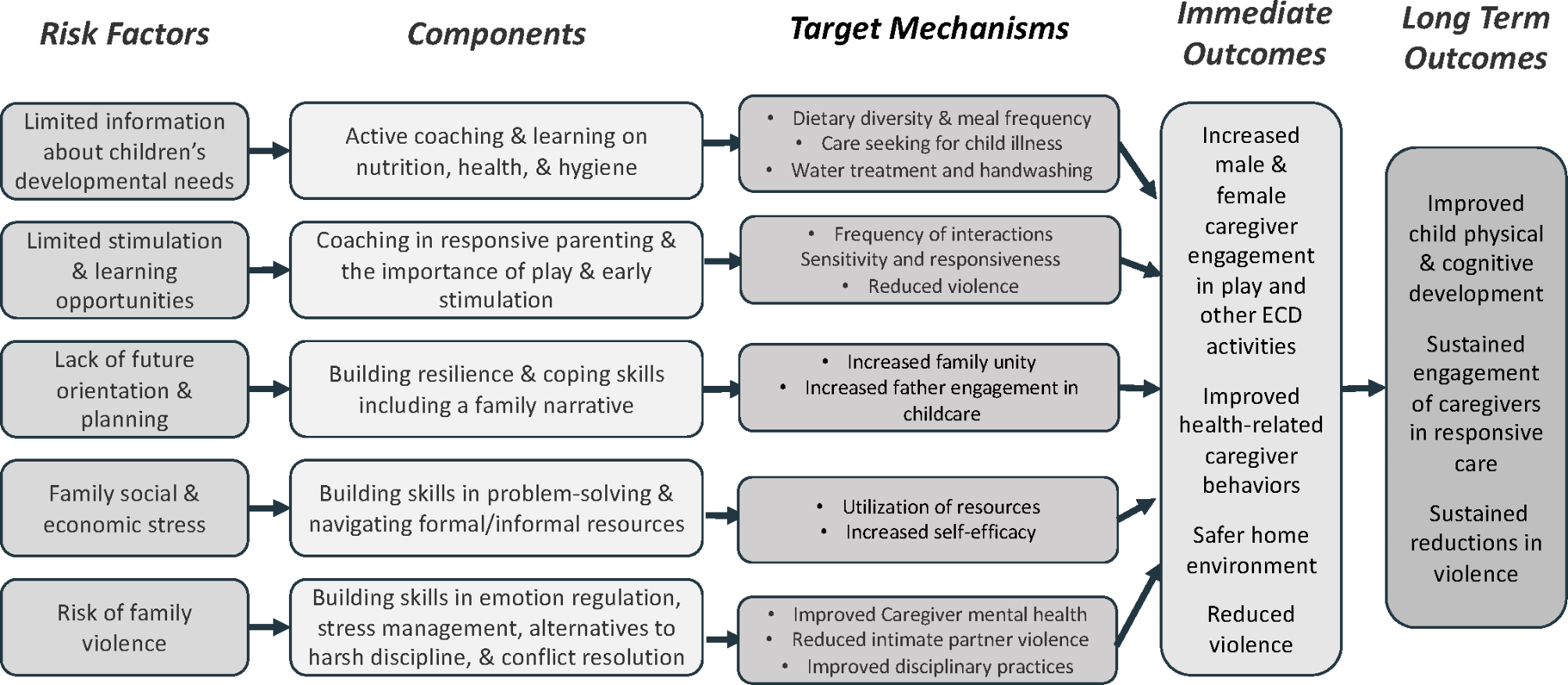
In this comprehensive study, profound insights were gathered through in-depth interviews with both service users with psychosis and caregivers, providing detailed descriptions of the factors contributing to service user disengagement. The findings were grouped into five categories: individual factors, stigma, progression, treatment factors, and external factors. Each category was dissected into distinctive thematic concepts, allowing for targeted interventions if needed. Beyond the primary objective of understanding the reasons for disengagement from an early psychosis intervention programme, the study delved into additional aspects such as types of disengagement, treatment adherence, decision-making processes, and circumstances of re-engagement.
Within the individual factors category, six themes highlighted the importance of acknowledging the unique traits and autonomy of service users. Conflicting findings from previous quantitative studies on symptom severity predicting disengagement [3, 16] were addressed by a proposed bimodal relationship – for patients with higher symptom severity, poor insight into their illness or symptom interference could mediate the relationship with nonadherence to treatment; for those with lower symptom severity, the need to continue treatment may not be as keenly felt by the patients and/or caregivers, leading to a poorer compliance to the treatment routine [17]. This was exemplified in the present study, where only caregivers but not service users reported service user disengagement due to illness symptoms and severity; while many service users considered their symptoms mild, normal, or manageable without conventional treatment. Service users expressed a strong desire for greater autonomy in decision-making, emphasising the need for shared decision-making practices which can potentially enhance patient empowerment and promote user involvement, satisfaction and retention [18, 19]. A Norwegian study revealed that many participants felt excluded from participating in treatment decisions [20], even though they believed they were capable of doing so [21]. Caregivers in the study reported observing high levels of self-efficacy in their service users too, who were confident of their ability to self-manage their diagnosis, with the aid of information they gathered online while researching on their symptoms. As self-efficacy has been associated with health-related quality of life [22] and health literacy [23], this may be considered a desirable outcome; however, it warrants further investigation into whether this sense of confidence is a constructive recovery tool, or simply illness-related denial and lack of insight, which can lead to poor health outcomes. Resource conservation was identified as a theme, with service users wanting to save time and effort by avoiding outpatient appointments. This suggests a need to explore ways to increase service accessibility and better value alignment with patients. Additionally, commitments such as school or work were identified as barriers to treatment adherence, prompting the need for measures to accommodate service users’ real-life responsibilities. While online interventions show promise, further research is necessary to tailor them to service user needs and ensure that similar challenges of sustaining engagement does not carry over onto virtual platforms [24].
Stigma was identified as the second category, encompassing structured discrimination, interpersonal stigma, label avoidance, and self-stigma. Structured discrimination has been discussed in previous studies, where disclosing a mental illness diagnosis was seen as disadvantageous as it may create unfair performance expectations [25], or result in unequal renumeration and reduced chances for advancement [26]. This has important implications, especially since functioning level and employment status is an important measure of social impairment and outcome of treatment [27]. The remaining three stigma themes were congruent with the Mental Illness Stigma Framework (MISF) conceptualised by Fox and colleagues [28] and reflect pervasive and prevalent obstacles service users encounter while navigating society, which affect their engagement rates with intervention services. Stigma-reduction efforts should thus target a range of factors at different levels to be effective – for example, employing anti-discrimination policies in workplaces (structural discrimination), targeting harmful beliefs, attitudes, and actions through community dialogues (interpersonal stigma), providing effective psychoeducation to promote acceptability of mental conditions (label avoidance), and facilitating and strengthening sources of social support (self-stigma) [29, 30]. Further research is to understand the intersection of various stigma forms and their impact on service users; as reflected in Fox and colleagues’ findings, there is substantial heterogeneity in how people experience and respond to being stigmatised [28, 31].
The third category, progression, introduced themes of perceived improvement and moving on. Two users expressed some surprise or disagreement when their disengagement was brought up, responding that the reduction in contact with the service as they progressed was natural and aligned with their expectations of returning to school or work. This is consistent with Tindall and colleagues’ reactive disengagement concept, where positive life changes make continued engagement less prioritised against other commitments [9]. Contrary to the view that disengagement is exclusively negative, perceived improvement suggests it could be a positive outcome, albeit potentially uninformed. Users feel their initial treatment needs are met, and further engagement is redundant. Caution is needed to ensure this well-being improvement is genuine and not a denial of symptoms. Meanwhile, participants who express a desire to “move on” report discontinuing help-seeking after traumatic events related to symptoms or service experiences. Understandably, the onset of psychosis is described to be distressing, potentially leading to secondary symptoms resembling posttraumatic stress disorder [32]. Involuntary hospitalisation and restraint contribute to intense feelings of shame and helplessness, resulting in formidable barriers to continued engagement [33]. Service providers play a crucial role during treatment, helping users navigate hospitalisations, understand and manage their illness with minimal traumatic complications, and prevent hazardous premature disengagement. Care models like shared decision-making and trauma-informed care can support this [34].
Treatment factors constituted the fourth category, revealing negative experiences with medications, treatment teams, hospital environments, and appointment mechanisms. Medication side effects and unpleasant interactions with staff were highlighted. The integration of comprehensive monitoring tools [35] and management strategies [36] into pharmacological strategies during clinical consultations may improve medication adherence [37]. Other negative treatment experiences included unpleasant interactions with the treatment team or hospital staff where users felt disrespected, and frightening memories of being in the hospital. Witnessing floridly disorganised or aggressive behaviours exhibited by other patients was reported as traumatising. The hospital environment was viewed as scary or too clinical, hindering recovery. These highlight the need for urgent and systematic improvements to inpatient mental health settings, as well as regular client satisfaction surveys and interventions to address poor therapeutic alliance before disengagement occurs. Even though the usage of patient reported outcome measures are on the rise, these methods of measuring patient satisfaction and feedback are conventionally quantitative in nature and prone to clustering or ceiling effects, which could restrict the discriminative ability of results to detect potential sources of service user discontentment [38]. As such, the use of mixed methods approaches may be better suited to elicit meaningful descriptions of service gaps that may be easily overlooked or neglected by service providers [39]. Another theme revealed under treatment factors was a perceived lack of quality or sufficient information provided by the treatment team, which led to dissonance or a perceived breach of trust, culminating into eventual disengagement. Service users complained of not fully understanding their diagnoses and treatment implications. Tiered, curated, and personalised educational materials [40], patient empowerment through shared decision-making approaches [41], and the provision of alternative communication platforms are potential solutions. Some service users also questioned the effectiveness of interventions and felt that their symptoms were not addressed. These participants were motivated to get better but were frustrated by the lack of progress or improvement. Understanding patients’ goals, providing tailored psychoeducation and treatment, and managing expectations are critical in addressing this issue. Finally, some users received treatment only when coerced by their family or mandated by the law, ceasing engagement immediately upon discharge. For involuntarily admitted or coerced patients, maintaining a working (and perhaps even transactional) relationship and equipping them or their caregivers with information and tools for symptom and crisis management is crucial. It may be necessary at the initial stages to state explicitly the conditions leading to involuntary treatment so that the patient understands the legalities, and a common goal of preventing a recurrence of involuntary admission can be established. When opportunities arise for reparation of therapeutic alliance, it is important for the treatment team to acknowledge the patient’s anger with autonomy violation, so that honest conversations can ensue, and foundations can be built for improved engagement with the aim of building intrinsic motivation for recovery.
In the last category, external factors, two key elements were identified: the adoption of non-medical approaches and the impact of the COVID-19 pandemic. Some users found symptom relief through religious or alternative methods, and some with the support of their caregivers. Previous studies have illustrated that turning to religion or alternative methods have also been shown to be common coping strategies in service users and their families [42, 43], emphasising the need to recognise, respect, and harmonise pre-existing spiritual needs in psychosocial care [44]. The pandemic disrupted clinical operations, limiting face-to-face interactions and reducing engagement between the EPIP clinical team and users. The resulting panic and paranoia had widespread consequences on mental health and contributed to the development of new psychiatric symptoms or exacerbation of existing ones [45, 46], necessitating the development of future contingency plans to address critical user needs during global crises [47].
Overall, negative experiences emerged as the primary reason for disengagement, among both service users and caregivers. Lack of treatment effectiveness, perceived improvement, and other commitments were reported frequently among service users, while label avoidance, illness denial, and general unwillingness and personal autonomy were endorsed more often by caregivers. Interestingly, comparison between service user and caregiver dyads revealed varying agreement on reported themes. While some pairs aligned on themes like other commitments, interpersonal stigma, label avoidance, and non-medical model, others presented divergent perspectives. Due to the exploratory nature of this study, microscopic themes were developed while the categories were kept broad and open for future interpretation and application. It is not the goal of the present study to recommend addressing all themes concurrently to minimise disengagement; in fact, the aim of discussing and inspecting these findings is to highlight and bring awareness to the complex and multi-faceted nature of the engagement process. More work is required in order to narrow down or efficiently and feasibly elicit urgent areas of attention, such as cross-examining the resulting themes from this study together with risk factors already established in the literature and the economic or individual burden of disengagement.
Limitations
The cross-sectional nature of data collection, which was captured sometime after disengagement has occurred, makes it prone to recall and hindsight bias. A prospective design capturing real-time events could enhance accuracy [9]. Secondly, the exclusion criteria may have limited perspectives, especially from those with florid symptoms or explicit hostility, potentially missing certain viewpoints. As noted by Doyle [3], true engagers who refused any sort of contact with the service would not be captured and their opinions would remain out of reach. To mitigate this, attempts were made to include those who had disengaged but returned and involve caregivers to present a more comprehensive view. As this was the first study (to the best of the authors’ knowledge) to discuss disengagement with service users explicitly, the topics covered were broad. The semi-structured nature of interviews allowed organic content generation, limiting time for prompting and verification of themes outside of those self-generated by participants. Both groups of participants had vague and loose definitions of disengagement, which while representative of the emic perspective, resulted in the study team having to sometimes infer when and how the intention to disengage arose. Future studies should include focus group discussions to firm up this definition, which is a sentiment echoed in previous studies. These focus group discussions can then also examine and assess the current model of care provided to service users and caregivers, to introduce a more user-centric approach in designing these early interventions. These sessions would also be a suitable platform to discuss the acceptability and validation of the themes elicited from this study, by adding in cognitive interview techniques.
Another limitation was the intentional choice of a single interviewer to ensure standardisation of the content and format of each interview session. However, during the interviews, participants sought reassurance that confidentiality would be ensured and that they were free to share their opinions without repercussions, before delving into sensitive topics. This, together with the honest and negative feedback collected from the participants suggested that undue influence on the participants’ responses was successfully minimised. Lastly, while previous literature has explored substance abuse as a significant predictor of disengagement, this was not elicited or explored in the present study due to the stringent anti-drug laws in Singapore [48].









留言 (0)