
記住我
Negative emotions are generally indicative of distress and are often conceptualized in varying intensities, such as anxiety, depression, sadness, and anger (1). Among these, depression and anxiety are frequently employed as predictors (2). Depression is often a chronic and recurring condition (3) associated with high levels of psychological distress, impairments in functioning, and poor physical health (4). Depression is the most predominant aspect of negative affect and a major contributor to the global burden of disease in young people under the age of 25 (5). It is estimated that one in five people will be affected by depression in their lifetime, and the majority of people with depression begin to experience the onset of the illness in adolescence to young adulthood (6, 7). Anxiety is the most common manifestation of psychopathology in youth, negatively affecting academic, social, and adaptive functioning and increasing risk for mental health problems into adulthood (8, 9). Approximately 1 in 4 adolescents exhibits increased levels of worry and anxiety. In addition, adolescent anxiety predicts ongoing mental health problems throughout life (10). Therefore, depression and anxiety are the most important aspects of negative emotions, and this study also focuses on these two aspects of negative emotions.
Adolescence, a period characterized by rapid growth and maturation, neuronal plasticity (11, 12), identity formation (13), and the establishment of behavioral tendencies, plays a crucial role in shaping mental well-being, potentially steering it in either positive or negative directions (14, 15). During this critical phase, individuals experience significant physical, psychological, and social development, which makes them particularly susceptible to negative emotional states influenced by various factors. Adolescence brings profound changes in the social environment, physical growth, and dramatic hormonal changes (16, 17). Behaviorally, adolescence is also accompanied by constant emotional changes (relative to childhood and adulthood), which can trigger more extreme emotional responses for at-risk individuals (18). Numerous studies have revealed that the incidence of negative emotions escalates considerably during adolescence, surpassed only by behavioral disorders (19–21). The predominant clinical manifestations of negative emotions in adolescents encompass apathy, somatic complaints, impaired concentration, indecision, overwhelming guilt, reckless behavior, disinterest in food or compulsive overeating, resulting in significant weight fluctuations, memory lapses, fear of death, defiance, pervasive sadness, anxiety, or despair, nocturnal insomnia, and excessive daytime drowsiness (22). It is therefore not surprising that adolescence is also a time when emotional symptoms such as anxiety and depression are often present. These emotional states not only exacerbate psychological suffering and impair the mental health of adolescents but are also closely associated with deliberate or inadvertent harmful behaviors (15, 23), such as smoking (24), drinking (25), and other detrimental activities. Hence, it is logical to conclude that an adolescent’s environmental exposure could mitigate the development of negative emotions later in life (26).
Physical exercise (PE) encompasses aerobic activity, resistance training, as well as both physical and mental exercises (27). Numerous studies have revealed that engaging in physical activity not only bolsters mental health but also mitigates negative emotions and diminishes the risk of mental disorders (28, 29). For example, regular and appropriate PE has the potential to transform the brain’s structure and function, thereby ameliorating negative emotional states by increasing levels of dopamine, serotonin, and norepinephrine (30). Scholars have also established a correlation between adhering to the three recommended 24-hour activity guidelines and a reduced risk of depression and anxiety (31). Research conducted among school-aged children in China indicated that those who adhered to the 24-hour activity standards exhibited the lowest risk of experiencing negative emotions (32). According to findings from Wang’s study, a six-week regimen of PE has proven effective in alleviating symptoms of depression among adolescents aged 12 to 18 (27).
Research on negative emotions in adolescents is limited. Considering the influences noted in earlier studies and adolescents’ natural emotional sensitivity, alongside the positive impacts of PE interventions on their emotional well-being, our study aimed to investigate negative emotions in individuals aged 10 to 19 years. We conducted a meta-analysis of existing literature to examine how the duration, time, and frequency of PE interventions affect study outcomes. Based on this, the hypothesis of this study was formulated: This study hypothesizes that physical exercise interventions will significantly reduce symptoms of anxiety and depression in adolescents.
2 MethodsFollowing the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) (33) and the Cochrane Handbook for Systematic Reviews and Meta-Analysis (34), this review was conducted. Moreover, the protocol for this review was duly registered on PROSPERO under the registration number CRD42024534375.
2.1 Search strategyFor this study, we searched PubMed, Web of Science, EBSCO, Cochrane, and Embase up to April 11, 2024. The main search terms were physical exercise, negative emotions, adolescents, randomized controlled trials, etc., and the search terms were connected by AND and the search terms were connected by OR. The search strategy was a Boolean logic search with the following search strategies: (“physical activity” or “physical exercise” or “sports activities” or “physical education” or “sport movement”, sport or “athletic sports” or “aerobic exercise” or “aerobic training” or “resistance exercise”, “muscle-strengthening exercise” or “strength training”, “fitness game”) AND (“negative emotion” or anxiety or anxious or depression or depressive or depress or pressure or stress or “psychological ill-being” or “mental disease”) AND (adolescent or teenager or “junior high school students” or “senior high school students”) AND (“randomized controlled trial” or RCT). The details of our search terms are outlined in Table 1, demonstrating the meticulousness and accuracy of our research approach. The study was conducted independently by two researchers (TW and WCL), with a third researcher (YFL) consulted in case of disagreement. In this case, WCL performed the first stage of screening based on the title and abstract, and TW performed the second stage of screening by reading the full text. Finally, the data were analyzed by TW, WCL, and JXD and supervised and reviewed by QBZ and YFL.
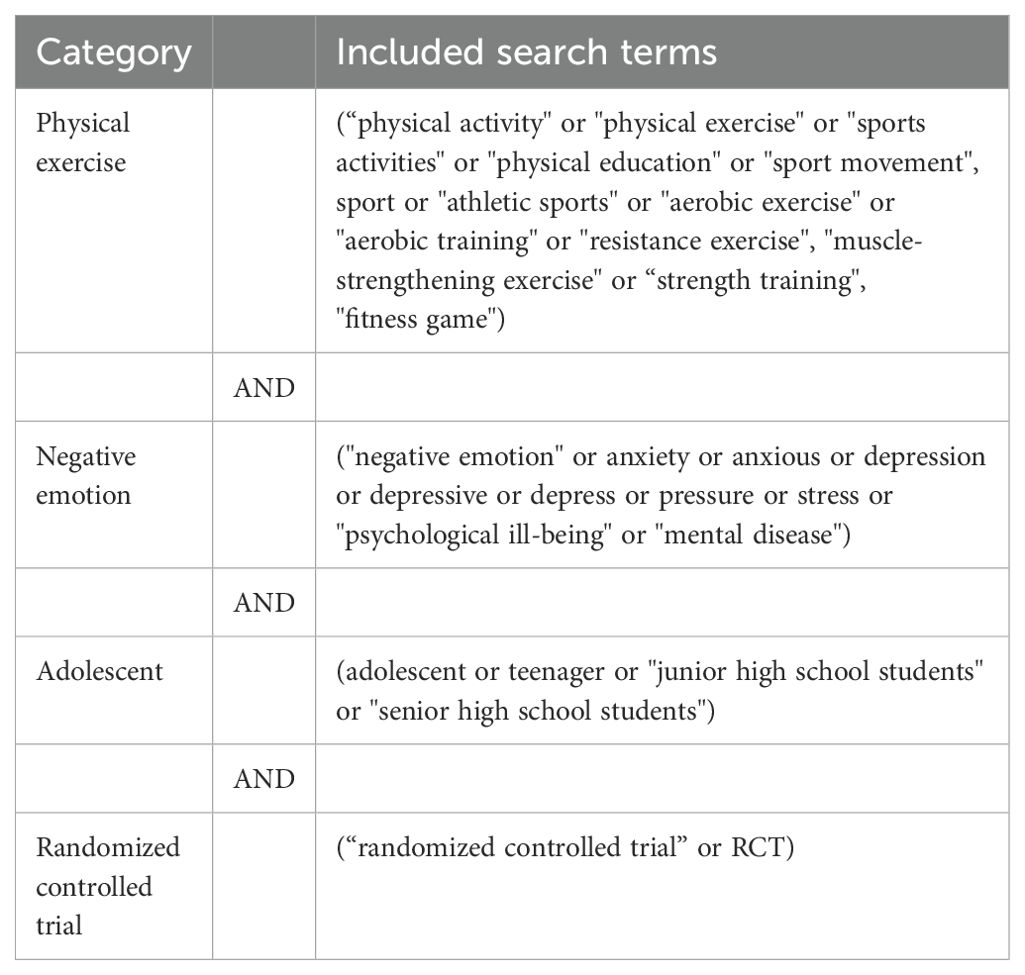
Table 1. Summary of search terms.
2.2 Eligibility criteriaThe relevant studies’ inclusion criteria were established following the PICOS framework. For participants (P), studies involving adolescents aged 10 to 19 years were considered. Regarding Intervention (I), the experimental group received various forms of PE intervention. Comparison (C) groups encompassed no-exercise (NT), wait-list (WL), and attention/activity placebo (AP) conditions. Outcome (O) measurements are primarily focused on assessing negative emotions in adolescents. Lastly, Study Design (S) adhered to the randomized controlled trial methodology.
The following criteria were applied to exclude relevant studies: literature not in English, including unpublished materials, theses, and reviews; studies involving adults, animals, or special populations; literature lacking valid data extraction; duplicate publications; and full texts that were inaccessible.
2.3 Data extractionThe study followed the PRISMA statement guidelines when extracting data and selecting studies. Duplicate studies were eliminated using EndNote 20 software to consolidate articles from each source into a unified database. Data extraction was mainly carried out independently by two researchers (TW and WCL), with a third researcher (YFL) being consulted in case of disagreement. Data were analyzed by TW, WCL, and JXD and supervised and reviewed by QBZ and YFL. Investigations into the attrition of treatment during follow-up were conducted independently by two researchers (TW and QBZ), who examined the included literature and consulted a third researcher (YFL) in cases of discordance. When data cannot be extracted, we will contact the author of the article to resolve the issue. If we cannot get in touch, we will extract the data using WebPlotDigitizer software.
Utilizing Review Manager 5.3 (35), data were inputted for both intervention and control groups, encompassing mean values, standard deviations, and participant counts. To accommodate the anticipated heterogeneity between trials attributed to the implementation of diverse PE interventions, meta-analysis pooling was conducted using a random effects model. To facilitate the aggregation of data from various negative emotions symptom scales, the effect was evaluated as the standardized mean difference (SMD), calculated using Hedges’ g, adjusted for small sample size bias, accompanied by 95% confidence intervals (CI) (36), and heterogeneity was evaluated through standard parameters of the I2 statistic (34). In cases where the test indicated substantial heterogeneity (I2 > 50%), we employed subgroup analysis and sensitivity analysis to elucidate the findings (37).
Subgroup analysis was utilized to investigate potential factors influencing the impact of PE on negative emotions. Pre-specified subgroup objectives were type of negative emotions (depression vs. anxiety), type of control group (WL/NT vs. AP), type of exercise intervention (aerobic vs. resistance vs. mixed), exercise intervention duration (<12 weeks vs. ≥12 weeks), exercise intervention time (<60min vs. ≥60min), exercise intervention frequency (≤3 times per week vs. >3 times per week).
2.4 Methodological quality assessmentThe included studies were independently quality assessed using the Cochrane Risk of Bias Tool (38) by researchers TW and WCL, respectively. In this process, consensus is sought through in-depth discussion of any disagreements that arise in the assessment. If there were disagreements that could not be resolved through discussion, a third reviewer (CY) was consulted to ensure the objectivity and accuracy of the results. The methodological quality of the included studies was evaluated using the Cochrane risk of bias criteria, comprising seven items: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other biases. Each item was assessed as “low risk”, “uncertain risk”, or “high risk” based on the responses to the signaling questions, contributing to an overall judgment of bias for each study assessed.
3 Results3.1 Study selectionThe literature search results and research selection process are shown in Figure 1. Initially, 3368 articles were retrieved from the databases, of which 1156 were from Pumbed, 635 from Embase, 1063 from Cochrane, 406 from Web of Science, and 108 from EBSCO. Following the removal of duplicates, 2271 studies remained, while 2193 studies did not meet the eligibility criteria during the title and abstract screening phases. These ineligible papers covered reviews (n = 106); not relevant studies (n = 1882); animal experiments (n = 1); reports, cross-sectional studies, longitudinal studies, and other articles (n = 181); and alcohol/tobacco and other articles (n = 23). Out of 78 studies, 63 were excluded after reading their full texts: no data (n = 3); non-English (n = 3); unable to access original text (n = 6); experimental design discrepancy (n = 3); incorrect age (n = 20); intervention discrepancy (n = 9); and outcome index discrepancy (n = 19). A total of 15 articles were eventually included in the meta-analysis.
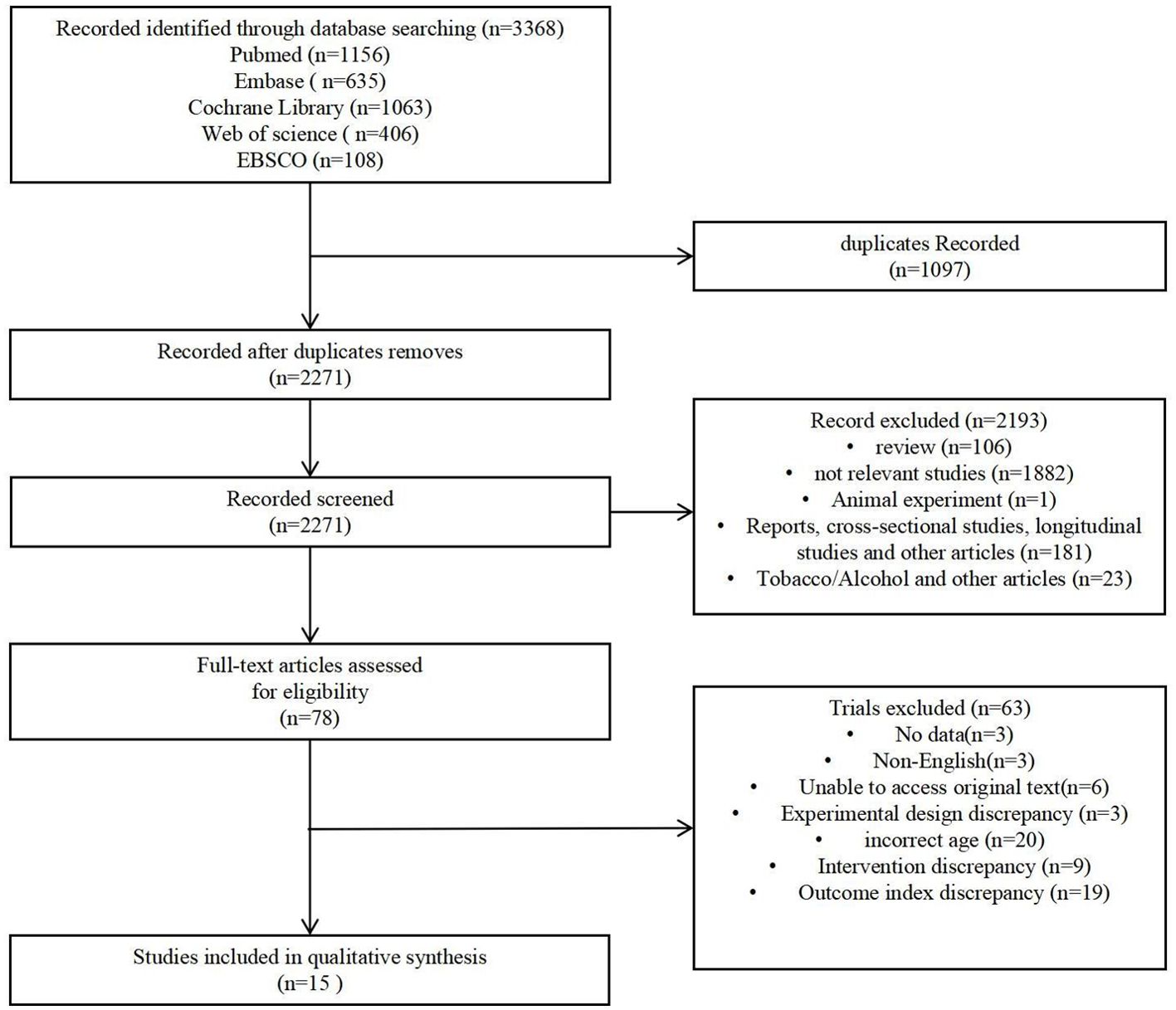
Figure 1. Flow chart of literature retrieval.
3.2 Study characteristicsAs illustrated in Table 2, the sample sizes of the trials ranged from 24 to 1066 participants, with mean ages spanning from 12 to 18.8 years. Two studies included subjects with a healthy mental status, seven studies included subjects with an unhealthy mental status, and six studies did not report the mental status of the included subjects. A summary of the characteristics of the PE interventions implemented in each trial is provided in Tables 2 and 3. The majority of trials employed aerobic exercise, though there was significant variation in the types of PE. The duration of the interventions varied between 6 to 48 weeks, with sessions occurring 1 to 5 times per week. The time commitment per session ranged from 20 to 440 minutes. The control groups consisted of NT (n = 3), WL (n = 3), and AP (n = 8). Ten studies used per-protocol analysis, and five studies used intention-to-treat analysis.
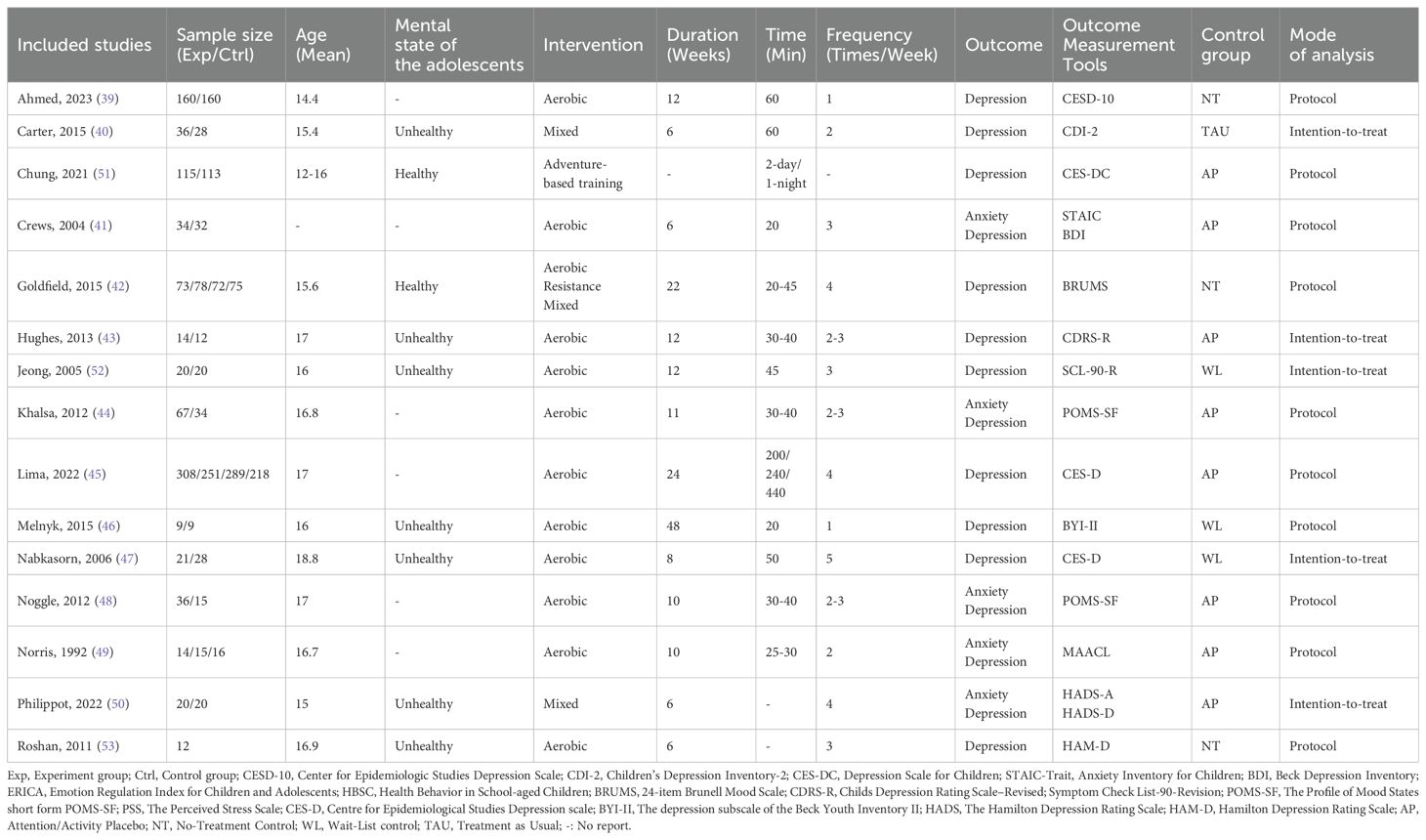
Table 2. Included trial characteristics.
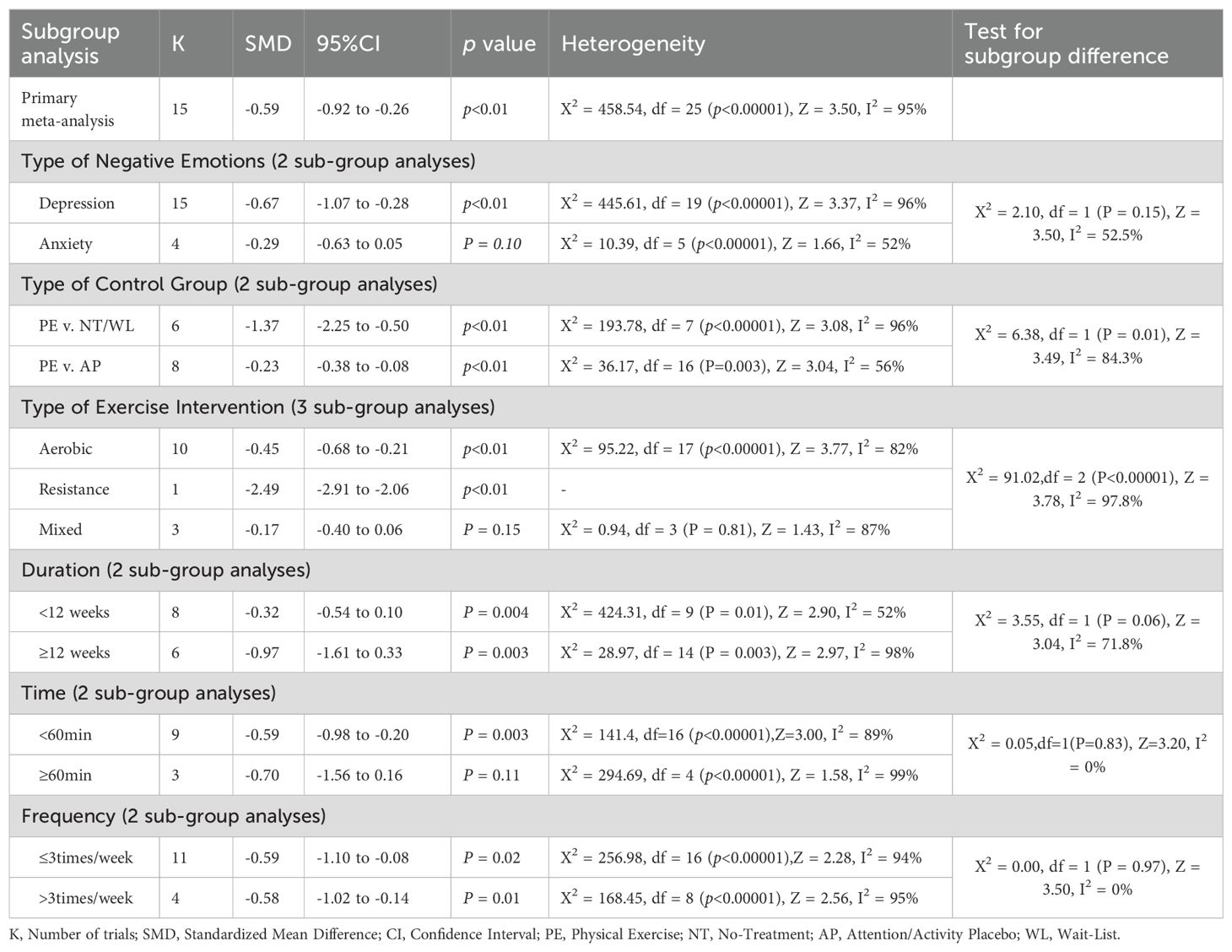
Table 3. Subgroup analyses based on the primary meta-analysis.
3.3 Risk of biasThe methodological quality of the included literature was assessed using the Cochrane Risk Assessment Tool. For random sequence generation, 12 articles (39–50) were rated as low risk and 3 articles (51–53) as unclear risk. For allocation concealment, 13 articles (39–43, 45–52) were rated as low risk, 1 article (53) as unclear, and 1 article (44) as high risk. Regarding performance bias, 2 articles (46, 50) were rated as low risk, 3 articles (39, 41, 47) as unclear risk, and 10 articles (40, 42–45, 48, 49, 51–53) as high risk. Regarding detection bias, 4 articles (42, 43, 46, 50) were rated as low risk, 4 articles (39, 41, 47, 53) as unclear, and 7 articles (40, 44, 45, 48, 49, 51, 52) as high risk. For attrition bias, 11 articles (39, 42–47, 49–52) were rated as low risk and 4 articles (40, 41, 48, 53) as unclear risk. Regarding reporting bias, 10 articles (39, 40, 42–47, 50, 51) were rated as low risk, 4 articles (41, 48, 49, 53) as unclear risk, and 1 article (52) as high risk. Finally, with regard to other biases, 6 articles (39, 40, 43, 45, 47, 50) were rated as low risk, 8 articles (41, 42, 44, 46, 48, 49, 51, 53) as unclear risk, and 1 article (52) as high risk (Figure 2). The assessment of publication bias in the included studies was performed visually through an analysis of the funnel plot (Figure 3, Supplementary Figure 1). The funnel plot analysis reveals notable asymmetry, indicating potential publication bias. This asymmetry suggests that smaller studies with non-significant results may be underrepresented, consequently inflating the true effect size in our meta-analysis. Beyond publication bias, discrepancies in study design, including variations in sample size, methodology, and population characteristics, may also contribute to the observed asymmetry. Smaller studies often exhibit more variable effect sizes, further compounding the asymmetry.
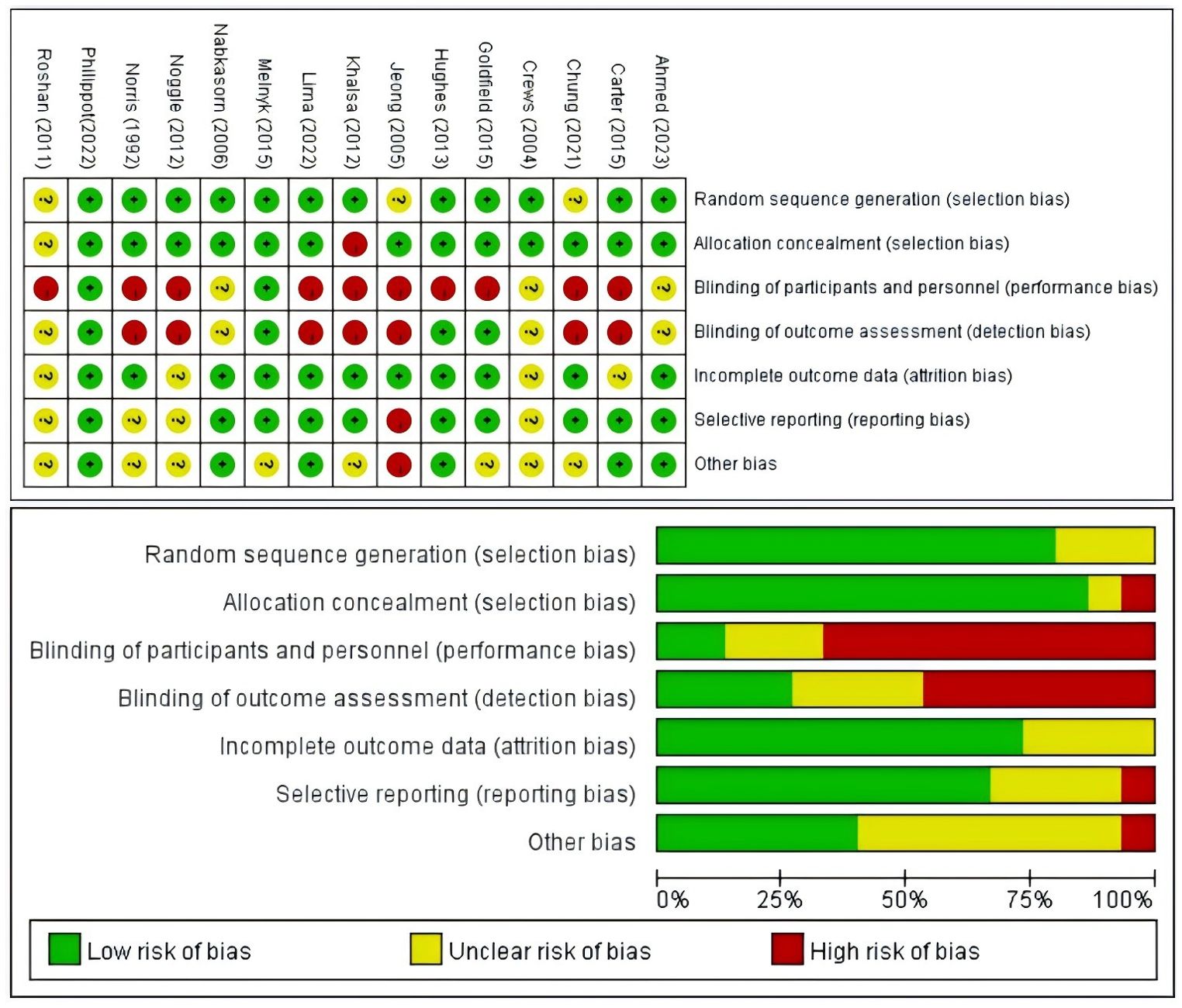
Figure 2. Results of the Cochrane risk of bias tool.
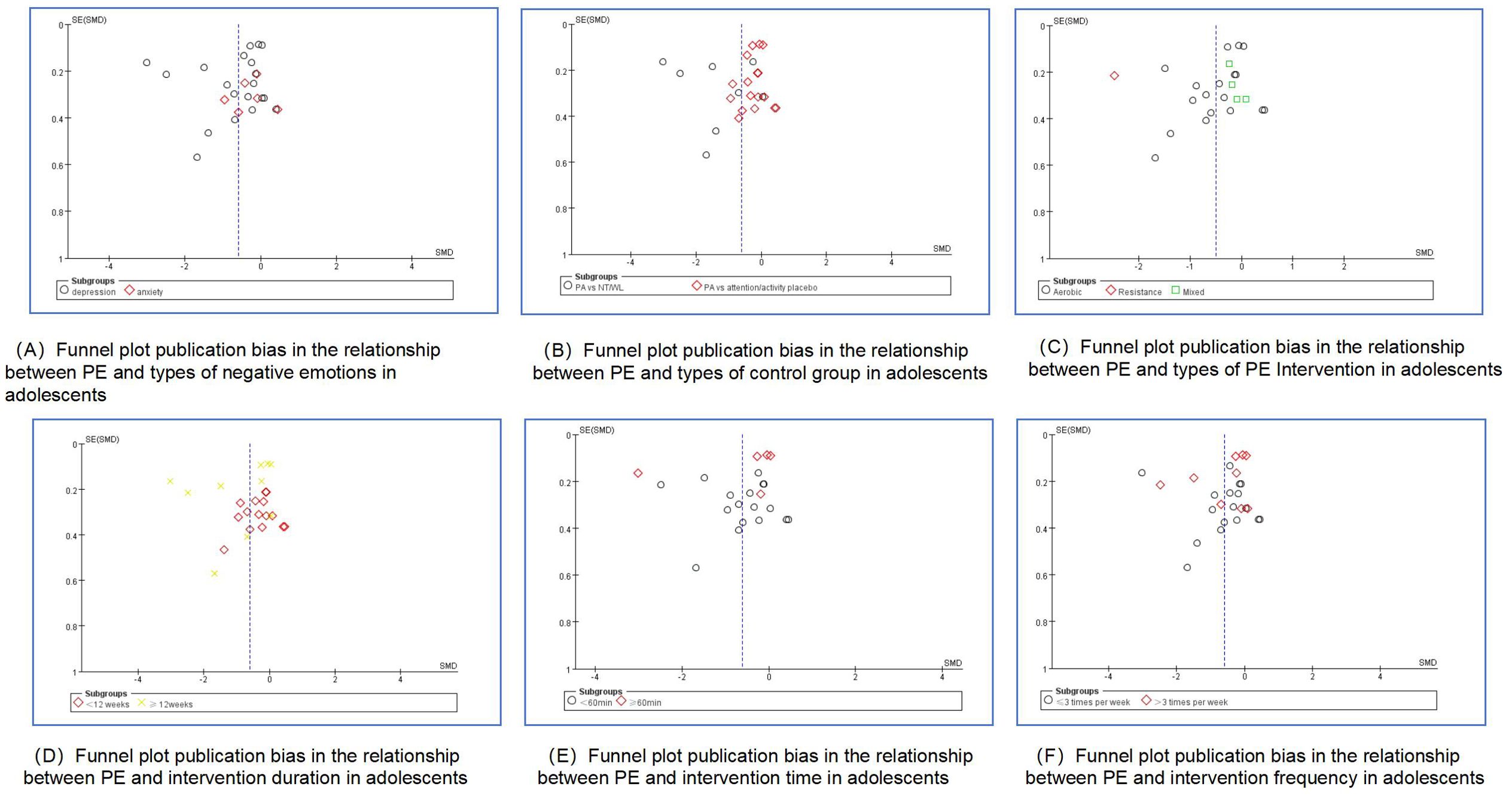
Figure 3. Funnel plot publication bias in the relationship between PE and negative emotions in adolescents (Subgroup analysis).
3.4 Meta-analysis resultsIn evaluating the effects of PE on negative emotions in adolescents, fifteen studies utilized negative emotions, such as depression or anxiety, as outcome measures. Initially, these studies were tested for heterogeneity, revealing substantial differences among them (I² = 95% > 50%, p < 0.01). A high degree of heterogeneity (I² = 95%) in a meta-analysis indicates substantial variability across studies, likely due to differences in study populations, methodologies, contexts, or statistical issues. This variability can arise from factors like demographic differences, variations in interventions, study settings, and potential biases in publication. The implications are significant, as it suggests that the pooled results may not accurately reflect the true effect, limiting the generalizability of the findings. Therefore, we used a random-effects model and a way to minimize heterogeneity by dividing the subgroups. The meta-analysis, depicted in Supplementary Figure 2, demonstrated a significant improvement in negative affect in the PE intervention group compared to the control group (SMD = -0.59, 95% CI: -0.92 to -0.26, p < 0.01, Z = 3.50, I² = 95%). This indicates a notable reduction in negative emotions among adolescents who engaged in PE.
3.5 Sensitivity analysisSensitivity analyses were conducted to further explore the sources of heterogeneity. The process involved systematically excluding individual studies from the analysis one at a time to assess their impact on the overall results. Factors such as study design, sample size, and quality scores were considered in these analyses to determine their potential influence on heterogeneity. The results obtained after each exclusion were consistent with the initial analyses, indicating that no single study significantly affected the composite results. This consistency suggests that the composite effect size in this study is stable and robust.
3.6 Subgroup analysisTo explore potential modifications of PE effects on negative emotions, a subgroup analysis (Table 3) was conducted to assess the influence of specific factors. We divided the subgroups according to the Physical Activity Guidelines for Americans (54), a document that requires that the majority of the 60 minutes or more per day for children and adolescents should be moderate-intensity or vigorous-intensity aerobic exercise and should include vigorous-intensity physical activity at least 3 days per week. Therefore, the objectives of the subgroup analysis in this study were to determine the type of negative emotions (depression, anxiety), type of control group (WL/NT, AP), intervention type (aerobic, resistance, mixed), exercise intervention duration (<12 weeks, ≥12 weeks), intervention time (<60min, ≥60min), intervention frequency (≤3 times/week, >3 times/week).
3.6.1 Types of negative emotionsA total of 15 studies were included (Figure 4). 15 studies (39–53) provided data on the effect of PE intervention on adolescent depression; 4 studies (41, 44, 48–50) provided data on the effect of PE intervention on adolescent anxiety. A random-effects model was employed for the meta-analysis, revealing that the PE intervention had a pronounced impact on adolescent depression (SMD = -0.67, 95% CI = -1.07 to -0.28, p < 0.01, I² = 96%), whereas its effect on adolescent anxiety (SMD = -0.29, 95% CI = -0.63 to 0.02, p = 0.05, I² = 52%) was not statistically significant.
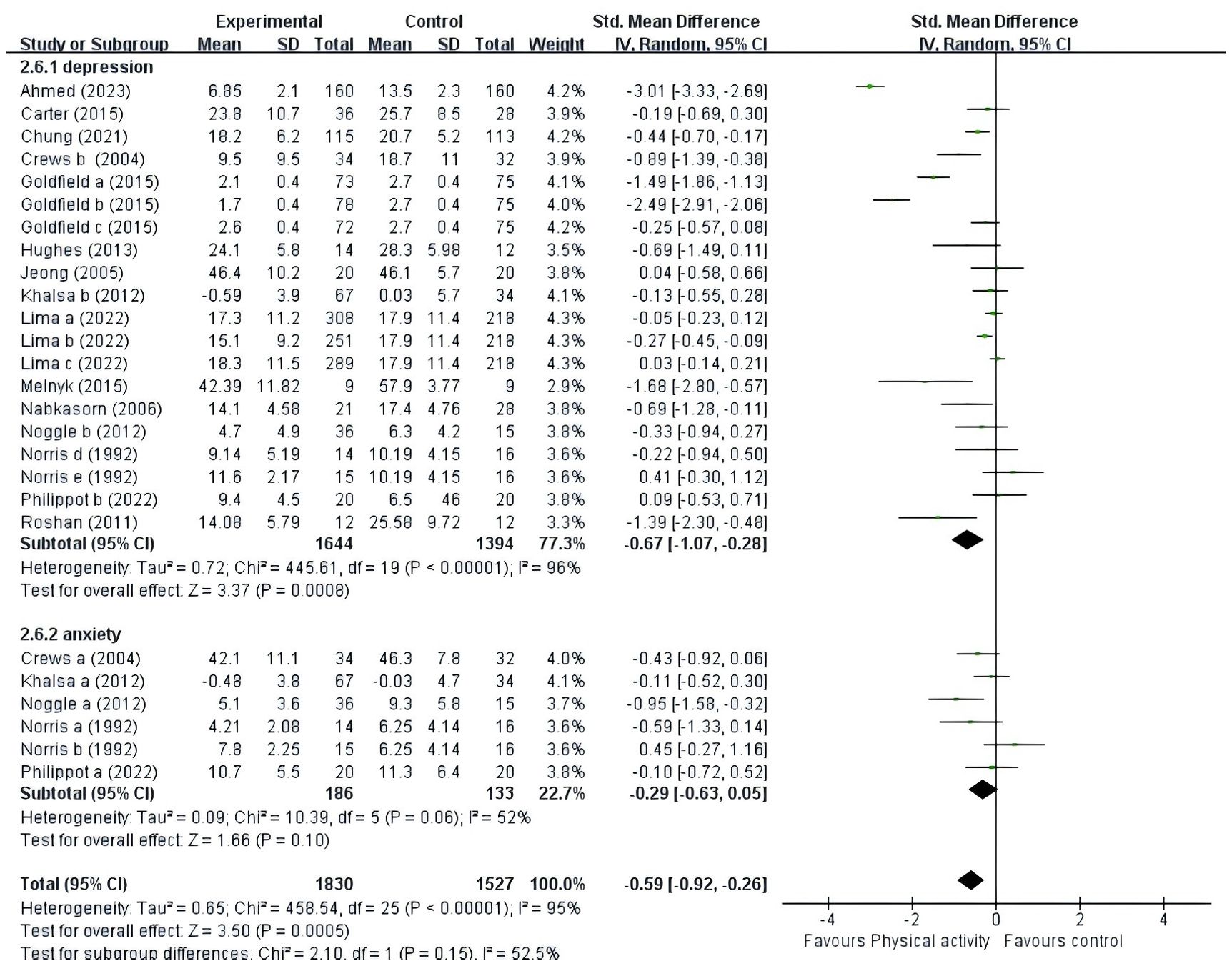
Figure 4. Forest plot of a meta-analysis of the relationship between PE and negative emotions after the intervention.
3.6.2 Types of control groupsA total of 14 studies were included (Figure 5). Six studies (39, 42, 46, 47, 52, 53) provided data on the type of control group that was the NT or WL group, and eight studies (41, 43–45, 48–51) provided data on the type of control group that was the placebo group. The results showed that PE improved negative emotions significantly in both the NT/WL (SMD = -1.37, 95% CI = -2.25 ~ -0.50, p<0.01, I2 = 96%) group and the AP group (SMD = -0.23, 95% CI = -0.38 ~ -0.08, p<0.01, I2 = 56%).
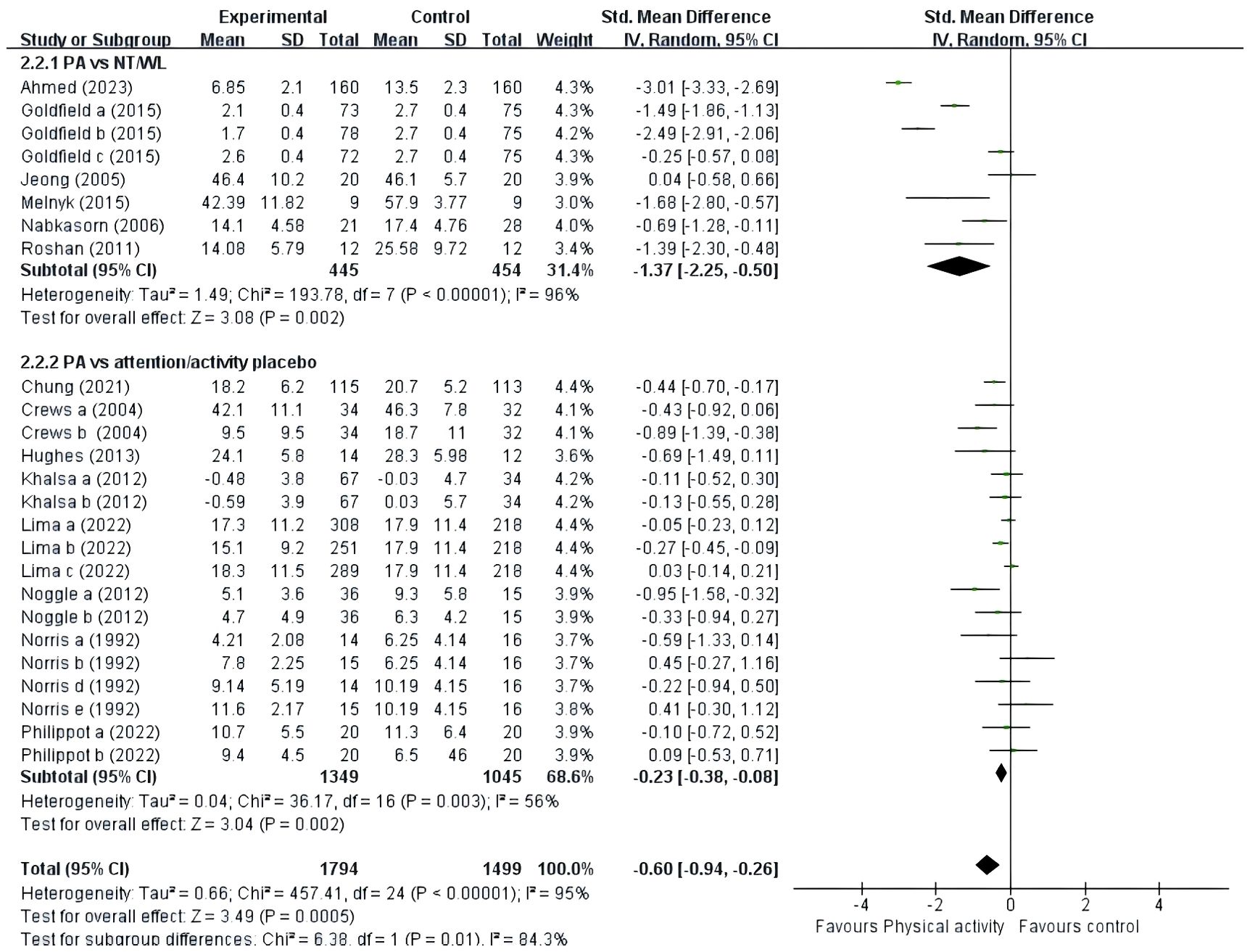
Figure 5. Forest plot of a meta-analysis of the relationship between PE and types of control group after the intervention.
3.6.3 Types of PE InterventionA total of fourteen studies were included (Figure 6). Ten studies (41–49, 53) provided data for aerobic exercise; one study (42) provided data for resistance exercise; and three studies (40, 42, 50) provided data for mixed exercise. Subgroup analyses showed that aerobic exercise (SMD = -0.45, 95% CI = -0.68 ~ -0.21, p < 0.01, I2 = 82%) and resistance exercise (p < 0.01) significantly improved negative mood. However, mixed exercise (SMD = -0.17, 95% CI = -0.40 ~ -0.06, p = 0.15, I2 = 0%) was not significantly associated with negative mood in adolescents. Only one article on resistance exercise intervention was included, so the results should be interpreted with caution. Therefore, aerobic exercise had a significant effect on the improvement of negative mood in adolescents.
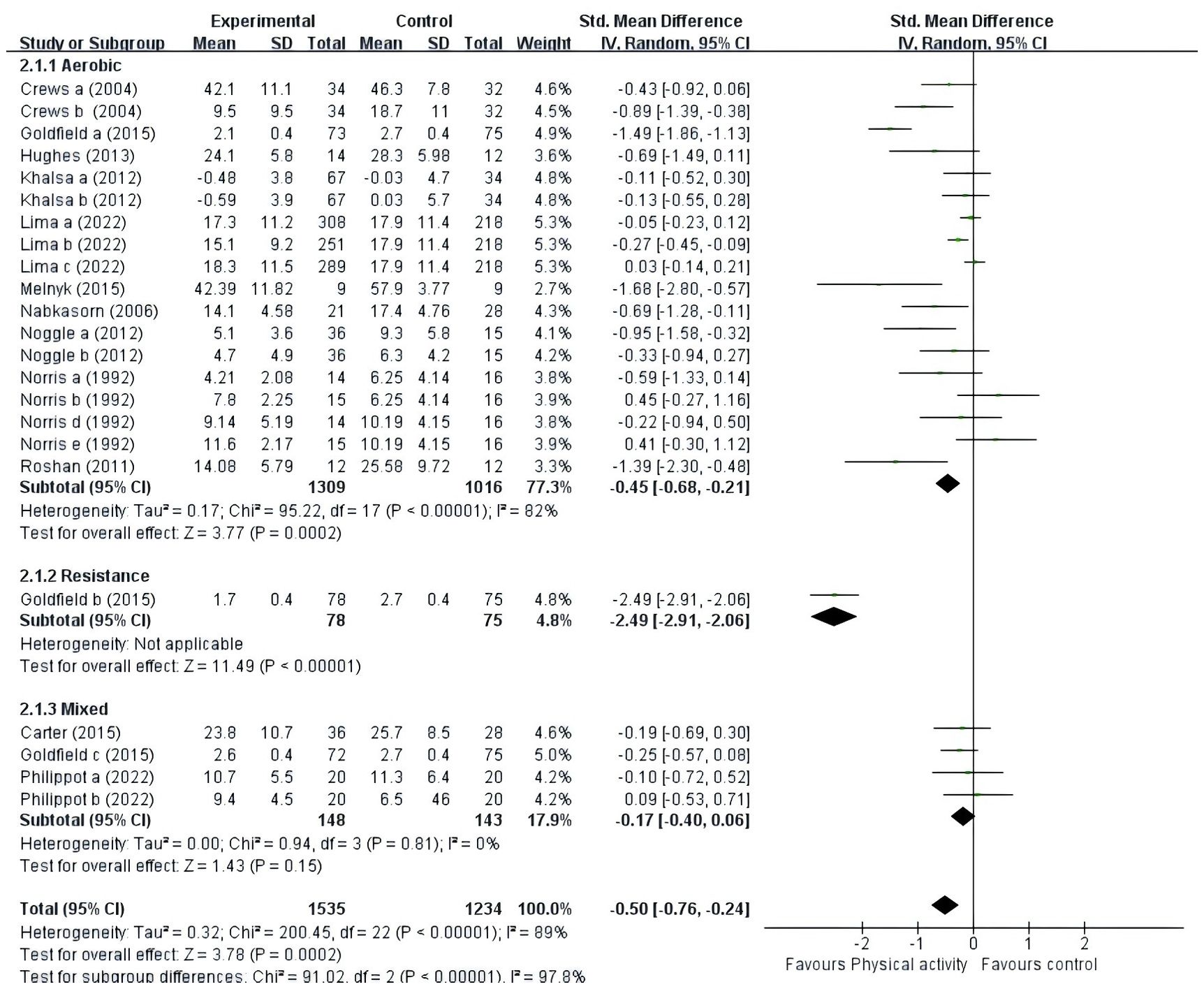
Figure 6. Forest plot of a meta-analysis of the relationship between type of PE intervention and negative emotions after the intervention.
3.6.4 PE intervention durationA total of fourteen studies were included (Figure 7). Eight studies (40, 41, 44, 47–50, 53) provided data for intervention duration of less than 12 weeks; six studies (39, 42, 43, 45, 46, 52) provided data for intervention duration of at least 12 weeks. The results showed that PE interventions of less than 12 weeks (SMD = -0.32, 95% CI = -0.54 ~ -0.10, p = 0.004, I2 = 52%) or at least 12 weeks (SMD = -0.97, 95% CI = -1.61~-0.33, p = 0.003, I2 = 98%) had a significant effect on adolescents’ negative emotions. Overall, PE interventions lasting at least 12 weeks were significantly more effective in adolescents (p = 0.003) compared to those conducted for less than 12 weeks (p = 0.004).
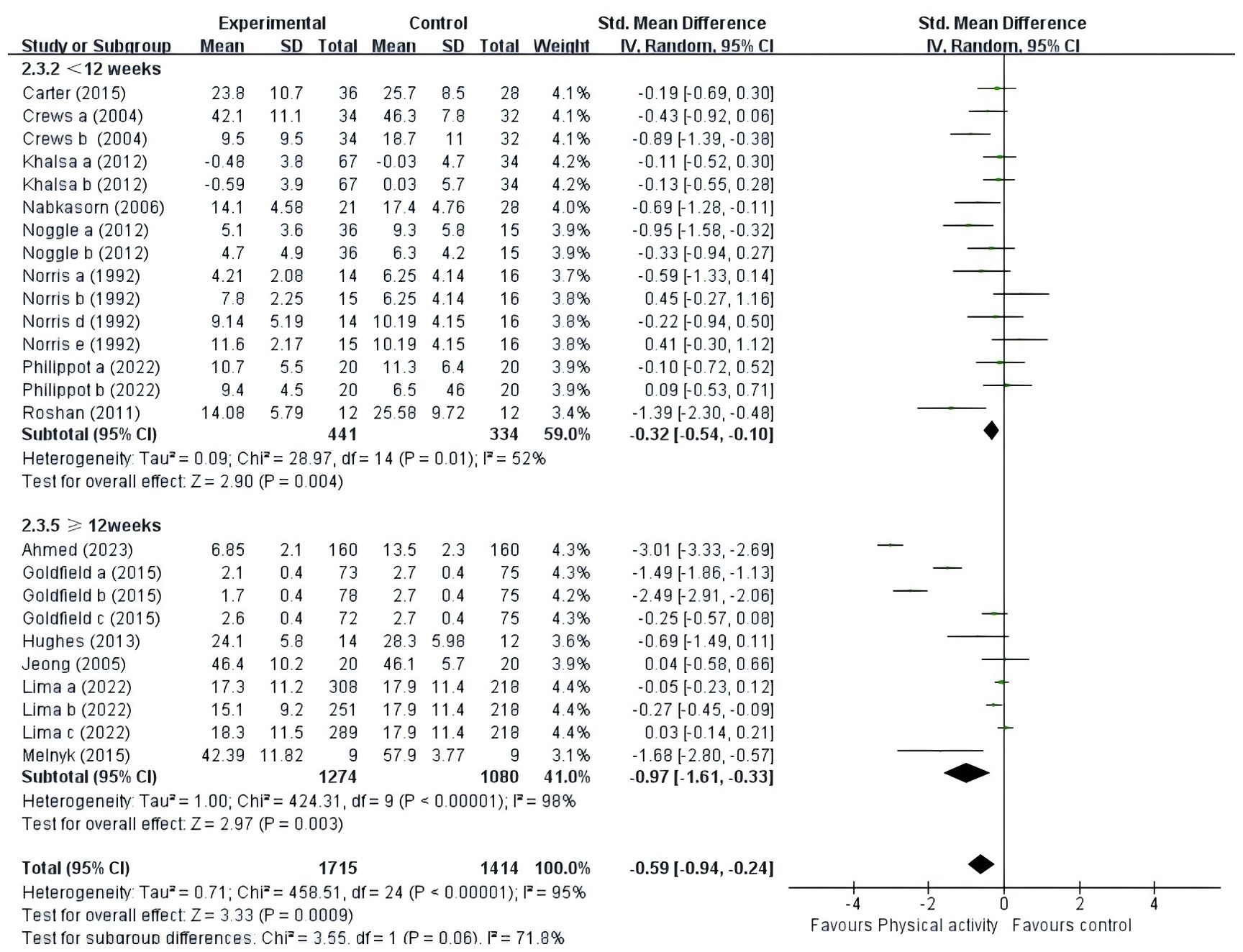
Figure 7. Forest plot of a meta-analysis of the relationship between PE intervention duration and negative emotions after the intervention.
3.6.5 PE intervention timeTwelve studies were encompassed in the analysis (Figure 8). Nine studies (41–44, 46–49, 52) provided data for intervention time less than 60 minutes; and three studies (39, 40, 45) provided data for intervention time greater than or equal to 60 minutes. The results showed that when the time was less than 60 minutes (SMD = -0.59, 95% CI = -0.98 ~ -0.20, p<0.01, I2 = 89%), the PE intervention had a significant effect on the negative emotions of adolescents. When time was at least 60 minutes (SMD = -0.70, 95% CI = -1.56 ~ 0.16, p = 0.11, I2 = 99%), PE intervention had no significant effect on adolescents’ negative emotions. Therefore, the PE of adolescents can be controlled in under 60 minutes.
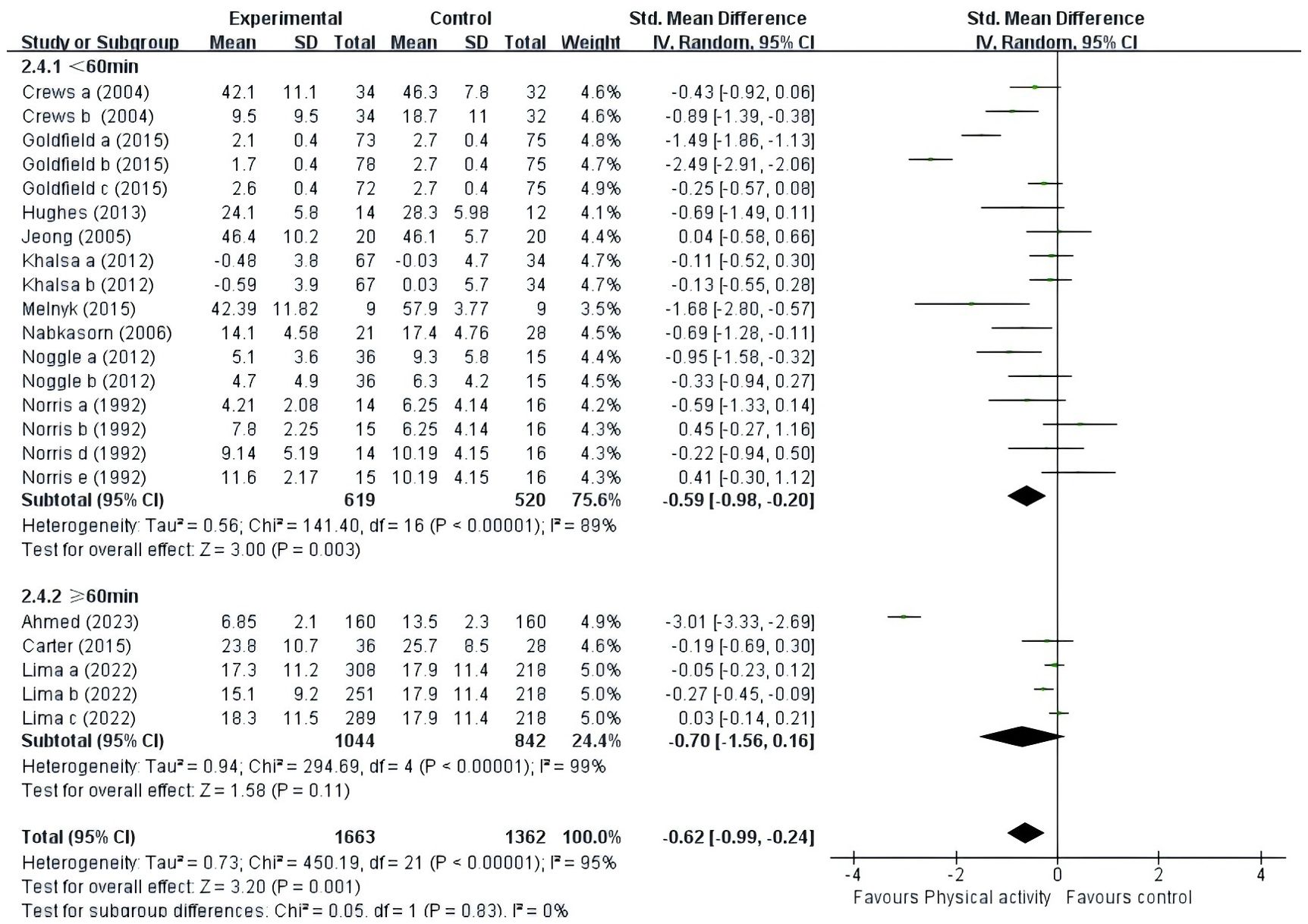
Figure 8. Forest plot of a meta-analysis of the relationship between PE intervention time and negative emotions after the intervention.
3.6.6 PE intervention frequencyA total of fifteen studies were included (Figure 9). Eleven studies (39–41, 43, 44, 46, 48, 49, 51–53) provided data at a frequency of three or fewer times per week; and four studies (42, 45, 47, 50) provided data at a frequency of more than three times per week. The results showed that adolescents were better able to improve negative affect with both PE interventions less than three times per week (SMD = -0.59, 95% CI = -1.10 ~ -0.08, P = 0.02, I2 = 94%) and PE interventions more than three times per week (SMD = -0.58, 95% CI = -1.02 ~ -0.14, P = 0.01, I2 = 95%). Overall, the PE interventions conducted with adolescents more than three times per week (p = 0.01) proved to be more efficacious than those administered fewer than three times per week (p = 0.02).
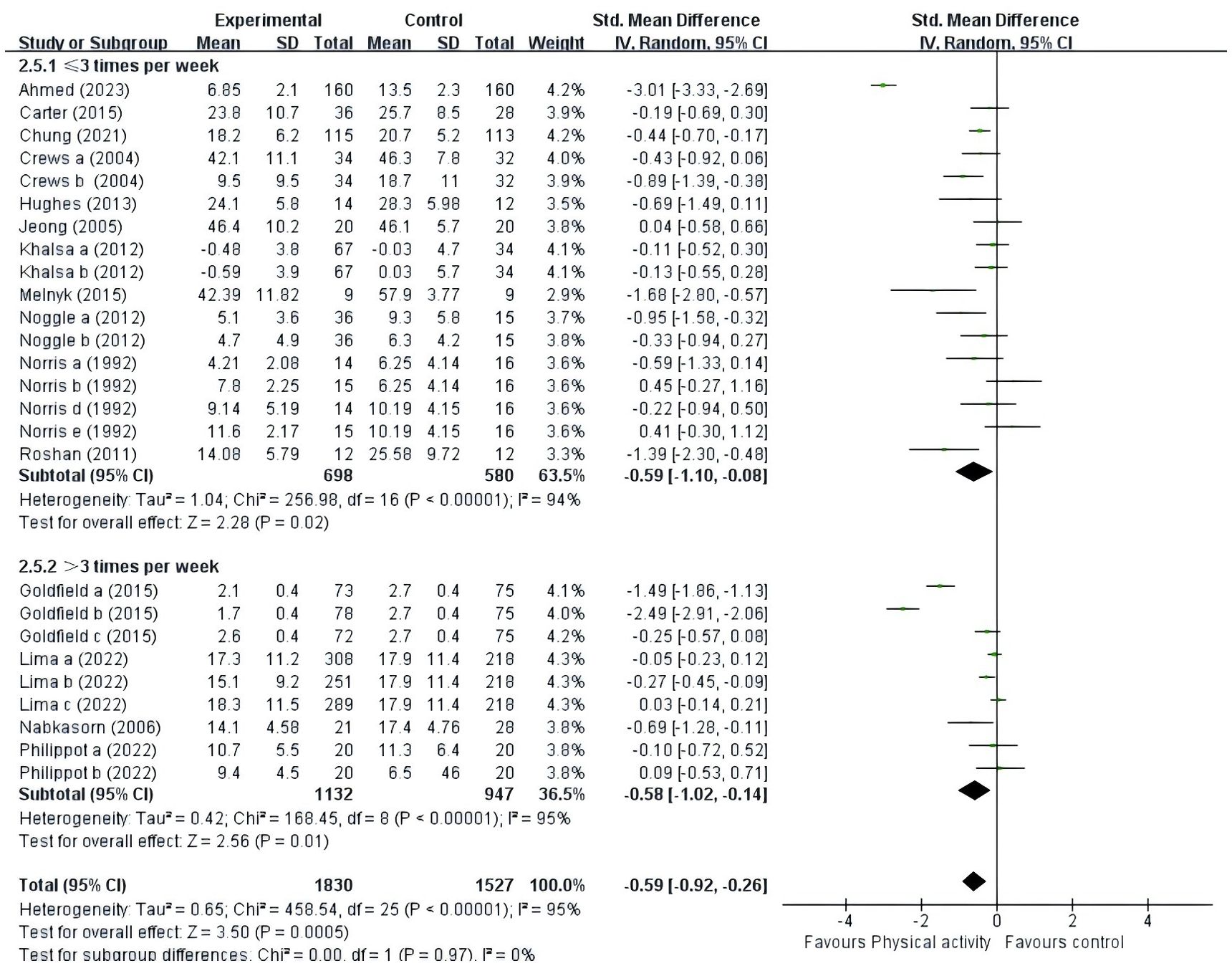
Figure 9. Forest plot of a meta-analysis of the relationship between PE intervention frequency and negative emotions after the intervention.
4 DiscussionThis study aimed to explore the impact of PE on adolescents’ experiences of negative emotions. From an initial pool of 3,368 search records, 15 studies were selected for inclusion in the meta-analysis. It was observed that since the included studies were randomized controlled trials focusing on PE interventions, the implementation of complete blinding was not feasible. Consequently, trials without blinding were not classified as low-quality during the literature quality assessment, as such a classification would be unjustified. The findings of this study indicate a significant reduction in adolescents’ negative emotions as a result of engaging in PE. The conclusions from a 2022 review by Hale and colleagues on the correlation between exercise and mental well-being corroborate this outcome. Further subgroup analyses revealed that adolescents who participated in aerobic exercise sessions lasting at least 12 weeks, conducted more than three times per week, and with each session lasting less than 60 minutes, experienced substantial improvements in negative emotions.
4.1 The effect of PE intervention on different kinds of negative emotions in adolescentsThe results of our meta-analysis indicated that participation in sports was effective in alleviating depression but not anxiety in adolescents. First, the aspect of physical activity in alleviating depressed mood in adolescents agrees with previous studies (55, 56). Participation in exercise enhances the synaptic transmission of monoamines from a physiological perspective, thereby stimulating the release of endorphins (57). These substances exert inhibitory effects on the central nervous system, effectively diminishing discomfort and elevating the brain’s active state. Consequently, this process leads to a natural improvement in mood following physical exertion (58). In a comprehensive review conducted in 2001, Sallis examined 108 studies on PE and its effects on depression in children and adolescents. The review thoroughly documented the efficacy of PE in alleviating depressive symptoms in this demographic (55). A recent clinical study, notable for its integration of psychiatric and cardiological methodologies and compelling argumentation, conducted an exhaustive examination of 210 patients diagnosed with depression. The study’s findings revealed a significant correlation between elevated depressive symptoms and decreased levels of PE among participants (56). Our meta-analysis further corroborated the effectiveness of PE in mitigating depressive symptoms among adolescents. However, our study did not confirm that physical activity was effective in reducing anxiety (p = 0.10), which is inconsistent with previous studies that have examined the ability of physical activity to reduce anxiety. A study by Tao (59) illuminates this issue, focusing on visually impaired children, revealing that continuous engagement in physical activities and the reduction of prolonged sedentary behavior not only alleviated anxiety but also significantly contributed to its reduction (59). This discovery is supported by Gehricke’s research, thus bolstering the evidence surrounding the beneficial impact of PE on reducing anxiety (60). This uncertainty was particularly evident in 7 of the 12 studies, which accounted for approximately 58.3% of the research in this area (61). From our analysis, the PE intervention did not reduce anxiety, which is more consistent with some studies. Related studies also lacked sufficient evidence that PE reduces anxiety (40, 44, 49, 50). There are several possible reasons for this situation: Critical factors encompass sample size and diversity, which significantly influence the generalizability of findings. The intervention’s intensity, duration, and consistency are paramount, as low-intensity or short-duration exercises may fail to yield meaningful changes while inconsistent adherence can further attenuate the effects. The precision, reliability, and timing of measurement tools are also essential, as inadequately selected instruments or poorly timed assessments may overlook the intervention’s true impact. Psychological elements, such as baseline anxiety levels and placebo effects, may additionally sway outcomes. Furthermore, statistical and external considerations, including the choice of control groups and environmental variables, add layers of complexity to the interpretation. Future research should incorporate larger, more heterogeneous samples and interventions that are meticulously tailored to the specific characteristics of the target population.
4.2 The effect of types of control groups on adolescents’ negative emotionsThis study investigated whether the type of control group affects the impact of physical exercise (PE) on adolescents’ negative emotions. Our meta-analysis showed that physical activity resulted in a slight reduction in negative emotions compared to the AP group (SMD = -0.23). Physical activity significantly reduced negative affect compared to the NT/WL group. The smaller improvement in the placebo group suggests that the placebo itself can provide some psychological benefit, but not as much as the actual physical activity. This highlights the importance of considering the placebo effect in psychological and physical interventions. A narrative review indicates that the mental health benefits of acute exercise may be due to placebo effects, as the acute psychological outcomes of exercise are not shown to be mediated by stimulus characteristics such as exercise duration or intensity (62). Philippot's (50) longitudinal HADS-A scores showed a reduction in anxiety symptoms over time in both groups. Thus, we can infer that participants benefited from the anxiolytic effects of the general psychiatric environment but did not derive added value from physical activity or did not have a sufficient effect size to reach significance, perhaps because of the placebo group (50). However, further research is necessary to substantiate this finding due to the observational nature of the analysis, the limited number of trials, and their low quality.
4.3 The effect of types of intervention on adolescents’ negative emotionsThe study examined whether the type of intervention affected the impact of PE on adolescents’ negative emotions. Aerobic exercise emerged as the main focus in studies utilizing PE to alleviate adolescents’ negative emotions, highlighting the widespread adoption of aerobic exercise as a preferred intervention method, consistent with previous research (54, 63, 64). Involving the voluntary movement of skeletal muscles, aerobic exercise surpasses basal metabolic rates. This form of exercise is intricately linked with various facets of well-being, encompassing physical health, mental well-being, and overall life satisfaction (63). The elevation in heart rate and oxygen consumption induced by aerobic exercise triggers the release of endorphins and various other neurotransmitters renowned for their mood-enhancing properties. In the domain of mental health and exercise physiology, the hypothesis regarding the role of endorphins enjoys substantial support. Many researchers commonly believe that endorphins play a crucial role in conserving energy during physical exertion, potentially resulting in psychological benefits such as improved mood and reduced anxiety levels (65). Direct evidence also suggests that PE has the capacity to elevate plasma endorphin levels (66). In a comprehensive review conducted in 2021, Song found that university students experienced substantial alleviation from symptoms of depression through the efficacy of both aerobic exercise and traditional Chinese exercises (64). Only one study in our meta-analysis explored the impact of resistance exercise on negative emotions in adolescents (42). This emphasizes the importance of embracing all forms of PE to optimize well-being and emotional health in this demographic. Furthermore, despite the potential for comprehensive exercise to provide a range of physical benefits, such as increased strength, flexibility, and coordination, its effect on negative emotions may not consistently demonstrate significance (40, 42, 50). These findings underscore the critical role of tailoring interventions to align with individual preferences and needs, taking into account factors such as adherence and enjoyment, which are known to influence the effectiveness of PE interventions in enhancing mental well-being and alleviating negative emotions. Additionally, the limited inclusion of only three studies may have contributed to the perception that the observed effect lacks significance.
4.4 The effect of PE intervention duration on adolescents’ negative emotionsWe assessed whether the duration of the intervention influenced the impact of PE on adolescents’ negative emotions. For this study, we categorized the included studies into two subgroups based on intervention duration: fewer than 12 weeks and at least 12 weeks. Our subgroup analysis revealed that PE interventions lasting fewer than 12 weeks or at least 12 weeks significantly affected adolescents’ negative emotions. Overall, interventions that lasted at least 12 weeks were more effective than those that lasted less than 12 weeks, which is consistent with previous studies (67–69). PE of a sustained and appropriate duration has the potential to induce significant changes in both the structure and function of the brain. These changes, in turn, have been associated with improvements in states of negative emotion. This improvement is attributed to heightened concentrations of dopamine, serotonin, and norepinephrine in the brain, known to positively influence mood regulation (30). However, long-term PE interventions may also lead to negative emotions not achieving that tan, possibly due to natural degradation processes, physical exhaustion, environmental monotony, or a combination of these factors (70, 71). Given the limited number of studies included, effect size statistics may be influenced, necessitating future large-scale studies to confirm the efficacy of PE intervention duration.
4.5 The effect of PE intervention time on adolescents’ negative emotionsIn our meta-analysis, we examined the influence of intervention duration on the correlation between PE and adolescent negative emotions. The studies included were divided into two categories based on duration: those lasting less than 60 minutes and those lasting 60 minutes or more. Our subgroup analyses indicated that PE interventions lasting less than 60 minutes significantly enhanced adolescents’ negative emotions, whereas interventions lasting 60 minutes or more did not significantly affect these emotions, consistent with previous findings (54, 72, 73). Numerous studies have indicated that individuals with depression can alleviate negative emotions by engaging in aerobic exercises lasting 20 to 40 minutes (74). A separate retrospective analysis was conducted using data from a longitudinal study spanning a decade. This analysis revealed a significant correlation between regular PE, even for durations as short as 15 minutes, and reduced susceptibility to depression (73). The findings of this study align with the prevailing recommendations outlined in both the general health promotion guidelines of the Canadian government and those of the American Academy of Pediatrics. These guidelines emphasize the importance of engaging in at least 60 minutes of moderate-to-vigorous PE daily for children and adolescents to effectively maintain their physical and mental well-being. This highlights the critical role of consistent PE in promoting overall health and underscores the importance of adhering to such guidelines for optimal health outcomes in young individuals (75). However, based on the findings of this study, prolonged engagement may potentially lead to physical exhaustion, mental fatigue, or ennui among adolescents. Consequently, this could diminish the immediate mood-elevating effects commonly associated with PE and increase the likelihood of experiencing negative emotions. Extended periods of PE can stimulate androgen production akin to that observed with anabolic steroids, potentially resulting in a significant rise in irritability and aggression (76). Introducing novelty and variety into brief workout routines has been demonstrated to heighten enjoyment and intrinsic motivation. This enhancement of positive mood and emotion is reinforced by the diverse nature of these exercises, thereby aiding in the alleviation of negative emotions and contributing to overall emotional well-being.
4.6 The effect of PE intervention frequency on adolescents’ negative emotionsThe study aimed to evaluate how intervention frequency affects the relationship between PE and negative emotions in adolescents. This meta-analysis categorized the studies into two groups based on intervention frequency: less than three times per week and three times per week or more. The subgroup analysis revealed that adolescents experienced enhanced improvement in negative affect with both less frequent (less than 3 times per week) and more frequent (3 times per week or more) PE interventions. Overall, PE interventions more than three times per week were more effective than interventions less than three times per week, which is consistent with previous research (54, 73, 77). Current clinical recommendations propose that to alleviate negative emotions in children, engaging in exercise sessions lasting at least 45 minutes on a minimum of three days per week is advisable. These guidelines highlight the importance of exercise frequency in alleviating negative emotions among children (77). Adolescents should engage in PE sessions at least three times weekly, as recommended by current clinical guidelines. This structured regimen facilitates the establishment of consistent exercise habits among adolescents. Regular participation in PE over time promotes positive physical and mental adaptations, contributing significantly to overall well-being and long-term adherence to exercise routines. Integrating PE into their weekly schedule can lead to sustained improvements in mood and emotional well-being. Moreover, maintaining a high frequency of PE sessions helps sustain the mood-enhancing benefits of exercise throughout the week. By spacing out their PE sessions and consistently exposing themselves to the positive physical effects of PE, adolescents can experience more enduring improvements in mood, fostering emotional stability and long-term well-being. Therefore, increasing the frequency of PE sessions to three or more times weekly represents a potentially effective strategy to enhance mental health and emotional well-being in adolescents. Further research should explore optimizing PE interventions tailored to the specific needs and preferences of adolescents.
4.7 Proposed clinical interventions based on meta-analysis findingsTo translate the findings of the meta-analysis into effective clinical practices for mitigating negative emotions in adolescents, several intervention strategies can be proposed, each meticulously tailored to address the unique needs of this population. Among the most impactful approaches is the introduction of structured physical activity programs, which could be implemented in schools or community centers specifically targeting adolescents who grapple with negative emotions. Ideally, these programs should be conducted three to five times per week, with sessions lasting between 30 and 60 minutes at a moderate to vigorous intensity, contingent upon the individual’s fitness level and psychological state. The potential benefits of such programs are considerable, including the alleviation of symptoms associated with depression, anxiety, and stress, as well as enhancements in overall mood through the release of endorphins and the promotion of neuroplasticity. Moreover, group activities within these programs can provide essential social support, which is particularly advantageous for adolescents navigating negative emotions. However, challenges such as maintaining consistent participation, ensuring accessibility to facilities, and the necessity of individualized programming to accommodate varying fitness levels and emotional states must be carefully managed to optimize the success of these interventions.
Incorporating physical activity into existing therapeutic practices, such as cognitive-behavioral therapy (CBT), represents another promising intervention. This approach could involve the integration of brief exercise breaks—five to ten minutes of aerobic exercises—within therapy sessions or prescribing personalized exercise routines as part of therapy homework. The inclusion of physical activity in this context may enhance the overall efficacy of psychological treatments, empowering adolescents by equipping them with coping skills through movement. Nevertheless, this approach does pose challenges, including the need for additional training for therapists to integrate exercise effectively, as well as potential resistance from adolescents who may have low motivation or negative associations with physical activity.
Lastly, the development of school-based wellness programs that amalgamate physical education, mental health education, and mindfulness practices presents a holistic approach to addressing negative emotions in adolescents. These programs should incorporate curricula that educate students on the psychological benefits of exercise and stress management techniques, alongside peer support groups that encourage participation in physical activities and offer emotional support. The key advantages of this approach include the promotion of both physical and mental well-being and the cultivation of a culture that recognizes the interconnectedness of emotional health and physical activity. Nevertheless, the successful implementation of such programs necessitates coordination among educators, school counselors, and physical education instructors, and they must be designed to be sustainable and adaptable to the evolving needs of students.
In conclusion, the application of these meta-analysis findings offers a promising avenue for supporting adolescents with negative emotions through physical activity-based interventions. Whether through structured programs, integration into therapy, or comprehensive school-based initiatives, these strategies can be tail
留言 (0)