
記住我
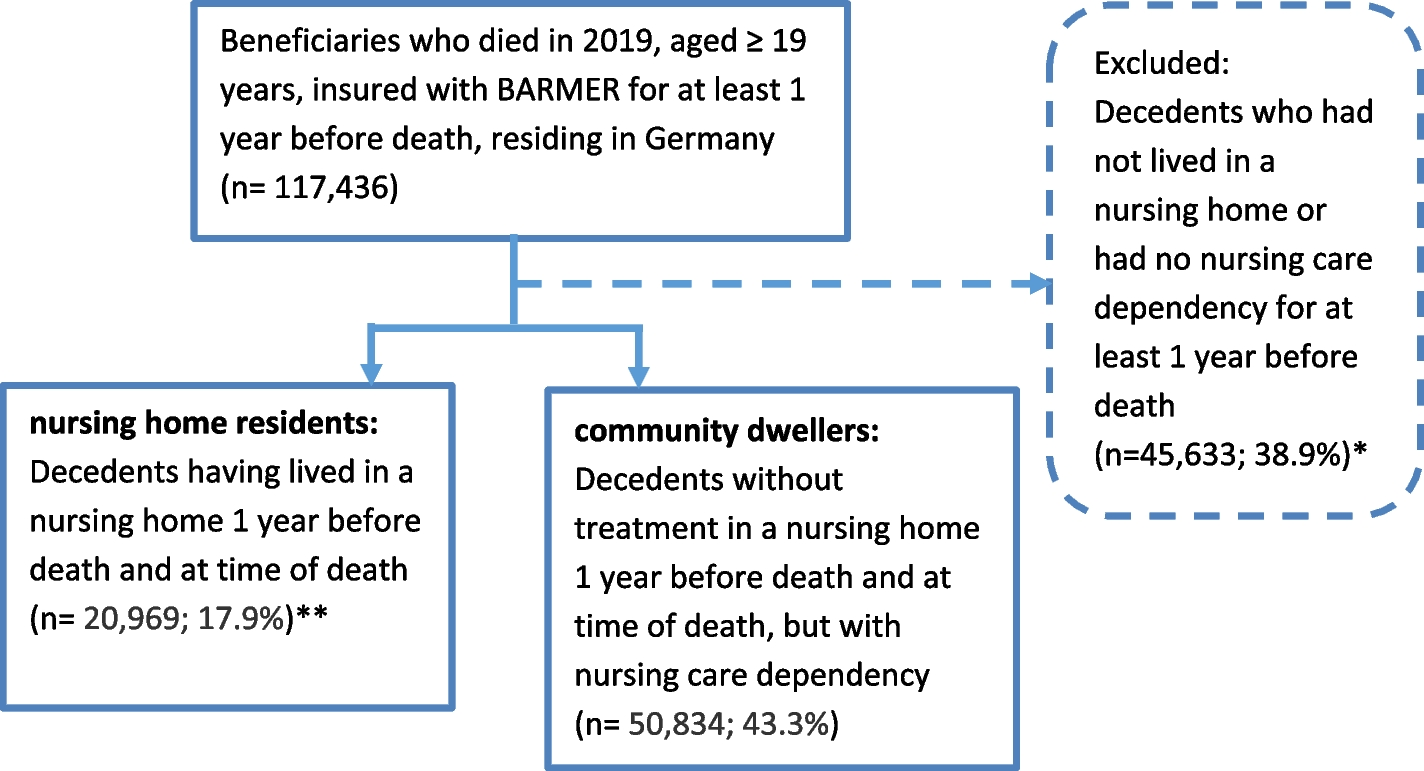




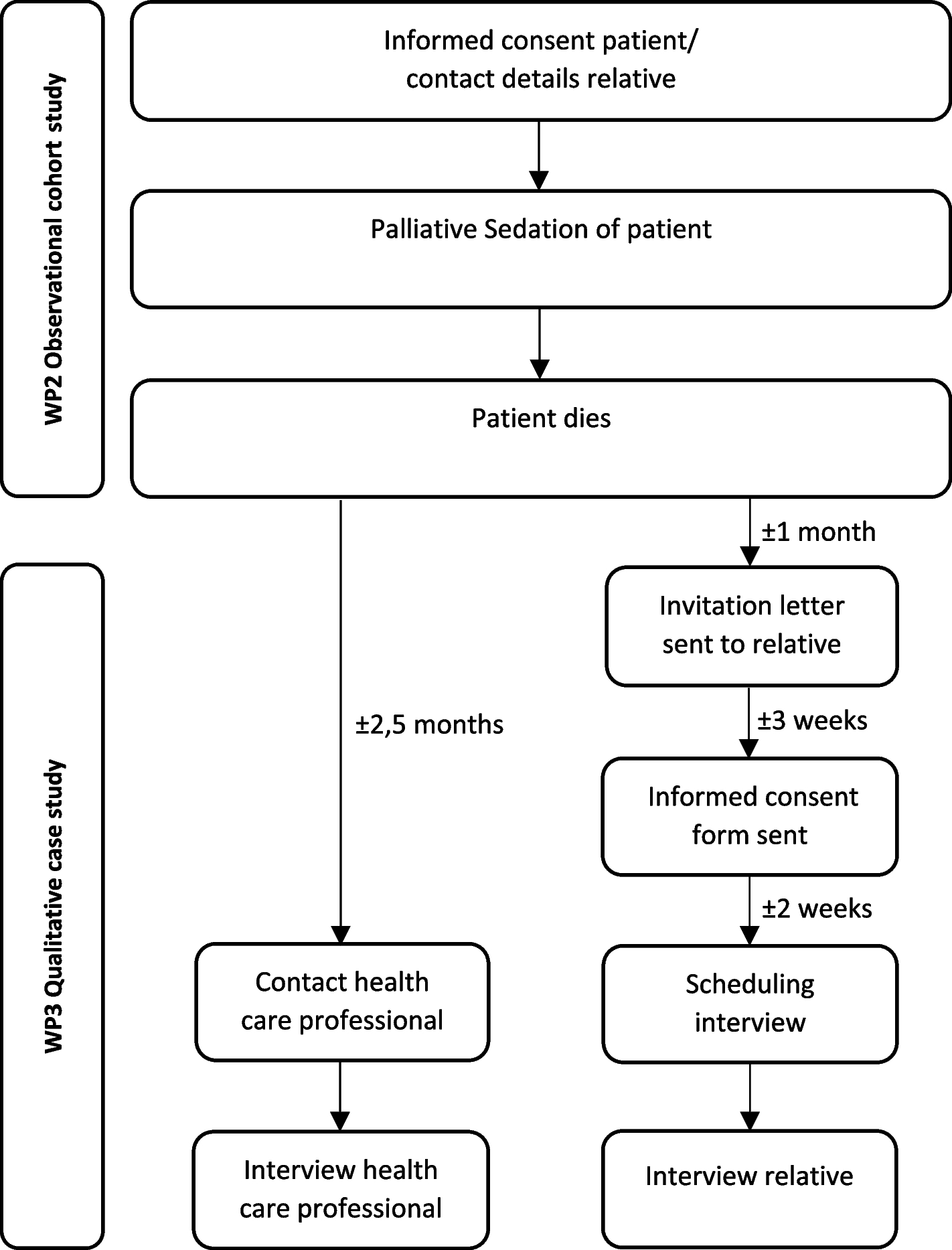
During the interview period (5 months), from the two units monitored for selection bias a total of 60 palliative patients were admitted, of which 33 patients met the inclusion criteria. From these 33 potential participants, 15 patients were not interested to participate, two patients had no time, and two patients indicated concerns with data protection (Fig. 1). The 15 participants, 8 men and 7 women, ranged in age between 39 and 82 years (M = 63.4; SD = 11.3). The majority was married (n = 8) or single (n = 7), two were widowed, one did not provide information. Six patients had children. The majority were diagnosed with multiple myeloma (n = 5), n = 3 patients had a pancreatic carcinoma while the following diagnoses occurred once: gastric cancer, cholangiocellular carcinoma, colorectal carcinoma, breast cancer, ovarian cancer, and lymphoma. On average, patients had been in the hospital for 8.9 days (SD = 10.7). We did not collect the socio-demographic details of the relatives.
Fig. 1
Flowchart of included study participants
We identified a total of 235 codes and classified them into 6 main categories with subcategories: General interest in VR, desired content, content not desired, expected benefits, concerns, irregularities (see Table 1). Of the 235 codes, 42 were assigned to two different subcategories.
Table 1 Category system with main and subcategoriesGeneral interest in VRMost patients and relatives expressed a general interest in VR for cancer patients in the palliative setting. For example, one relative said: “And I would definitely be in favor of something like that. Absolutely” (rel04f). Some patients reported a clear lack of interest: “Because I’m not interested in it, I don’t deal with it at all” (pat12f). One patient remained undecided: “I can’t imagine at the moment because I always prefer the original. But maybe in old age or, never say never, with advanced illness, but I’ve already mentioned it, I’m actually gifted with a great imagination” (pat13m). Patients and relatives named content that they would like to see for VR applications in the palliative setting.
Desired VR contentMost patients and half of the relatives named nature as desirable content for the VR videos. Very different aspects were mentioned, including general videos with “everything to do with mountains” (rel04f); walks in the forest or “by the sea, on the beach” (pat01m). But there were also specific places mentioned such as “my meadow” (pat09m). Cities and sights were also frequently named by patients and relatives. Here, too, specific places such as “Jerusalem” (rel03m) were mentioned as well as general ideas: “…or simply pretty, great cities, pretty buildings…” (pat09m). Some patients and one relative actively named their own home and family as videos that they would like to see, e.g. “… therefore our home. We built the house ourselves” (rel01m). For some patients, the content was less important, but they were interested in a virtual escape from the hospital. Time travel to the future or the past was also of interest. One patient would be interested in playing games on VR headsets.
Weighing of interestNature (M = 7.53) and cities and sights (M = 8.18) were endorsed most strongly; the own home (e.g. living room, garden; M = 5.00) and images of people close to them (e.g. friends, family; M = 7.00) were moderately preferred with substantial differences between people (Table 2, column range).
Table 2 Scaled retrieval of desired video contentNon-desired VR contentIn addition to the desired videos, the study participants named content that they would not want to see on VR headsets. Some negative images such as terror, war, torture, and disputes were named. However, boring content were also highlighted; one patient was concerned that “some games are so optimized for the disease or for tests running in the background that they are simply boring” (pat09m). Nevertheless, for patients and relatives, the idea of seeing a personalized VR video was clearly associated with benefits.
Expected benefitsAround half of the interviewees anticipated well-being such as “joy” (pat04f), “good well-being, positive experiences” (rel03m), and fun. They expected that the videos would evoke fond memories. One relative said: “… when you can visually go back to these places that you actually love. […] and you also know what you experienced there, out in the garden. It brings back a lot of memories…” (rel01m). The interviewees also expected a break from the patient experience. Some saw an advantage in being able to pursue their own curiosity. A few patients and one relative had little idea of the positive effects a VR video could have in a palliative context and were uncertain. One patient said: “That’s a difficult question. If I don’t try it now, I can’t do it now, so I can’t give you an answer to that. I’m sorry” (pat07m). Next to the expected benefits, we were interested in concerns.
ConcernsWhen asked about concerns, most patients and relatives spontaneously replied that they had no concerns. The interviewer raised possible concerns, some of which were then shared by the interviewees. Privacy and security were frequently discussed in the context of videos of the patient’s own home. Some patients and one relative did not perceive it as a problem at all. However, the majority of the participants mentioned conditions that would have to be met; usually who would be allowed to record the videos and who would be allowed to see them, e.g. “…as long as they [note: individualized videos] are only accessible to these specific people, that wouldn’t be a problem for me at all.” (rel04f) or “So I would only want my son to do that [note: video recording of my own home]” (rel04f). Most patients also considered the fact that relatives would be filmed to be unproblematic. However, some interviewees considered personalized VR videos of their own home and/or relatives unimaginable due to privacy concerns.
Most patients and relatives had no concerns specifically about the implementation of personalized videos to patients in the palliative setting. If they mentioned concerns, they mostly asked for support, e.g. “…if you are no longer quite up to scratch motorically… you have to make sure that you put it on well, that it hasn’t slipped somehow, otherwise you see everything askew and that’s not good either. Or if you don’t put it on properly, you can still see something from normal reality. It has to be put on properly, the straps have to be tightened; you might need a bit of help” (rel03m). Some patients mentioned concern about not getting any added benefits from an individualized VR video. One patient said: “I just thought to myself, yes, it’s virtual, but not real. And that can make her happy at the moment, but when she’s out of the thing again, just shitty again, right?” (pat14f). Others were concerned that individualized videos would reinforce negative feelings or memories, including homesickness. One patient said: “…in places that you have a close connection to. […] I can’t really tell, but I think it’s quite possible that it triggers sadness. That it’s a pain, a shock, an internal shock, along the lines of: ‘Look there. You’ll never be able to do it again.’ […] or look at the tree you planted on your x-th birthday and how big it is. But you won’t live to see it stand for 25 years because you have a lethal tumor. Although it doesn’t necessarily have to be deadly or won’t be deadly with treatment. But I’m afraid those negative thoughts will come” (pat09m).
Some patients were concerned about being influenced through the use of VR, e.g. that VR videos “lead to an impairment of the own fantasy world” (pat14f) or that they “actually lose my sense of reality” (pat14f) as a result. One patient mentioned the fear of being manipulated by VR videos and drew a reference to marketing strategies.
Time perspectivePatients agreed moderately (M = 4.83) with the statement that they still have time to make plans. They also agreed moderately (M = 5.40) that their time is running out. The answers to both statements showed substantial differences between the patients (see Table 3, column range).
Table 3 Time perspective of patientsIrregularitiesIn 10 answers (by 6 patients), we think that the interviewee had not understood the question correctly, as the answer was unsuitable to the question, which might be due to the vulnerable health of the patients. Further, we observed in seven statements that the participants contradicted themselves or changed their mind during the interview, which might occur in any reflective context. It was also noticeable that thoughts about others were stated, such as “There are certainly people and situations for whom that would be nice. But as I said, I prefer to look at it globally somehow” (pat14f). Or “Oh well, not for me personally, I don’t have a garden, but I think it would be really interesting for older people” (pat05m) that could be attributed to double awareness in order to cope with being under palliative care, facing a life limiting prognosis.
留言 (0)