The parallel group randomised controlled trial was conducted in Hong Kong, China. Ethical approval was obtained from the Institutional Review Board (IRB) of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (UW 18–053). The trial was registered in ClinicalTrials.gov (NCT04163354).
Sample size calculation
The sample size was calculated based on the outcome of child anxiety, cooperativeness and pain assessed using Frankl Behaviour Rating Scale (Frankl 1962) (FBRS), Venham Behaviour Rating Scale (Venham et al. 1980) (VBRS) and Wong–Baker Faces Scale (Wong and Baker 2001) (WBFS). Based on Yon et al. (2020a, b), the proportion of pre-school children having negative dental behaviours is 4.4%. Assuming that quarterly application of NaFV can completely alleviate DA of pre-school children whilst the GIS group could not achieve the same outcome, the sample size was 180 per group when targeting a significance level of 0.05 and statistical power of 0.9; i.e. a total of 360 children at baseline. The initial sample size is further enlarged by 10% as children was further excluded if GIS cannot be placed on their occlusal surfaces. Hence, a total of 396 children were required, with 195 children being allocated to each group.
The children underwent additional follow-up to evaluate the development of occlusal caries in their primary molars over a period of 18–24 months. When the sample size was calculated based on progression of occlusal dentinal caries, it was determined that 284 children were required at baseline. The methodology for calculating the sample size is detailed elsewhere (Lam 2023). Considering both calculations, a total of at least 396 children were needed for this study.
Subject selection
Children aged between 3 and 6 years attending kindergarten grade 1 and nursery grade 2 in Hong Kong were invited to participate in the clinical trial. The study was conducted in 18 preschools located in various districts in Hong Kong using a combination of stratified and purposive sampling methods [Hong Kong Island (n = 4), Kowloon (n = 5), New Territories West (n = 5), New Territories East (n = 4)]. Parents or legal guardians received an invitation letter explaining the objectives and the procedures of the study. Only those children whose parents or legal guardians had signed the informed consent were included. In addition, parents were asked to complete a questionnaire regarding their socio-economic background and oral health-related behaviours.
Inclusion criteria
The potential subjects were screened using the following methods: plaque assessment using Visible Plaque index (VPI) (Ainamo and Bay 1975), overall tooth status assessment with diagnostic criteria recommended by WHO 2013(WHO 2013) and dental caries status cased on ICDAS code score (Ismail et al. 2007). After screening, children considered to be moderate to high caries risk according to the criteria (“Guideline on Caries-risk Assessment and Management for Infants, Children, and Adolescents,” 2016) outlined by the American Academy of Paediatric Dentistry (AAPD) were included. The criteria were children who were recent immigrants or of lower socio-economic background, who snacked more than 3 times a day, children with visible plaque, or who were put to sleep with a bottle containing natural or added sugar and children having decayed-missing-filled surfaces score of more than 1, having visible plaque or enamel defects. According to the AAPD guidelines, children with either moderate or high caries risk are recommended to receive fissure sealants and topical fluoride varnish application regularly every 3 months (“Guideline on Caries-risk Assessment and Management for Infants, Children, and Adolescents,” 2016).
Exclusion criteria
Children with serious systemic diseases requiring long-term medication or special needs were excluded. Furthermore, children who were uncooperative during the procedure or had received professional topical fluoride treatment in the past 6 months were excluded. Furthermore, primary second molars that are partially erupted, with enamel defects or with sealants, restorations or dentinal caries indicated by ICDAS scores 4, 5, and 6 was excluded.
Subject recruitment
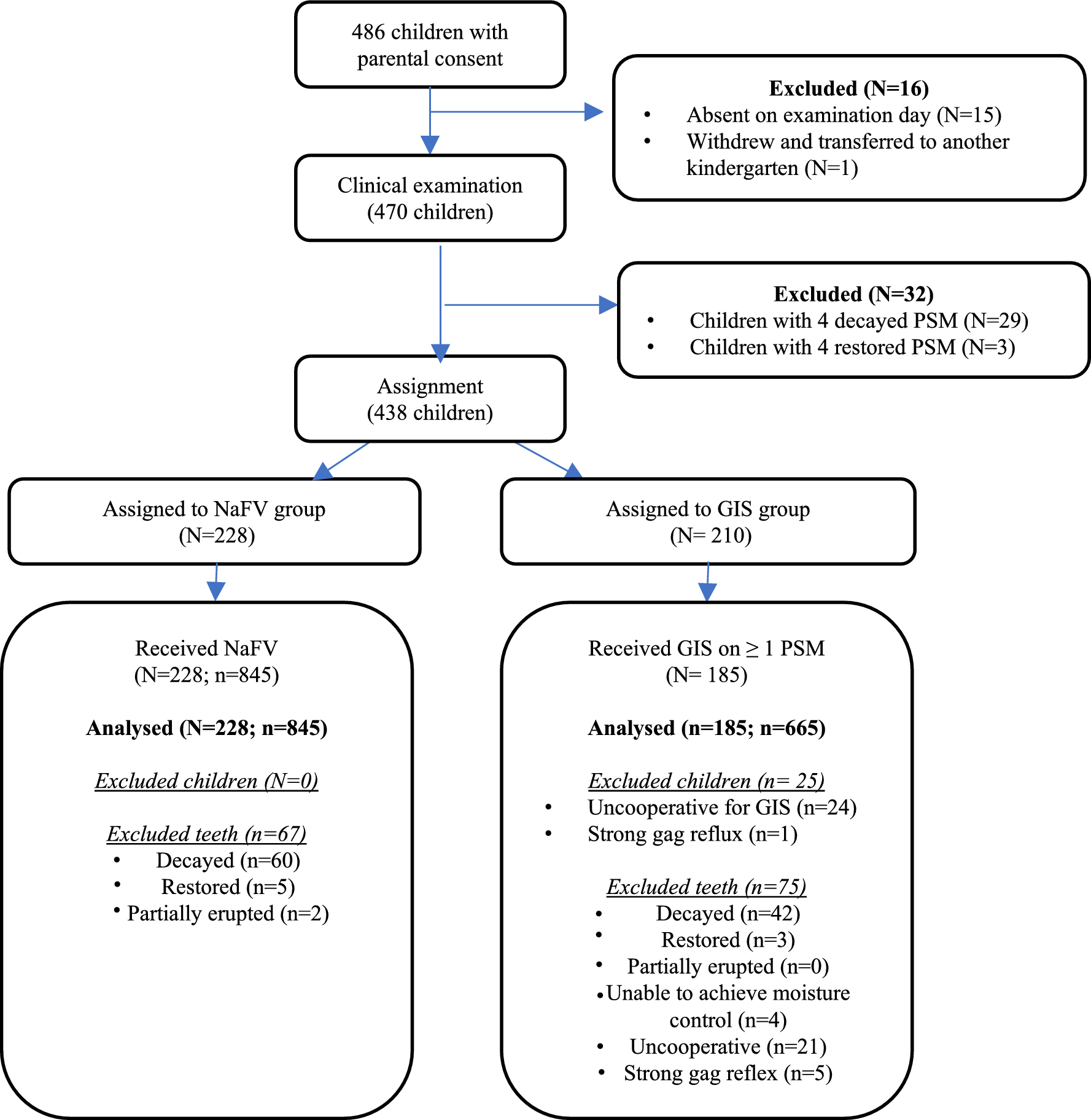
Subject recruitment lasted from September to December 2019. Children attending kindergarten grade 1–2 in 16 study kindergartens were approached. A total of 486 parental consents and completed questionnaires were obtained. Out of the 486 children, only 413 were deemed eligible and randomly assigned into the two treatment groups.
Questionnaire
Parents were required to complete a validated questionnaire before the baseline examination and intervention. The questionnaire included the child’s personal information, such as gender, age, place of birth and medical history; oral health-related behaviours, such as snacking habit, frequency and parental supervision of toothbrushing, use of toothpaste and night-time bottle habit; the child’s socio-economic background, such as parental age, education level household income and the number of siblings.
Clinical examination
Clinical examination was performed by one operator (P.P.Y.L.) with the child lying supine on a table provided by the kindergarten. The operator received training and had been examining children with VPI, dmft and ICDAS examination in an outreach setting for over 4 years. Disposable dental mirrors fastened to an intra-oral light emitting diode (MirrorLite, Kudos Crown Ltd., Hong Kong) along with a WHO CPI probe were used to record the VPI score and decayed, missing, filled, surfaces (dmfs) and teeth (dmft) scores. After cleaning and drying the teeth with gauze, the carious status of the primary second molars was noted using the ICDAS coding system. As air-drying with 3 in 1 syringe was not possible in an outreaching setting, ICDAS 0 and 1 lesions were grouped together for record to enhance detection reliability. The ball end of the CPI probe was used for tactile sense to detect enamel cavities or defects amongst the pits and fissures. A 10% random sample was re-examined to monitor intra-examiner reproducibility. The kappa values for intra-examiner reliability were 0.774, 0.964 and 0.834 for VPI, dmft and ICDAS examination, respectively (Lam et al. 2021).
Randomisation and treatment allocation
Treatment allocation was conducted by using random numbers generated by stratified block randomisation method in a personal computer, and the children were randomly allocated to one of the two intervention groups. The random allocation was concealed and only revealed in front of the participants just before their respective allocation.
Interventions
Immediately after oral examination, a chair-side dental assistant prepared the materials respective to the groups allocated on the random allocation list. Both interventions were provided by one operator (P.P.Y.L.). For the sealant group, GIS was applied using the finger pressure technique outlined in the WHO manual for atraumatic restorative treatment. The primary second molars were first cleaned and dried with gauze and afterwards, GC cavity conditioner (10% polyacrylic acid) was applied with micro-brush for 10–15 s and subsequently cleaned with wet cotton pellets. The assistant then mixed a capsule of standardised liquid–powder ratio GIC (GC Fuji VII, GC Asia) with the amalgamator and the operator applied the material on the occlusal surface using a plastic instrument. A gloved finger with petroleum jelly (Vaseline) was used to rub the GIC into the pits and fissures. Subsequently, excess material was removed using a hand excavator. The operator followed a standard technique and a protocol for each subject.
For the NaFV group, the operator placed 0.25 ml of varnish (Colgate Duraphat varnish, Colgate-Palmolive UK Ltd) in the plastic dappen dish. A micro-brush was used to apply the varnish onto the second primary molars and rest of the dentition. The child was instructed not to eat or drink for at least half an hour after the application.
Assessment of dental anxiety, cooperativeness and pain
The following four parameters were assessed at baseline and post-intervention including Frankl Behaviour Rating Scale (FBRS) (Frankl 1962) and Venham Behaviour Rating Scale (VBRS) (Venham et al. 1980) for DA and cooperativeness assessment; Wong–Baker Faces Scale (WBFS) (Wong and Baker 2001) for pain assessment and the length of time for intervention. Frankl Behaviour Rating Scale is a 4-point behavioural scale which ranges 1 (definitely negative) to 4 (definitely positive). Venham Behaviour Rating Scale is a 6-point behavioural scale ranging from 0 (total cooperation) to 5 (general protest). Besides assessing children’s behaviour and reactions, these two scales may provide an insight to the patient’s inner emotions and anxiety, which are reflected by their actions. Wong–Baker Faces Scale has long been utilised in previous studies to assess pain and discomfort in the paediatric population (Garra et al. 2013). It consists of 6 sequential faces, the number 0 happy face meaning “no pain at all” whilst the number 10 crying face meaning “most intense pain imaginable”.
One assessor (H.H.C.C.) was responsible to examine the following parameters during the study period. Before any treatment or intervention, the child was first be introduced to the WBFS. This is to ensure that the children are familiar with the spectrum of faces and their corresponding meanings. Once the child is familiar with the scale, they were asked to identify a face which denotes their current state of comfort before commencement of the treatment. Afterwards, the assessor recorded the score for both FBRS and VBRS on the examination sheet before the start of treatment.
After clinical examination and random allocation of treatment group, a plastic disposable tray of dental instruments and materials were placed next to the operator by the assistant. Subsequently, a timer was started to determine the duration of the intervention. The assessor observed the child throughout the entire process and determined the score for FBRS and VBRS to signify the child’s level of DA and cooperativeness during the procedure. After the intervention was completed, the timer was stopped, and the child was asked to choose a WBFS face to denote their current sentiment after the intervention.
Outcome measures
The primary outcome measure is the change in children’s DA and cooperativeness (FBRS and VBRS) as well as pain (WBFS) rating from the start to the end of the intervention. Secondary outcome measure is the duration of the two interventions.
Data processing and analysis
Data analysis was be performed using SPSS® Statistics version 23.0 (SPSS Inc, Chicago, IL, USA). Data proofreading was performed after data entry to identify and correct any anomalies before analysis. Chi-square test was used to assess the difference between the two groups according to the distribution of children’s demographic characteristics, such as gender, place of birth, oral health-related behaviour, use of fluoride toothpaste, snacking habit, parent’s education and family income. A multi-level logistic regression analysis was performed to analyse the effects of independent variables on the DA level of children, measured with FBRS, VBRS and WBFS. The variables include the child’s socio-demographic characteristics, oral health-related behaviours, clinical characteristics (VPI score, dmft score) and the treatment groups. The level of statistical significance for all tests was set at 5%.








留言 (0)