
記住我










The global burden of cancer is increasing rapidly, mainly due to the ongoing demographical and epidemiological transition1. Cancer is the leading cause of death globally (about 1 in 6 deaths), with an estimated 10 million deaths in 20202,3. Population ageing has significantly contributed to the rising burden; earlier estimates showed that older ages account for about 50 per cent of all global cancer burden4. Despite the high incidence and mortality, limited information is available regarding the disease burden in this group. Older patients are always at an elevated risk of unfavourable outcomes due to coexisting co-morbidities, and a higher treatment abandonment rate5,6 and lower survival rates were seen in older adults as compared to younger ones7.
It is projected that one in every six persons globally will be aged 60 yr or over by 20308, which will lead to an increase in both cancer incidence and deaths. This growing burden will make the role of geriatric oncology immense in the coming years to ensure comprehensive and effective treatment and care for this group of patients, particularly when resources are limited. We need good stratified local or national data on elderly cancers, which will also help to formulate effective local cancer control policies.
This study was initiated to provide a detailed global pattern of elderly cancer mortality by world region, sites and gender, which would help develop local elderly cancer care policies.
Material & MethodsThe study was undertaken at ICMR-Centre for Ageing & Mental Health, Kolkata, India from March to July 2023, after obtaining the approval from RIO (Research Integrity Officer).
Cancer mortality (deaths) and future estimates were arrived at using publicly available Globocan 2020 online database [Global Cancer Observatory (gco.iarc.fr), cancer today, cancer tomorrow and cancer over time] of the International Agency for Research on Cancer (IARC), World Health Organization (WHO) for all cancers combined (ICD-10, C00-C97, except C44), available for 185 countries or territories for 36 cancer types by sex and age group9-11. Data were available for 185 countries or territories. During the continent-wise analyses, data were extracted and reported for Asia, Europe, Northern America, Latin America & the Caribbean, Africa and Oceania.
We reported the number of new deaths among elderly aged 60 yr and above, truncated age-standardized mortality rates (per 100,000) for all cancer sites combined, site-wise, gender-wise and world region-wise. The truncated ASR was calculated for the age group 60 and above using the world standard population method proposed by Segi and modified by Doll et al12. Estimated results and figures generated online were used with appropriate permission from IARC Section of Cancer Surveillance (CSU).
All the analyses were done using Microsoft Excel, SPSS version 21 (IBM, Armonk, NY, USA) and IARC-WHO online portal (gco.iarc.fr, cancer today, cancer tomorrow and cancer over time).
Data permissionNecessary permission was obtained from the IARC–WHO for data abstraction, analysis and generating tables and Figures along with proper citation were provided as per the laid out policy ( https://publications.iarc.fr/Terms-Of-Use).
ResultsIt is estimated that 71.2 per cent (70,46,181 deaths excluding non-melanoma of skin) of all cancer-related deaths occur in individuals aged 60 yr and above in 2020, with a higher relative proportion of deaths in Asia (55.7%), followed by Europe (23%), Northern America (8.3%), Africa (5%) and Oceania (0.8%) (Table I, Fig. 1A). A total of 1.42 million deaths were estimated due to lung cancer in both sexes accounting for 20.2 per cent of all cancer deaths among older adults (Fig. 1B). It is quite remarkable to come across such findings among all global elderly deaths due to cancer; China alone accounts for 30.5 per cent when both sexes considered together, among elderly male deaths it accounts for 32.6 per cent and among elderly female deaths, it accounts for 27.7 per cent of total elderly global deaths (Table I).
Table I. Mortality (deaths, relative %, age-standardized rate) for all cancers (excluding non-melanoma of skin) by sex, continents, human development index and income in 2020
Population Males Females Both sexes No. of deaths Relative % ASR (World) No. of deaths Relative % ASR (World) No. of deaths Relative % ASR (World) Asia 2298840 57.6 782.4 1628433 53.3 473.4 3927273 55.7 616.1 Europe 899659 22.5 956.6 723847 23.7 525.1 1623506 23 706.6 Northern America 310078 7.8 686.2 273984 9 488.2 584062 8.3 576.7 Latin-America and the Caribbean 271917 6.8 653.3 234261 7.7 440.5 506178 7.2 531.7 Africa 178083 4.5 552.6 171338 5.6 426 349421 5 479 Oceania 31418 0.8 733.2 24323 0.8 491.3 55741 0.8 602.5 World 3989995 100 781.5 3056186 100 481 7046181 100 615.1 High HDI 1848109 46.3 912.5 1294606 42.4 531.2 3142715 44.6 704.2 Very high HDI 1619996 40.6 856.4 1289203 42.2 496.1 2909199 41.3 652.4 Medium HDI 424313 10.6 415.1 369708 12.1 328.5 794021 11.3 369.5 Low HDI 95606 2.4 469.2 101197 3.3 402.6 196803 2.8 429.9 China 1300675 32.6 1064.7 847591 27.7 604.4 2148266 30.5 819.4 India 242557 6.1 354.2 213988 7 297.2 456545 6.5 325 Upper middle income 1971237 49.4 941.3 1389738 45.5 533.7 3360975 47.7 716.1 High income 1376719 34.5 819.2 1095713 35.9 496.5 2472432 35.1 639.1 LMIC 573402 14.4 455.1 496340 16.2 346 1069742 15.2 396.4 Low income 66666 1.7 490.7 72923 2.4 412.5 139589 2 443.3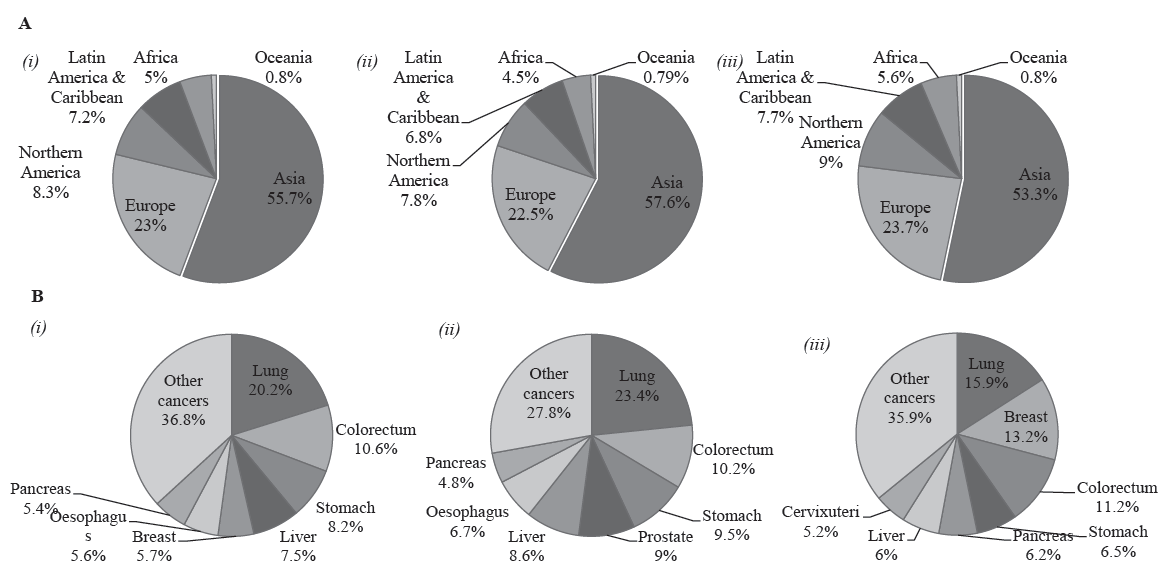
Export to PPT
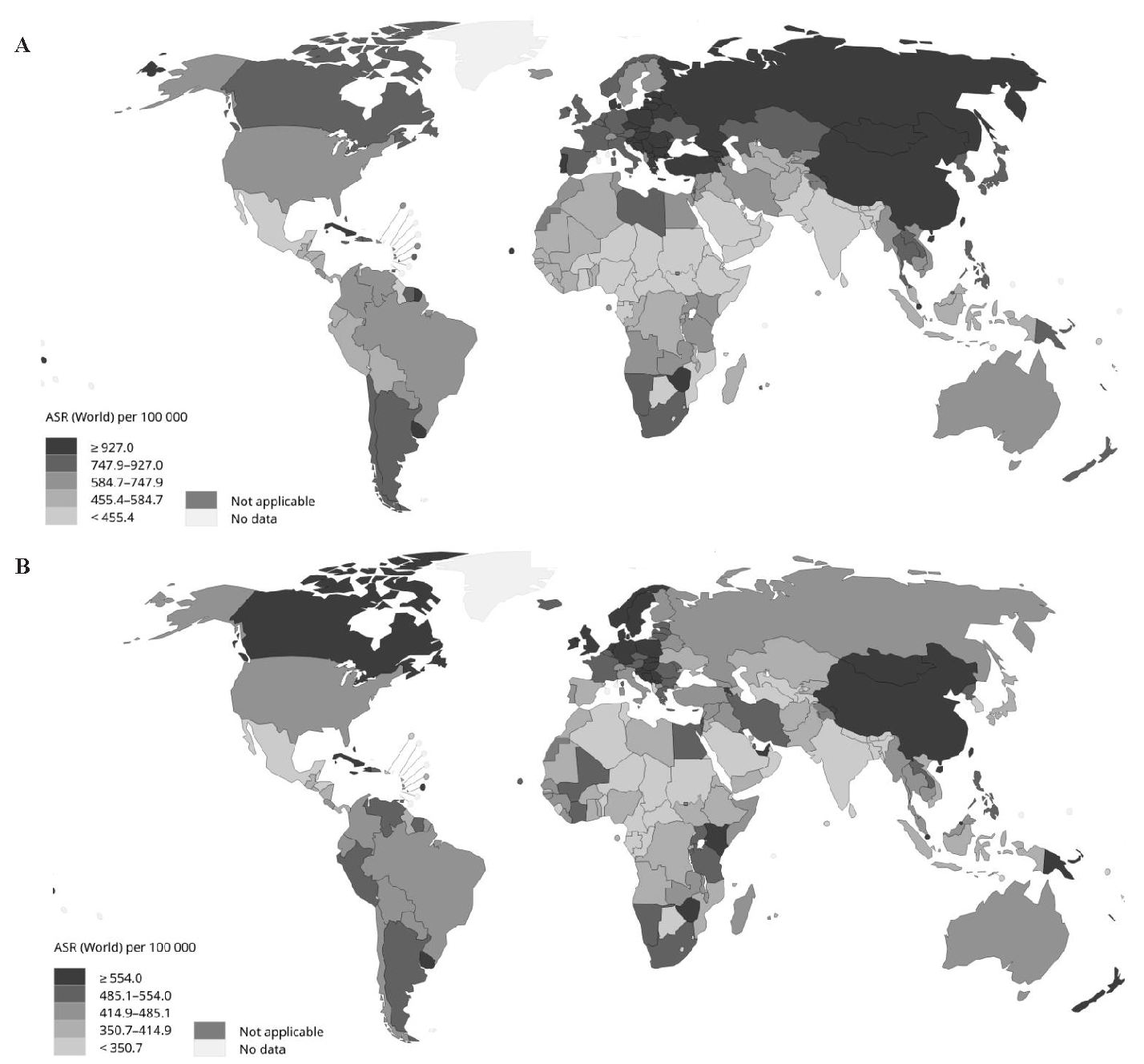
Global elderly cancer mortality rate among the older population (both sexes) is estimated as 615.1 deaths per 100,000. Highest age adjusted mortality rate is seen in Europe (706.6 deaths per 1,00,000) followed by Asia (616.1 deaths per 1,00,000), Oceania (602.5 per 100,000), Northern America (576.7 per 1,00,000), Latin-America and the Caribbean (531.7 per 1,00,000) and Africa (479 per 1,00,000) (Table I, Fig. 2).
Export to PPT
Human Development Index (HDI)-wise estimates show that high HDI countries have the highest mortality rate (704.2 deaths per 100,000), accounting for 44.6 per cent of all global mortality. This is followed by very high HDI (652.4 deaths per 100,000), which accounts for 41.3 per cent of all elderly deaths (Table I).
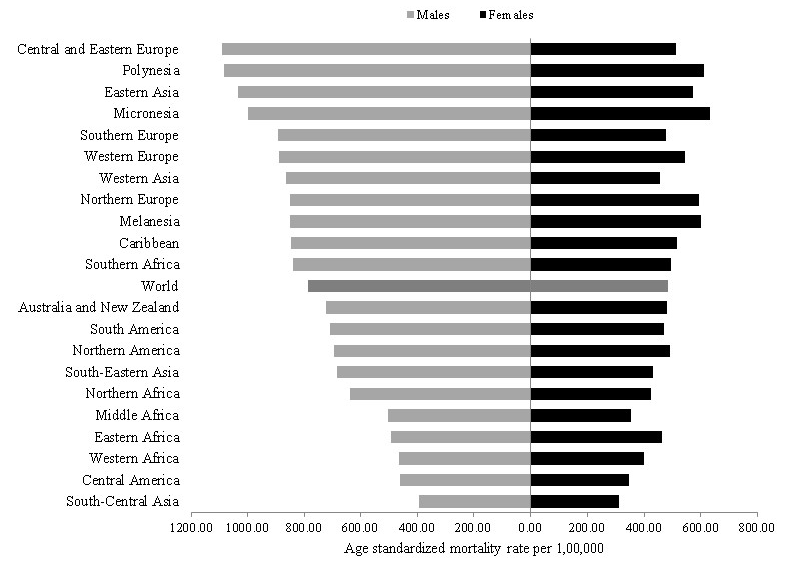
When further estimated according to the world region, it is seen that Central and Eastern Europe (1092.4 deaths per 100,000) have the highest death rate globally in elderly males and the highest death rates in elderly females is seen in Micronesia (631.7 per 1,00,000) and Oceania country. Disparity in the mortality rate is seen within continents. Stratified analysis in Asia shows that eastern Asia has the third highest mortality rate globally. Still, at the same time, South-Central Asia has the lowest mortality globally in elderly men. A difference of 163.5 per cent mortality rates in elderly males and 83.1 per cent in elderly females is seen between Eastern Asia and South-Central Asia (Fig. 3).
Export to PPT
Worldwide, the mortality rate among elderly men is estimated as 62.6 per cent higher (781.5 deaths per 1,00,000) as compared to elderly females (481 deaths per 1,00,000). The highest gender gap in mortality is observed in Europe, where mortality rates are 82.2 per cent higher in males (956.6 per 1,00,000) as compared to elderly females (525.1 per 100,000) and the lowest gap is seen in Africa, where elderly men have 29.7 per cent (552.6 per 1,00,000) higher death rate as compared to elderly females (426 per 1,00,000). The gender gap when compared by HDI, it is found that in Low HDI countries elderly men (469.2 deaths per 100,000) have 16.5 per cent higher death rates in comparison to women (402.6 deaths per 1,00,000) (Table I).
Comparison of leading cancer mortality sites by world region and sexLung cancer is the leading cause of death globally in both elderly males and females. Of all elderly deaths due to lung cancer, China alone accounts 39.1 per cent of lung cancer deaths. In elderly males, it accounts for 23.4 per cent (933108 deaths) and in elderly females, it accounts for 15.9 per cent (487303 deaths) of all global deaths (Fig. 1B). The age standardize mortality rate for elderly males is estimated as 184.2 deaths per 1,00,000 and for elderly females it is 77.7 per deaths 1,00,000. Lung cancer in elderly males is estimated as the leading cause of death in 90 countries and in females, leading cause of death in 38 countries (Table II & III; Supplementary Fig. 1).
Table II. Leading sites of mortality (deaths, relative %, age-standardized rate) for all cancers (excluding non-melanoma of skin) by sex.
Leading mortality sites, males Leading mortality sites, females Site (ICD 10 classification) Number Relative % ASR (World) Site (ICD 10 classification) Number Relative % ASR (World) Lung (C33-34) 933108 23.4 184.2 Lung (C33-34) 487303 15.9 77.7 Colorectum (C18-21) 407140 10.2 78.5 Breast (C50) 402255 13.2 65.2 Stomach (C16) 378605 9.5 74.6 Colorectum (C18-21) 341052 11.2 49.6 Prostate (C61) 358301 9 66.7 Stomach (C16) 198673 6.5 30.8 Liver (C22) 343428 8.6 69.1 Pancreas (C25) 188002 6.2 28 Oesophagus (C15) 266096 6.7 53.1 Liver (C22) 183889 6 29.3 Pancreas (C25) 192745 4.8 37.7 Cervixuteri (C53) 157641 5.2 27.8 Bladder (C67) 141259 3.5 26.6 Oesophagus (C15) 129409 4.2 20.9 Leukaemia (C91-95) 101176 2.5 19.6 Ovary (C56) 127217 4.2 21.5 Non-Hodgkin lymphoma (C82-86, C96) 97006 2.4 18.8 Non-Hodgkin lymphoma (C82-86, C96) 79803 2.6 12 Kidney (C64-65) 85896 2.2 16.8 Leukaemia (C91-95) 75166 2.5 11.5 Brain,central nervous system (C70-72) 69167 1.7 13.9 Corpusuteri (C54) 73699 2.4 11.9 Lip,oral cavity (C00-06) 60889 1.5 12.4 Brain,central nervous system (C70-72) 61655 2 10.3 Larynx (C32) 60321 1.5 12.1 Kidney (C64-65) 50035 1.6 7.5 Multiple myeloma (C88+C90) 51607 1.3 10 Bladder (C67) 47800 1.6 6.6 All cancers excl. NMSC (C00-97/C44) 3989995 100 781.5 All cancers excl. NMSC (C00-97/C44) 3056186 100 480.6Lung cancer is observed as the leading cause of mortality among elderly males in Asia (accounts for 25.1% of all deaths in Asia) with 196.2 deaths per 1,00,000, in Europe (23.9%), 243.5 deaths per 1,00,000, in Northern America (23.9%) 167.4 deaths per 100,000, and in Oceania (19.25%) 146.1 deaths per 1,00,000. In comparison, it is the second leading cause of death in Latin-America and the Caribbean (15.3%) 102.1 deaths per 1,00,000 and in Africa (10.7%) 58.2 deaths per 1,00,000.
Colorectum cancer is the second leading cause of death among the older population (both sexes), accounting for a total of 10.2 per cent of global deaths (748192 deaths) (Fig 1B). In elderly men, it is second (78.5 deaths 1,00,000), and in elderly women (49.6 deaths per 1,00,000), it is the third leading cause of death. It is estimated that in 50 countries, it is the second leading cause of death among elderly males and third leading in 74 countries. In elderly females in 51 countries, it is the second leading cause of death, and in 56 countries, it is the third leading cause of death (Table II & III; Supplementary Fig. 1).
Breast cancer among women is the second leading cause of death among elderly females (65.2 deaths per 1,00,000) accounting for a total of 13.2 per cent global deaths (Fig. 1B). Breast cancer is the leading cause of death in 82 countries and second in 70 countries (Table II & III). Region-specific estimates of breast cancer reveal that in Europe (accounts 15.3% of all deaths in Europe) with 80.9 deaths per 1,00,000, and in Latin-America and the Caribbean (14.1%) with 63.7 deaths per 1,00,000 and in Africa (18.2%) with 78.1 deaths per 1,00,000, breast cancer is the leading cause of mortality among elderly women. It ranks as number two in Oceania (13.9%) with 72.1 deaths per 1,00,000, Northern America (13.2%) with 66.4 deaths per 1,00,000 and Asia (11.5%) with 56.7 deaths per 100,000. The age-adjusted mortality rate estimated as highest in Europe (80.9 deaths per 100,000) (Supplementary Table).
Prostate cancer is the fourth leading cause of death (66.7 deaths per 100,000) representing nine per cent of all deaths among elderly men (Fig 1B). It is the leading cause of death in 75 countries and second in 59 countries. In Africa (accounts for 24% of all deaths in Africa, 138 deaths per 1,00,000) and Latin America and the Caribbean (20.3%, and with 123.2 deaths per 1,00,000), prostate cancer is the leading cause of death. A 3.6 fold variation in prostate cancer mortality rate is seen between continents, in African elderly males highest mortality rate is estimated as 122 deaths per 1,00,000 and the lowest is seen among Asian elderly males with 38.6 deaths per 1,00,000 (Supplementary Table).
Stomach cancer is the third leading cause of death globally, representing 8.2 per cent of all deaths (5,77,287 deaths) (Fig. 1B). In elderly men, it is the third leading cause of deaths (9.5%) and in elderly females, it is the fourth leading causes of deaths (6.5%). Stomach cancer is the third leading cause of death in 45 countries in elderly males and in 24 countries in elderly females (Table II & III). Among elderly males, stomach cancer is the second leading cause of death in Asia (accounting for 12.6% of all deaths in Asia) with 98.4 deaths per 1,00,000, and among elderly females, it is the fourth leading cause of death in Asia (8.6%) with 39.9 deaths per 1,00,000 (Supplementary Table).
Table III. Most common type of cancer mortality worldwide, by sex ages 60 yr and above (excl.Non Melanoma Skin Cancer)
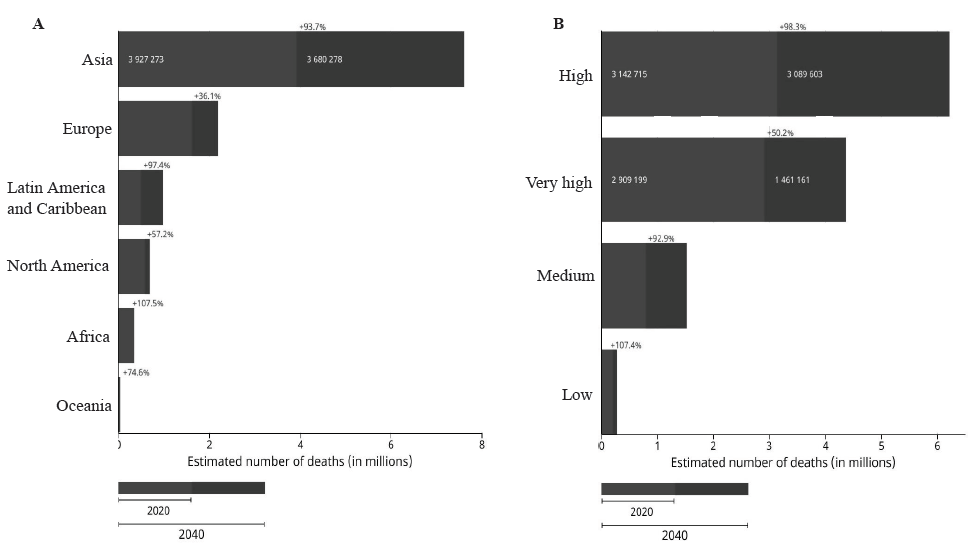
1ST 2ND 3RD 4TH 5TH Males Lung (C33-34) 90 35 20 11 14 Colorectum (C18-21) 3 50 74 26 13 Stomach (C16) 9 20 45 27 19 Prostate (C61) 75 59 18 7 9 Liver (C22) 8 37 27 11 30 Oesophagus (C15) 0 18 10 10 8 Pancreas (C25) 0 1 7 26 39 Bladder (C67) 0 4 7 12 10 Leukaemia (C91-95) 0 0 0 1 4 Non-Hodgkin lymphoma (C82-86, C96) 0 0 1 6 2 Females Lung (C33-34) 38 33 18 18 6 Breast (C50) 82 70 16 6 2 Colorectum (C18-21) 7 51 56 31 15 Stomach (C16) 5 8 24 23 19 Pancreas (C25) 0 3 24 30 20 Liver (C22) 8 13 13 28 19 Cervixuteri (C53) 43 22 17 8 15 Oesophagus (C15) 2 8 13 7 4 Ovary (C56) 0 3 14 16 46 Non-Hodgkin lymphoma (C82-86, C96) 0 0 4 2 3 Future burden of deaths by world regions and HDIThe overall future cancer deaths among the elderly are estimated to increase from 7.05 to 12.7 million deaths representing a total 80.2 per cent increase in deaths by 2040. The highest estimated number of deaths in elderly is predicted to increase in Asia by 93.7 per cent (from 3.93 to 7.61 million deaths), followed by Europe from 1.62 to 2.21 million (36.1% increase), Latin-America and Carrabin from 0.51 to 1 million (97.4%), Northern America from 0.58 to 0.92 million (57.2% increase), Africa from 0.035 to 0.73 million (107.5%) and in Oceania from 0.06 to 0.1 million (74.6% increase) (Fig. 4).
Export to PPT
In HDI-wise prediction, it is estimated that the highest burden of deaths will be in high HDI countries with an increase of 98.3 per cent (from 3.14 to 6.23 million deaths), followed by very high HDI by 50.2 per cent (2.91to 4.37 million), medium HDI (0.79 to 1.53 million) and low HDI (0.2 to 0.41 million).
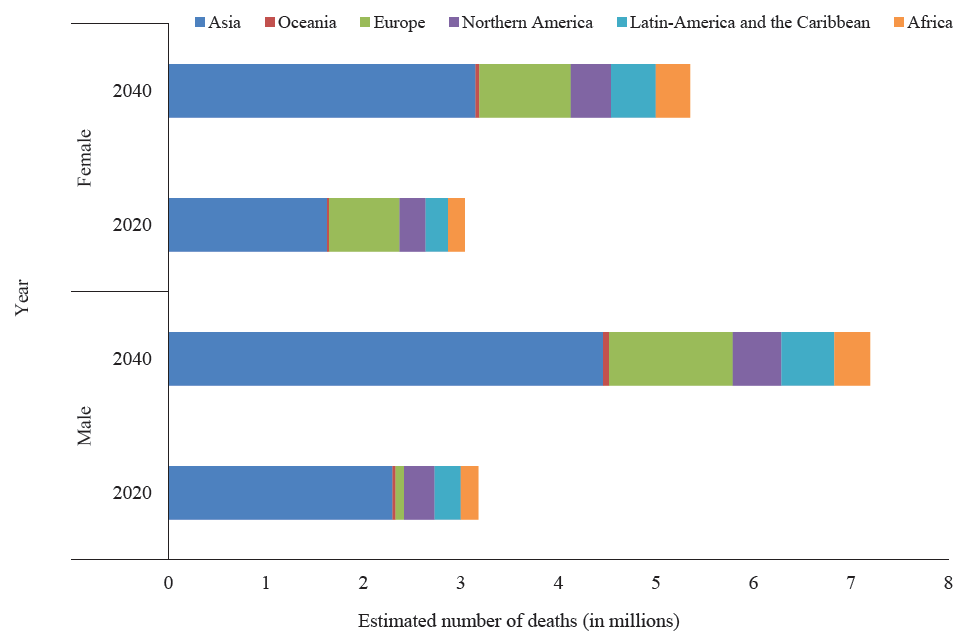
Future burden of deaths by gender and siteBy 2040, it is predicted that Asia will see the highest number of deaths among both males and females, with an estimated 4.46 million male deaths and 3.15 million female deaths, followed by Europe with 1.27 million male deaths and 0.94 million female deaths. The highest relative change in death percentage is expected in Africa, with a projected increase of 109.7 per cent in cancer deaths among males and 105.3 per cent deaths among females (Fig. 5). The leading future burden of cancer-related deaths among older adults is projected to be from lung cancer, with a relative increase of 78.4 per cent compared to 2020 estimates, resulting in an estimated 2.53 million deaths for both sexes in 2040. This will be followed by stomach cancer (79.5% increase, 1.04 million deaths), liver cancer (75.1% increase, 0.92 million deaths), prostate cancer (100.4% increase, 0.72 million deaths), and breast cancer (73.6% increase, 0.7 million deaths).
Export to PPT
DiscussionGlobally, cancer is either the first or second leading cause of death in 112 countries, according to the World Health Organization (WHO) estimates2. We estimated that cancer in older adults accounts for 71.2 per cent of all cancer (excluding NMSC) deaths globally and is projected to be on the rise from 7.05 to 12.7 million by 2040. The majority of the cancer burden falls in LMIC; Asia alone shares 55.7 per cent of global deaths. These patients were mostly diagnosed at a late stage where palliative treatment only can be an option. However, according to the lancet commission 2018 report, 80 per cent people living in LMICs have very limited or no access to pain and palliative care relief13.
Compared to younger, older cancer patients face a wider range of non-cancer-related issues, such as frailty and cognitive deterioration, which makes palliative care more challenging for them14. Also, geriatric syndromes are more prevalent in them due to shared risk factors like advanced age, cognitive impairment, functional disability, and restricted mobility, for which these group of patients are more likely to experience unfavourable outcomes and lower quality of life15.
Of all estimated cancer deaths among elderly males leading five cancers account for 60.7 per cent of deaths and among elderly females, it accounts for 53 per cent of all deaths. Deaths due to lung cancer is most common in both males (23.4%) and females (15.9%), whereas colorectum cancer is the second leading cause of death among elderly males (10.2%) and third leading cause in elderly females (11.2%). Among elderly females, breast cancer is the second leading causes of death, accounting for a total of 13.2 per cent of all elderly cancer deaths.
The overall mortality rate for lung cancer was 62 per cent higher in elderly males as compared to elderly females. Micronesia followed by Polynesia and Central and Eastern Europe (Supplementary Fig. 2) have the highest mortality rates globally. In high-income countries, lung cancer is higher mainly because of the higher prevalence of smoking, and about two thirds of the deaths in these countries were due to lung cancer16, which can be prevented through adequate tobacco regulations and policy. Lung cancer is lethal, and the mortality to incidence ratio for lung cancer (all ages) is reported as 82 per cent, which suggests the higher death rate due to lung cancer17. In lower or lower medium-income countries the survival rate for lung cancer ranges from 10 to 20 per cent, which is mainly because of late stage at diagnosis18. Low dose computed tomography (LDCT) based screening shows the potential to reduce lung cancer mortality, as per the estimates of both the National Lung Screening Trial and Multicentre Italian Lung Detection trials19,20.
Histological subtypes and molecular biological aspects play important roles in patients’ prognosis of the disease; somatic mutation was found significantly associated with increased age21,22. Older adults are mostly found to be diagnosed with non-small cell lung cancer (NSCLC), and the five-yr survival significantly varies according to their subtypes. A lower survival rate is seen in squamous cell carcinoma (SCC), which is more prevalent in older adults, than adenocarcinoma, which is more prevalent in younger ones23-25.
With a six-fold variation in death rates globally, colorectum cancer is the second leading cause of cancer mortality (both sexes) among the elderly and the highest rate of mortality is seen in Europe and lowest in South-Central Asia (Supplementary Fig. 3). Recent trend analysis of mortality rates (1990-2019) shows that in high income countries colorectal cancer mortality rates have been declining mainly due to effective screening programmes, as in Australia the age standardized mortality rate decreased by 33.5 per cent and in North America by 25.3 per cent26,27. Importantly, CIMP-high tumours are mostly associated with poor histological differentiation in colorectal cancer and are mostly prevalent among older adults28,29.
The highest mortality rate of stomach cancer is seen in Eastern Asia (Mongolia has the highest incidence and mortality rate in both males and females). In contrast, lower rates are seen in Northern America and Australia and New Zealand (Supplementary Fig. 4). However, there is diversity in incidence and mortality rates vary among regions; countries like Japan and Korea has high incidence rates globally but considerably low mortality rates. This may be due to the adoption of different screening programmes like National guidelines for gastric cancer screening in 2001 by Korean Gastric Cancer Association or Insurance coverage for a gastric cancer prevention programme by the Japanese government30,31.
Female breast cancer is the second leading cause of death among elderly females globally. Place of residence and socio-economic status are significantly associated with breast cancer incidence and mortality (Supplementary Fig. 5). Population-based survival (CONCORD programme) of breast cancer shows the five-yr net survival estimates range from higher than 85 per cent in many high-income countries to less than 60 per cent in some regions of sub-Saharan Africa, and country-specific survival estimates are as low as 12 per cent in Uganda32. These disparities are mainly because of inequalities in treatment facilities across the globe, mainly linked to inadequate access to diagnostic facilities in lower or lower middle-income countries and also late stage at presentation33,34. WHO recommends population-based mammography screening every two yr for women aged between 50–69 yr, which can be helpful for early detection of cases35.
Ageing is the most important non-modifiable biological risk factor for cancer. This will make the role of geriatric oncology vital in the coming yr, in ensuring older patients functional and nutritional status, social support, cognition, and psychosocial function36, especially in LMIC like India, where it is seen that 98 per cent of the older patients have at least one deficit37 and resources are limited.
However, older patients are often not included in randomized trials for which risk and benefits assessment could not to done. Likewise, the lack of evidence available on the benefits of breast cancer screening is due to the fact that screening above 75 yr is not recommended38,39. Studies have shown that elderly patients can also benefit from cessation of smoking or alcohol, weight management, and social support40,41. Local preventive strategies should also be developed with a focus on cancer types responsible for higher deaths.
This investigation did have some limitations, hence caution exercised while interpreting the results. Firstly, the data quality, particularly national cancer mortality registry, is not uniform across all countries. This may affect the estimations, and it is impossible to rule out overestimation or underestimation. Secondly, IARC data repository on cancer did not provide country-specific deaths by causes, for which association with death rate is not possible. However, despite these limitations, Globocan (IARC-WHO) remains as a reliable global data source to understand the pattern of cancer deaths.
留言 (0)