The effects of serial intravitreal anti-VEGF treatment with PI asepsis on the ocular surface and MG were investigated in the present study. In contrast to our hypothesis that repeated exposure to PI may affect the ocular surface and MG morphology, the present study showed that serial IVI procedures with PI asepsis resulted in no difference in NITBUT, Schirmer, corneal staining, or MG loss compared to untreated fellow eyes in patients with nAMD.
The primary concern with repeated anti-VEGF therapy is the risk of endophthalmitis, prompting a standardized antisepsis procedure on the ocular surface before each IVI to reduce this risk [12]. PI is favored for its broad antimicrobial spectrum, as it can effectively target various microorganisms, including antibiotic-resistant strains [13]. Studies have demonstrated acute damage to the ocular surface following IVI, mostly as a result of the acute toxic effect of PI on the corneal epithelium, which depends on its concentration [6, 7]. Additionally, the impact of perioperative use of topical antibiotics and anesthetics on the ocular surface should be noted. However, there is potential for ocular surface recovery between IVI intervals. Understanding the long-term effects of serial IVI on the ocular surface is crucial for its management.
Chronic exposure to PI antisepsis due to the need for repeated IVI in the treatment of nAMD raises concerns about the possibility of DED induction/exacerbation in this cohort. The present study revealed no significant differences in the fNITBUT, avgNITBUT, Schirmer test, or Oxford score between IVI-treated eyes and untreated fellow eyes in nAMD patients. Recently, in their meta-analysis of the effect of serial IVI procedures on DED, Gao et al. also revealed that there was a significant increase in the OSDI score and osmolarity of the tear film, but there was no significant difference between treated and untreated eyes in the fluorescein TBUT, fNITBUT, avgNITBUT, or Schirmer test [14]. On the other hand, there was no correlation between IVI number and OSDI score in the present study. This result may have been affected by the relatively limited range of IVIs. The IVIS study also revealed no relationship between the OSDI score and the number of IVIs received [15].
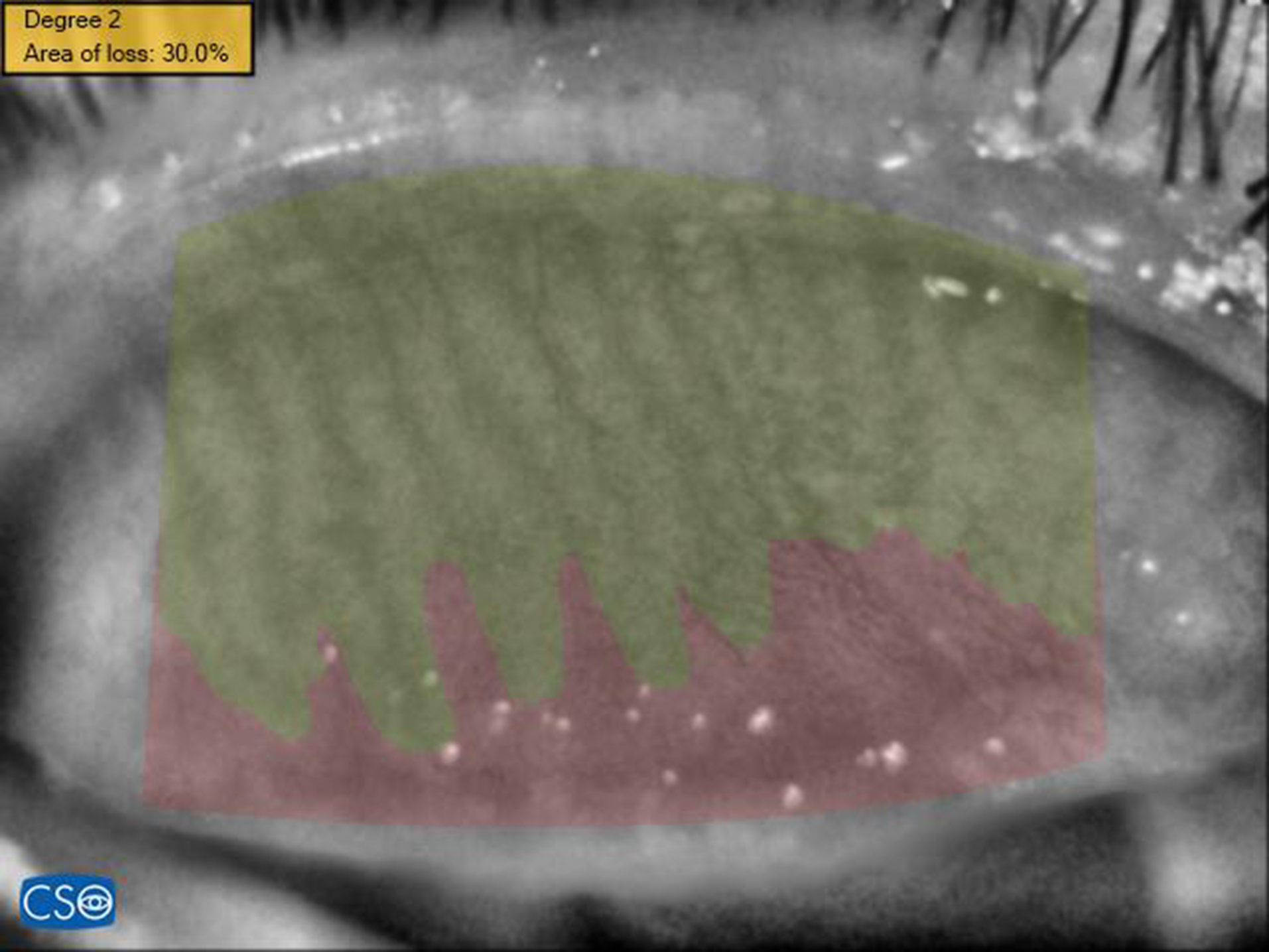
MGs are responsible for the secretion of the lipid layer of the tear film, which maintains tear film stability. MGD is associated with evaporative DED [16]. There are conflicting findings regarding the impact of anti-VEGF treatment procedures on MG structure [17,18,19]. Kiyat et al. and Polat et al. revealed significant MG loss in the IVI treatment group [17, 18]. However, they both prescribed topical antibiotics for prophylaxis of endophthalmitis, which may have increased the exposure burden to MG. In addition, in the latter, comparison to healthy controls and the presence of diabetes may have affected the results. In contrast, Malmin et al. reported reduced MG loss in nAMD eyes treated with IVI, which was attributed to decreased inflammation of the eyelid that continued after treatment owing to the anti-VEGF agent or PI itself [19]. Our results showed no significant difference in MG loss between treated eyes and untreated fellow eyes, but there was a significant correlation with aging, as reported previously [20]. It may also prevent MG loss in the present study because no patient received topical medication after IVI.
Another aspect to consider is whether anti-VEGF treatment itself might influence dry eye measures and MG. VEGF is a proinflammatory agent that promotes the release of cytokines such as interleukin 6 and 8, as well as tumor necrosis factor-a [21]. VEGF levels are greater in tears from DED patients than in those from healthy controls [22]. Jiang et al. revealed that anti-VEGF administration to the MG improves dry eye measurements, such as conjunctival redness and tear break-up time, in patients with MGD [23]. While systemic absorption of anti-VEGF agents is generally low, potential effects on nearby tissues cannot be entirely dismissed [24, 25].
The present study had several limitations, including its cross-sectional design, semiautomatic evaluation of MG loss, and lack of tear osmolarity measurement and staining with lisamine green. Although the fellow untreated eye was used as the control group in the present study to mitigate the impact of systemic conditions on the results, the lack of a detailed analysis of systemic diseases and medications used by the participants can also be considered another limitation of the study [26]. Therefore, a prospective multicenter clinical study with a larger sample size and longer follow-up period may be warranted in the future to reveal the longitudinal effect of IVIs on the ocular surface, MG loss and DED.
In conclusion, the results of the present study demonstrated that serial IVI of anti-VEGF agents with PI asepsis is well tolerated by nAMD patients in terms of ocular surface area, MG loss and DED measurements. The ocular surface may partially recover after IVI procedures. After undergoing IVI procedures, there might be some improvement in the condition of the ocular surface. Since dry eye significantly affects quality of life, it is important to closely monitor patients’ ocular surface health during the perioperative period. More research, particularly prospective studies focusing on various aspects of dry eye, is needed to confirm these findings and better understand the underlying mechanisms involved.








留言 (0)