
記住我

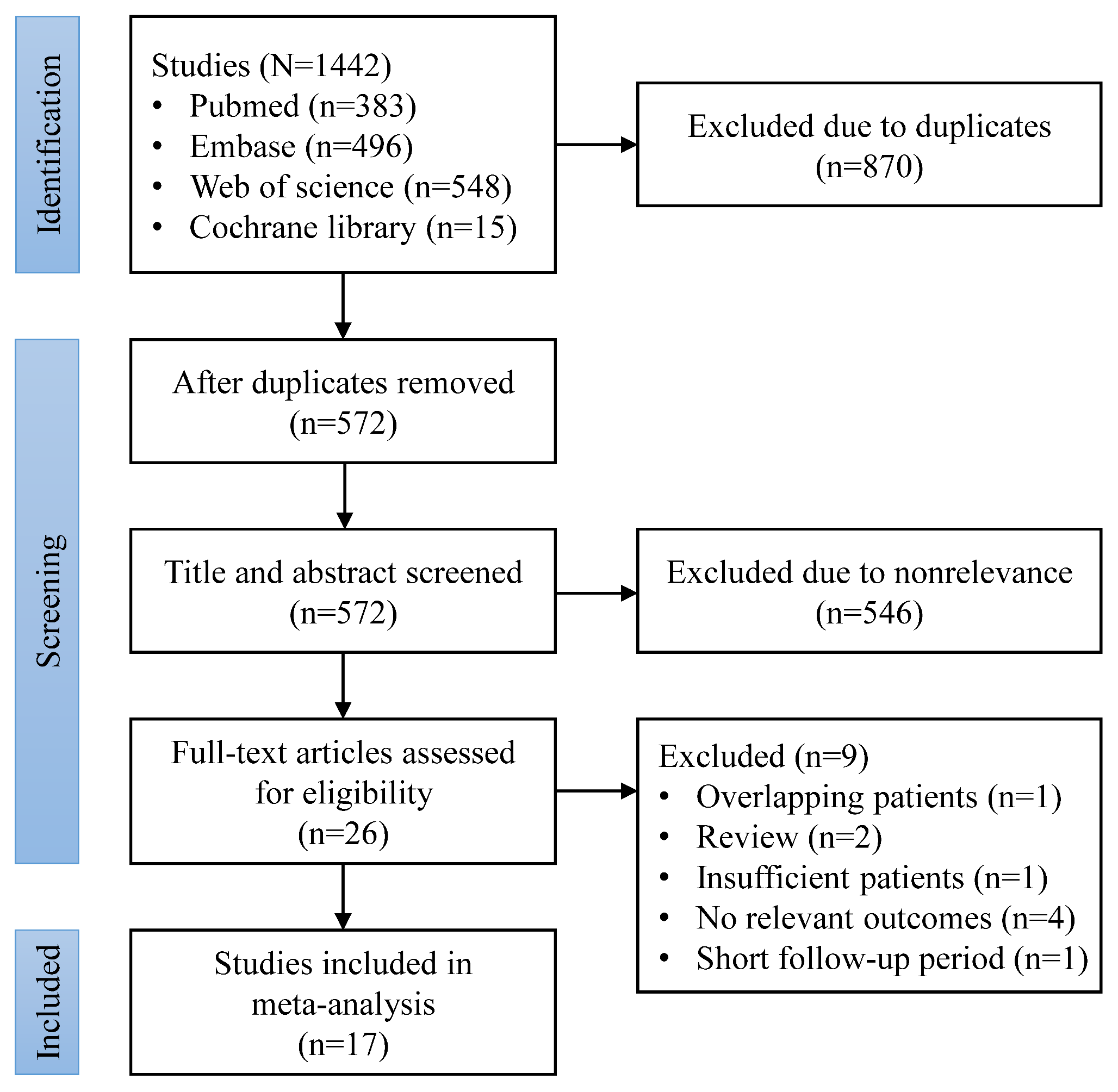







A systematic search for the articles was performed on 13 June 2024. From PubMed, 555 articles were exported, 186 from Web of Science, 122 from Cochrane Reviews, 439 from Scopus, and 655 from Embase databases. A total of 1957 of articles were imported into Zotero bibliography manager. Before the duplicate removal, four retracted articles were removed (one had copyright issues, two were randomly generated, and one violated ethical standards). From 1953 articles, 671 duplicate articles were found, which were removed before the screening. Over 1282 articles were screened, which lead to further full-text screening of 54 potentially eligible journal articles. From 54 articles, seventeen studies related to non-clinical technical trials, three non-English articles (all three Chinese), five articles not within the scope of this systematic review (application of robotics in different interventions or microscope assist), eight review articles, two clinical trial protocols, one with duplicate results, and three abstract-only papers were excluded from this synthesis. We have also found two studies through manual searching. Finally, 17 articles were included for systematic review, while 13 for meta-analysis [12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28]. Notably Zhao et al. study, while possessed a control group, lacked details regarding robotic group (number of patients, and outcomes) to be included into meta-analysis. A PRISMA flow-diagram for systematic search process is available as Fig. 1 to this paper.
Fig. 1
Most of the included studies (and all of them in meta-analysis) were from People’s Republic of China, one from USA, and one from Taiwan. Eight studies used ROSA robotic systems, four used Remebot, three used CAS-R-2, and two Sinovation SR1. In terms of control group, three studies were single-arm, three were evaluated to hematoma aspiration, six to conservative treatment, three to endoscopy, and two to craniotomy surgery. Only one study applied robot for RA neuro-endoscopy, while other papers have described RA puncture aspiration. Patient group sizes varied, however no group (robotic nor control) exceeded more than 100 patients in any of the included studies. Blood pressure (systolic & diastolic), and NIHHS score were relatively uncommonly reported. Initial GCS score varied from moderate to severe between the included studies. Hematoma volume, time from onset to surgery, type, and location also varied between included studies in this paper. Table 1 provides information about the basic demographic information from the included studies.
Bias evaluationOnly one randomized trial was conducted, and generally showed bias in terms of missing outcome data (patients from robotic group were missing), measurement of outcome, and deviations from intended intervention. Hence, bias concerns were raised about this study.
For other, non-randomized studies, we have also found various biases. Studies reported very selective inclusion criteria, decision on surgery was often affected by family due to the concerns to new technology, presence of retrospective design among the studies, missing patients at follow-up, or unclear measurement of the outcomes in some studies only complicated the unbiased evaluation of the results. Figure 2 provides detailed analysis of the bias assessment.
Fig. 2
Bias evaluation for RoB2 (upper) and ROBINS-I (lower) tools
OutcomesLong-term mortalityMortality was reported in nine studies, favoring robotically-assisted surgery (OR 0.3652 [0.1457; 0.9158], p = 0.0317), and indicating a lower mortality rate. High heterogeneity was observed among the studies (I2 = 68%).
[NOTE: Short-term deaths from Xu et al. were removed to maintain consistency among the studies and analyzed in secondary outcomes. Jin and Han have separately analyzed short term deaths, and these were also analyzed in secondary outcomes.]
Interestingly, the control subgroups revealed that craniotomy, endoscopy, or conservative approach were not inferior to robotic surgery (Fig. 3). The severe GCS subgroup showed statistically significant result (OR [0.08; 0.76]), while moderate did not. Hematoma volume subgroups revealed no statistically significant results. Remebot and Sinovation models achieved statistically significant results, while ROSA and CAS-R-2 did not.
Fig. 3
The funnel plot for mortality is shown in Fig. 4. ID analysis and Baujat plot revealed Tang study as an outlier. Therefore, we have applied leave-one out analysis, and exclusion of this yielded statistically significant results (OR 0.51 [0.26; 0.98]), and lowered heterogeneity (I2 = 22%).
Fig. 4
In a sensitivity analysis limited to puncture robotic aspiration (PR) interventions (exclusion of Wu et al. study, where robotic neuro-endoscopy was performed), PR intervention had favorable mortality outcome (OR 0.3447 [0.1292; 0.9195]).
Notably, Zhong et al. have reported mortality outcome without control data. Therefore, we assumed, that control had zero mortality events. When included in the sensitivity mortality analysis, effect size yielded a non-significant result (OR 0.4067 [0.1651; 1.0018], p = 0.0505).
Detailed sensitivity analyzes regarding mortality outcome are visualized in Supplementary Figs. 1–28.
RebleedingA smaller incidence of rebleeding events significantly favored robotic-assistance (0.3192 [0.1384; 0.7360], p = 0.0074). The studies reported homogenous results (I2 = 0.0%). This was also confirmed by prediction interval [0.11; 0.91]. Comparative subgroup analysis (Fig. 5) showed that RA surgery was more favorable compared to puncture aspiration interventions (OR 0.0857 [0.0157; 0.4675]). Subgroup analyzes of robot models & GCS revealed no statistically significant results. However, 20–40 mL hematoma volume subgroup achieved statistically significant result favoring RA surgery (OR 0.16 [0.05; 0.54], I2 = 0%).
Fig. 5
Influence diagnostic sensitivity analysis revealed no outliers, while Baujat plot identified Liang and Wang studies as outliers. Exclusion of Wang lead to increased effect size (OR 0.25 [0.10; 0.59], I2 = 0%), while exclusion of Liang lead to statistically insignificant result.
PR interventions also had favorable outcome for rebleeding events (OR 0.3132 [0.1231; 0.7970], p = 0.0148).
In the sensitivity analysis for rebleeding events, we have assumed no events in Xu et al. study, as authors have not provided sufficient data in control. The result remained statistically significant (OR 0.3873 [0.1597; 0.9392], p = 0.0358), with low heterogeneity (I2 = 14.5%).
Sensitivity analyses figures are visualized in Supplementary Figs. 29–57.
Surgery timeSurgery time strongly favored robotically-assisted interventions (MD -86.2447 [-128.5111; -43.9782], p < 0.0001), but extremely high heterogeneity was observed (I2 = 99.2%).
ID sensitivity analysis revealed, that Jin and Liang studies mostly contributed to the heterogeneity, what was confirmed by Baujat plot. Leave-one out sensitivity analysis had not solved the high heterogeneity value.
In control subgroup, only in craniotomy result was statistically significant (Fig. 6). None of the subgroups reduced the high heterogeneity.
Fig. 6
PR studies have also reported favorable surgery time (MD -99.8341 [-156.4745; -43.1938]), however high heterogeneity remained among the studies. The high heterogeneity of surgery time could be caused by differences in control procedures, staff experience, surgery admission, different locations of hematoma, geographical location, or presence of urgency cases, which were not fully analyzed due to the very limited data from the studies.
Sensitivity analyses figures are visualized in Supplementary Figs. 58–76.
Intracranial infectionIntracranial infection was reported by five studies (Fig. 7) and favored robotic surgery (OR 0.3068 [0.1182; 0.7961], p = 0.0152). No heterogeneity was observed (I2 = 0%).
Fig. 7
ID sensitivity analysis revealed Jin, as an outlier study. Leave-one out analysis without Jin maintained favorable effect size.
Sensitivity analyses figures are visualized in Supplementary Figs. 77–85.
Hospital stayHospitalization duration was not shortened with RA surgery (MD -2.8487 [-5.7933; 0.0959], p = 0.0579). Additionally, a high heterogeneity was observed (I2 = 90.9%).
ID sensitivity analysis revealed Xu study as an outlier. In leave-one out sensitivity analysis, exclusion of Xu et al. study reduced heterogeneity (I2 = 30%), and resulted in a favorable effect size (MD -1.930 [-3.115; -0.746]).
Subgroup analysis revealed a significantly shorter stay when compared to craniotomy (MD -2.1795 [ -3.3689; -0.9900], I2 = 1%). A favorable mean difference was also observed in patients with moderate GCS (MD -1.9550 [-3.6168; -0.2933]).
Sensitivity analysis with PR studies had not achieved statistically significant difference.
Sensitivity analyzes figures are visualized as Supplementary Figs. 86–105.
Pulmonary infectionPulmonary infection was reported in six studies and achieved favorable effect for robotic surgery (OR 0.3770 [0.2408; 0.5902], p < 0.0001). Almost no heterogeneity was present (I2 = 3%). Additionally, RA surgery was more favorable compared to craniotomy and conservative treatment, but not superior to endoscopic surgery (Fig. 8).
Fig. 8
ID sensitivity analysis revealed Zou study as an outlier and in leave-one out analysis, exclusion of this trial resulted in even stronger effect size (OR 0.297 [0.180; 0.491]).
PR sensitivity analysis also favored RA surgery (OR 0.3780 [0.2240; 0.6379], p = 0.0003) and low heterogeneity was present (I2 = 22%).
Sensitivity analyzes figures are visualized as Supplementary Figs. 106–124.
Mean modified ranking scaleMean MRS was lower in RA group (MD -0.8063 [-1.0786; -0.5341], p < 0.0001). However, notable heterogeneity was present (I2 = 71%).
ID sensitivity analysis revealed both Tang & Han as outlier studies. A leave-one out analysis was performed, and exclusion of Tang reduced heterogeneity below 50% (I2 = 43%), while exclusion of Han still led to high heterogeneity (I2 = 61%).
In subgroup analyzes, RA surgery resulted in more favorable MRS compared to craniotomy, conservative, or endoscopy treatment. Mean MRS was more favorable for RA in both moderate and severe GCS subgroups. Additionally, more favorable mean MRS was reported in all three volume subgroups. All robots (ROSA, SR1 and Remebot) except CAS-R-2 performed better (lower mean MRS) than control.
In PR sensitivity analysis, the effect size remained favorable for RA group (MD -0.8056 [-1.1237; -0.4875], p < 0.0001). However, high heterogeneity remained.
Sensitivity analyzes figures are visualized as Supplementary Figs. 125–144.
Secondary outcomesGOS was higher in RA surgery (MD 0.6792 [0.1599; 1.1985], p = 0.0104). High heterogeneity was present (I2 = 91.8%). Exclusion of Xu study led to reduction of heterogeneity to 0%, while effect size remained statistically significant. GOS in PR studies was also favorable (MD 0.6934 [0.0809; 1.3060], p = 0.0265), however heterogeneity was even higher (I2 = 95%).
The incidence of digestive track hemorrhage had no statistically significant difference between intervention and control. The number of patients with favorable MRS score remained statistically insignificant.
Mean GCS score was higher in RA group (MD 1.9387 [0.8215; 3.0559], p = 0.0007). Hematoma reduction (%) has not achieved statistically significant result. Short-term mortality was non-inferior in control groups.
Hospitalization cost has not reached a statistically significant difference. The cost of robotic surgery was lower compared to conventional surgical strategies, but not than conservative treatment. This was confirmed in leave-one out sensitivity analysis.
Detailed economical evaluation was described in Tan et al. study, where authors have applied a Markov model to simulate 10-year disease progression. RA surgery had significantly lower costs for one year and ten-year simulation compared to endoscopic surgery. Patients in the Remebot surgery group saved ¥36,862.14 per capita compared to the neuro-endoscopic group, and over a 10-year period, the savings per patient for the robotic surgery group increased to ¥40,442.19. Total hospital costs were also significantly lower in the Remebot group. This includes the perioperative expense, medical care costs, and patient lost wages due to hospitalization. Average hospital cost was ¥50,516 for Remebot surgery and ¥89,155 for neuro-endoscopic surgery Additionally, Remebot surgery showed an increase with 0.062 additional quality-adjusted life years (QALYs) gained per patient in the first year and 0.463 additional QALYs gained after 10 years compared to endoscopic surgery.
Secondary outcomes figures are visualized as Supplementary Figs. 145–162. Table 2 summarizes all analyzed outcomes and subgroups.
Table 2 Overview of results. Results for subgroups are presented as effect size [95% CI]
留言 (0)