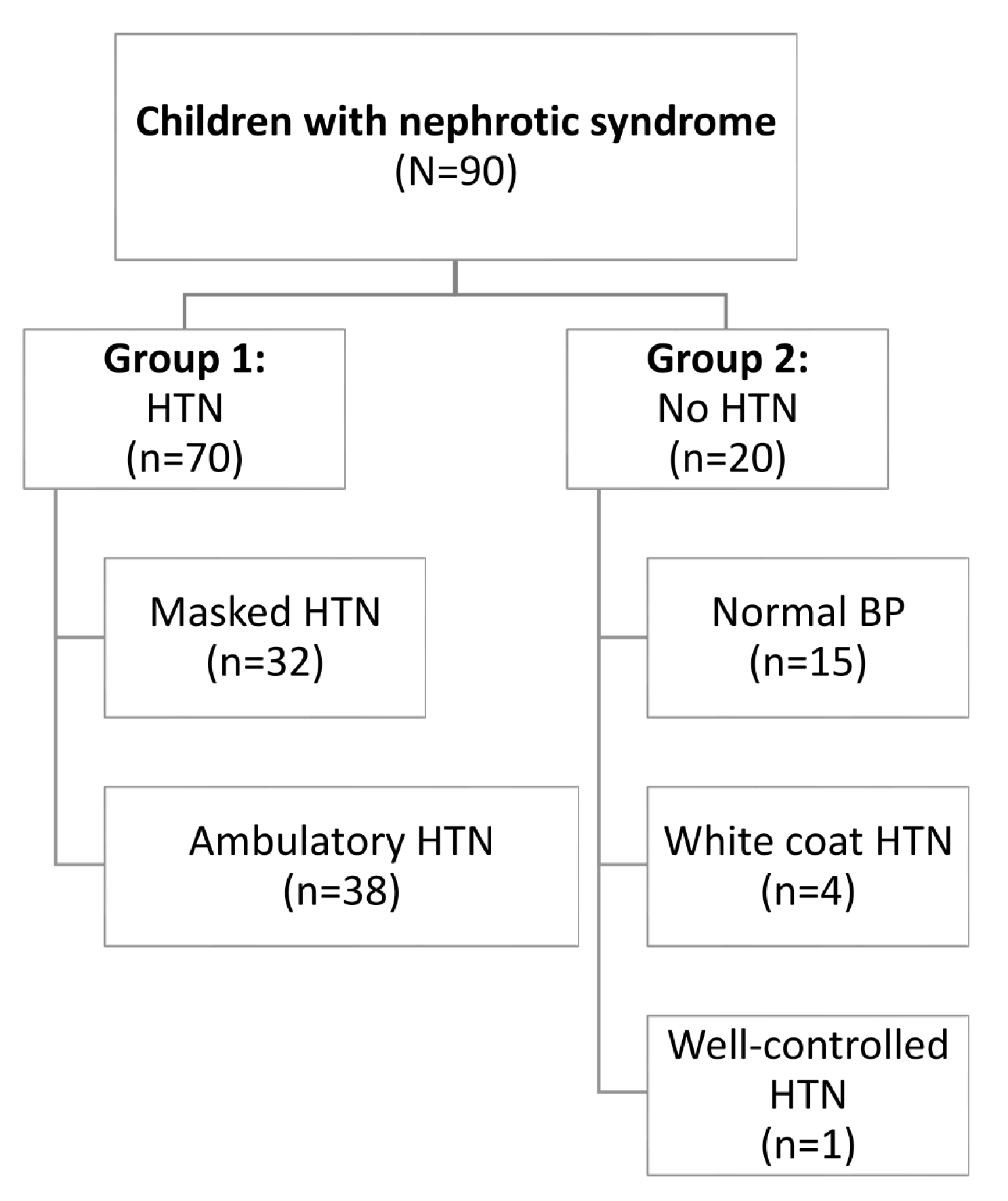
The present work showed that about two thirds (n = 70/90) of the children with nephrotic syndrome had either ambulatory (n = 38/90) or masked hypertension (n = 32/90).
In addition to higher serum urea and lower serum albumin levels being significantly associated with hypertension in children with nephrotic syndrome, increased BMI was found to be associated with hypertension in such children.
Children with nephrotic syndrome who were also hypertensive also had evidence of LVH and a significantly higher IVS z score. This highlights how crucial it is to use ABPM in children with nephrotic syndrome in order to improve their prognosis and reduce long-term morbidities, particularly those related to the cardiovascular system.
Manasa and others found that the prevalence of hypertension is more in steroid dependent nephrotic syndrome than steroid resistant NS which is not detected in our study as there is no significant difference between SRNS and SDNS either males or females in ours [17].
Analyzing the blood pressure characteristics in the studied group yields several noteworthy insights. Firstly, between the two groups, all the overall, morning, night, blood pressure measurements were significantly higher in the hypertensive group, p < 0.001, all the MAP, PP measurements, and blood pressure high readings were significantly higher in the hypertensive group, p < 0.001. while there was no significant difference between the two groups regarding the pulse average overall, SBP D/N index or DBP D/N index, p > 0.05. This significant difference is a clear indicator of the heightened cardiovascular risk in the hypertensive cohort. Moreover, the SBP and DBP percentiles for age also showed significant differences, with the HTN group having higher mean percentiles (SBP: 99 ± 1.9, DBP: 95.6 ± 5.5) than the non-HTN group (SBP: 77.5 ± 14.9, DBP: 78.5 ± 12.8), p-values < 0.001. These findings suggest a pronounced deviation from the normal blood pressure range in the hypertensive group, emphasizing the severity of hypertension in these patients and the persistence of hypertension throughout the day, with no significant reduction during nocturnal periods, which is often expected in healthy individuals. All of that highlighting the need for meticulous blood pressure monitoring and management in patients with nephrotic syndrome [18].
Most of hypertensive patients were SBP non-dippers (74.3% of hypertensive group), with a significant difference with the non-hypertensive group (p = 0.045), indicating a pronounced absence of typical nocturnal SBP reduction which is clinically relevant as it is typically associated with higher cardiovascular risks and may necessitate more aggressive management strategies. While there was no significant difference between the two groups regarding the rate of DBP night dipping, p > 0.05. Ninety-nine children with frequently relapsing NS were included in a study that evaluated ABPM; of them, 72 had nocturnal non-dipping, and 55 had a high nocturnal systolic blood pressure load [19]. In a second, smaller group of 21 patients with primary NS, diurnal blood pressure anomalies and a high frequency of overnight hypertension were also seen. Of these individuals, 8 (38%) had daytime hypertension, 13 (62%) had nighttime hypertension, and 13 (62%) did not dip [20]. Similar findings were seen in another study, where 25 out of 37 patients (68%) did not engage in nocturnal dipping; 14 of these patients did not dip for either SBP or BP, and the remaining patients did not dip for SBP alone [21].
Regarding the risk factors of hypertension, clinically, none of the patients of group 2 (the non-hypertensive group) were found to have pleural effusion or ascites, but the difference between the two groups were non-significant p–values were 0.091 and 0.054 respectively. The absence of a significant difference could also imply that these complications are more closely related to other aspects of nephrotic syndrome, such as the severity of proteinuria, the degree of hypoalbuminemia which is more prevalence in hypertensive group1, or overall fluid status, rather than the presence of hypertension alone.
The second clinical risk of hypertension in our study that overall z-score of BMI of hypertensive group 1 is significantly higher than non-hypertensive group 2 with p-value: 0.029. It contrasts with the Keshri et al. study, which found no discernible variation between the nephrotic children’s BMI and the incidence of hypertension [22].
In children with NS, the impact of steroid therapy on blood pressure varies. Steroid therapy may cause hypertension (HTTN) or worsen pre-existing hypertension (HTTN) in certain people with NS, while high dosage steroid therapy improves blood pressure in other patients after remission [19].
This could be explained by that the patients on steroid therapy that have hypertension developed significant sodium retention, decreased renin and aldosterone levels, and hypervolemia. However, with steroid therapy, patients who are normo- or hypovolemic experience significant diuresis and natriuresis. Complex interactions between hereditary and environmental factors may be the cause of the variability in how steroids affect blood pressure [19].
In addition, in the current study it was observed that, distinctions in mean serum urea and albumin levels, along with the presence of pus and casts in the urine, between the hypertensive (HTN) and non-hypertensive (non-HTN) groups that yield significant insights into the interplay of hypertension and pediatric nephrotic syndrome. The HTN group displayed a higher mean serum urea level (23.8 ± 22) in comparison to the non-HTN group (13.7 ± 6.1), with a statistically significant difference (p = 0.047). This may be explained by elevated blood urea despite normal serum creatinine, which is linked to the children’s hypovolemic state. This, in turn, activates the Renin-Angiotensin System (RAS), which causes hypertension in such children [23].
Furthermore, the HTN group exhibited a lower mean serum albumin level (2.8 ± 1.2) than the non-HTN group (3.5 ± 1.3), with a significant p-value of 0.017. This implies a more severe protein loss in hypertensive patients, considering hypoalbuminemia as a hallmark of nephrotic syndrome which may be attributed to increased glomerular damage or a more severe manifestation of the disease [24].
Hypoalbuminemia, a hallmark of Nephrotic syndrome, leads to decreased plasma oncotic pressure and subsequent fluid shifts into the interstitial space, causing edema. The body’s compensatory mechanisms, including activation of the renin-angiotensin-aldosterone system, may contribute to elevated blood pressure, particularly in pediatric patients [25]. In our patients, there was a significant negative correlations between the serum albumin and SBP percentile for age (p: 0.017, r: -0.250) and DBP percentile for age (p: 0.008, r: -0.277).
In a study done on 207 hypertensive children, there were 51.21% of cases were non-dippers, total cholesterol level was significantly higher in non-dippers than dippers (4.34 vs. 3.99 mmol/L, p-value :0 0.034) [26]. Among our group 1, it was noticed that 74% (n = 52/70) of them were systolic non-dipper, also it was observed that the mean serum cholesterol were significantly higher among systolic non-dipper when compared with systolic dipper patients with p-value 0.005.
In this work it was observed that the mean serum K was significantly higher among systolic non-dipper when compared with systolic dipper patients with p-value: 0.045. which do not agree with a study in adult patients that showed serum K was significantly higher among systolic dipper when compared to systolic non-dipper [27].
It was observed that the z score of IVS is significantly higher in hypertensive group. The elevated Z score in the hypertensive group could be indicative of early cardiac remodeling, a known complication of sustained hypertension [28].
There were significant positive correlations between the z score of IVS and SBP percentile for age (p: 0.045, r: 0.21) and DBP percentile for age (p: 0.043, r: 0.21). In current study, there is significant positive correlations were observed between the IVS z score and the albumin creatinine ratio (p: 0.028, r: 0.232). Proteinuria may be an important factor in the development of chronic inflammation in NS with subsequent myocardial involvement [29].
In our study, It was noticed that the Z score of IVS is significantly higher among systolic non-dipper (2.7 ± 1.0) when compared to systolic dipper (1.9 ± 1.6), among hypertensive group (group 1) with p-value 0.017. Patients without dipper patterns are more likely to experience end-organ damage in essential pediatric hypertension, LV hypertrophy, and early LV dysfunction. This is important since it can lead to unfavorable cardiac remodeling [29].
The study’s limitation was the requirement for a larger cohort of children and for follow-up on the children’s blood pressure, cardiac health, and nephrotic syndrome status, including whether there was activity or remission during the follow-up period. Additionally, the dosage of steroids given to the children will be correlated to these variables. We recommend further studies on Control of masked hypertension in children with nephrotic syndrome and its effects on IVS hypertrophy.
Finally, the present study examined the diagnostic accuracy of BMI, IVS z score, serum urea, and serum albumin to predict the occurrence of hypertension in pediatric nephrotic syndrome patients. The results suggested that serum urea has the highest sensitivity (92.9%) for predicting hypertension (AUC = 0.666), while BMI and IVS z score demonstrate moderate diagnostic accuracy (AUC = 0.626 and 0.638, respectively). In contrast, serum albumin shows limited utility in this prediction, as indicated by its lower AUC value (0.340). Overall, this study adds valuable evidence to the existing knowledge on pediatric nephrotic syndrome, particularly concerning the interrelationship between proteinuria, ambulatory blood pressure, and various demographic and clinical factors. The findings will help guide future research and clinical practice to characterize risk factors better, understand underlying mechanisms, formulate management strategies, and ultimately improve outcomes for this vulnerable patient population.








留言 (0)