Ethics approval and consent to participate
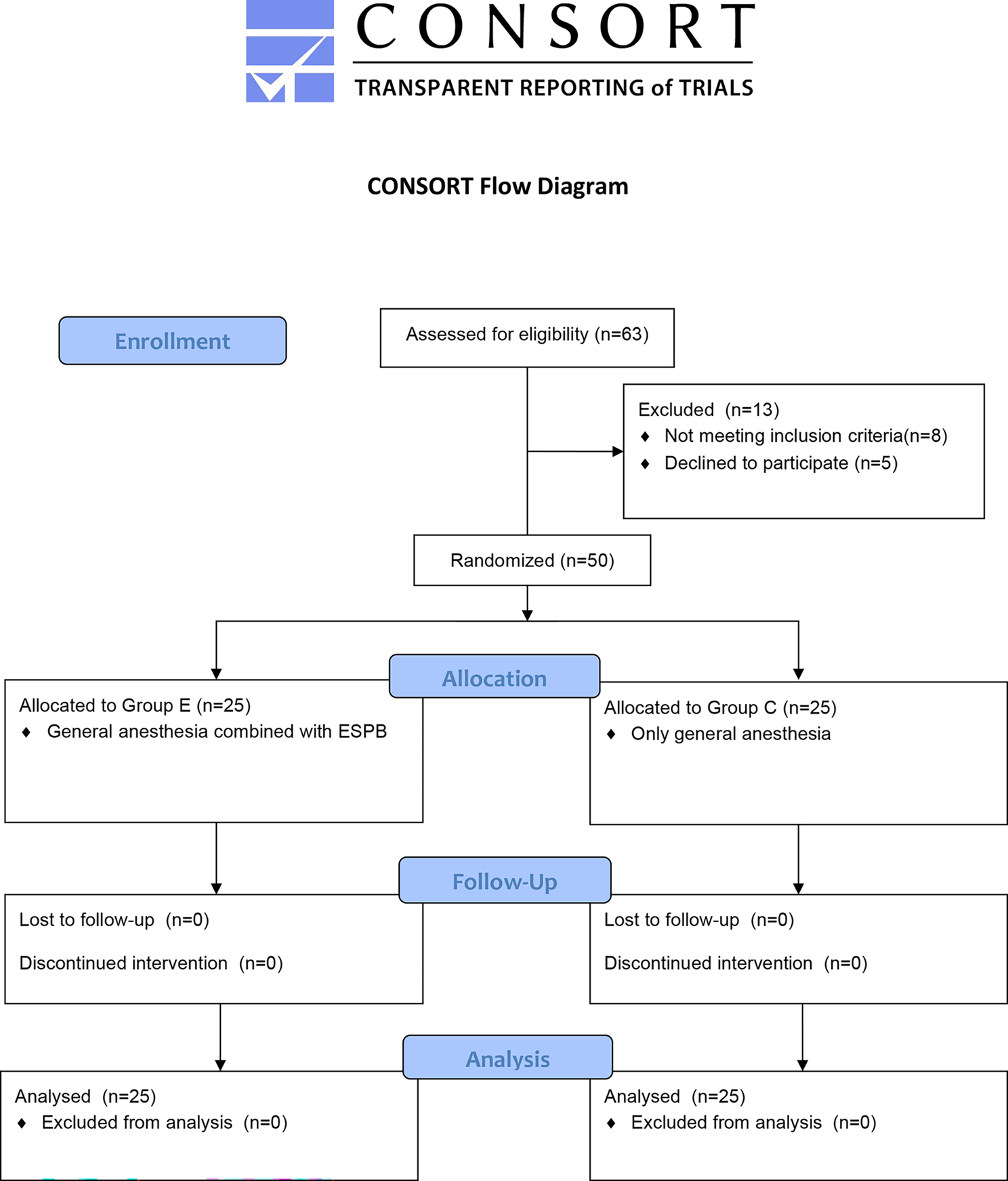
This prospective, randomized, controlled, double-blind trial was approved by the Ethical Committee of Women’s Hospital, Zhejiang University School of Medicine (Hangzhou, China) (No. IRB-20230261-R) and was registered at the Chinese Clinical Trials.gov (No. ChiCTR2400079888, date: 15/01/2024). This trial was conducted from Jan 15, 2024 to Apr 30, 2024 in Women’s Hospital Zhejiang University School of Medicine in Hangzhou. Written informed consent was obtained from all patients before enrollment. The principles of Declaration of Helsinki were followed for this study. This manuscript adheres to the applicable CONSORT guidelines.
Study population
Patients were eligible if they met the inclusion criteria: (1) scheduled to hysteroscopy requiring intravenous anesthesia; (2) American Society of Anesthesiologists (ASA) physical status I-II; (3) aged 20–45 years; (4) body mass index (BMI) 18–25 kg/m2. Patients were excluded if they had any of following conditions: (1) cardiopulmonary disease; (2) alcohol abuse, liver and kidney dysfunction; (3) chronic use of tranquillizers/opioids/antidepressants; (4) anesthetic drug allergy; (5) difficulty in cervical dilatation which was defined as the duration of cervical dilatation > 5 min; (6) obstructive sleep apnea-hypopnea syndrome (OSAHS); (7) participating in other clinical studies; (8) other reasons that are not appropriate for clinical study.
Randomization and blinding
The simple randomization was chosen in our trial which was performed using a computer-generated random numbers table to ensure that each group contained 125 subjects. Randomized results were sealed in sequentially numbered envelopes until the end of the study. Sealed and numbered envelopes were handed to an anesthesiologist who was not involved in this study performed the anesthesia procedure. A blinded investigator who was not directly involved in intraoperative anesthesia collected data. The surgeons and patients were all blinded to the grouping assignments.
Anesthesia and monitoring
The intramuscular injection of phloroglucinol (80 mg) was used for cervical ripening for each patient at 2 h before operation. All the patients had routine noninvasive monitoring of blood pressure (1 min cycle), electrocardiogram (ECG), and pulse oximetry (SpO2) in the operating room during the whole duration of hysteroscopy. In addition, end-tidal carbon dioxide monitoring measured respiratory rate (RR). Spectral entropy (SE) measured the depth of anesthesia by monitor (CARESCAPE Monitor B650, GE Healthcare, Helsinki, Finland). All patients inhaled oxygen (5 L/min) through a Venturi oxygen mask.
Patients were randomly assigned to receive either propofol (Group P, n = 125) or remimazolam-propofol combinations (Group RP, n = 125) at a 1:1 ratio. Intravenous injection of sufentanil 0.1ug/kg, dexamethasone 5 mg and palonosetron 0.25 mg were administered before sedative medication. In group P, a bolus of 2.5 mg/kg propofol (Aspen Pharma Co. LTD., Ireland) was administered. In group RP, intravenous anesthesia was commenced with 0.125 mg/kg remimazolam (Yichang Humanwell Pharmaceutical Co. LTD., China) and 1 mg/kg propofol. The concentrations of propofol and remimazolam were 10 mg/ml and 1.25 mg/ml respectively. The total volumes of induced drugs were 0.2 ml/kg in group RP and 0.25 ml/kg in group P. All drugs were injected by the speed of 600 ml/h. After loss of consciousness, propofol was maintained at 6 mg/kg/h. The surgeon was allowed to start cervical dilation when adequate sedation (SE < 60) was achieved. The cervix was dilated to 1 cm in diameter and hysteroscope with 27-Fr (9 mm) outer sheath was inserted. If patients did not achieve adequate sedation (SE > 60 or body movement), they were given top-up doses of propofol (0.5-1 mg/kg per time) and the top-up interval was more than 1 min. If SE was lower than 40, propofol was suspended till SE > 50. SE was maintained at 40–60 during the operation. After the procedure, patients were transferred to the recovery room. Visual analog scale (VAS) was used to assess pain after surgery. If VAS > 4, ketorolac 30 mg was administered intravenously.
Outcome measures
The primary outcomes were the incidence and amount of hypotension during surgery. Hypotension was defined as a mean arterial pressure (MAP) less than 65mmHg for at least 1 min [8, 9]. The amount of hypotension was assessed by time-weighted average intraoperative MAP (TWA MAP) under a threshold of 65 mmHg. The measure characterizes both the duration and severity of hypotension. TWA was measured by calculating the area under the threshold (AUT) divided by the total duration of hysteroscopy [10, 11]. The AUT was calculated as the sum of the products of the duration spent below the 65mmHg threshold and the difference between these measurements and the threshold. If MAP < 55mmHg, hypotension was treated by intravenous injection of norepinephrine.
The secondary outcomes were various anesthesia related parameters and some adverse events. The onset time was defined as the time from the end of sedation drugs injection to reach SE < 60. The operation time was defined as the time from the insertion of the speculum to the time of the hysteroscope removal. Recovery time was defined as the time from the stop of propofol injection to the time that the patient was awake and opened eyes. The adverse events include injection pain, low oxygen saturation, jaw thrust, bradycardia, hiccup, body movement, additional medication and vomiting. The injection pain was defined as patients verbally reported their pain by themselves after the first injection. Low oxygen saturation was defined as SpO2 < 95% which was treated with jaw thrust, mask ventilation, or endotracheal intubation. Jaw thrust was defined as maneuver against the patient’s jaw to prevent the jaw from slipping back and causing an airway obstruction. Bradycardia was defined as heart rate (HR) < 50 beats per minute which was treated by intravenous injection of atropine or norepinephrine. Hiccup was defined as involuntary contractions of the diaphragm and the auxiliary respiratory muscles, mostly in irregular series, followed by glottic closure, thereby producing a typical “hiccupping” inspiration. Body movement was defined as visible autonomous body movement during operation. Additional medication was defined as the top-up drugs to achieve adequate sedation after the initial dose of drugs. Induction was defined as the process from injection of sedation drugs to accomplish cervical dilation. Maintain was defined as the process from end of cervical dilation to finish operation.
Statistical analysis
Based on our preliminary study, the incidence of hypotension in intravenous anesthesia during day-surgery hysteroscopy was 5% in the remimazolam-propofol group and 20% in the propofol group. A sample size of 97 patients per group was required for 90% power with a 0.05 α. Taking into account the 20% loss rate, we needed to enroll 125 patients per group for a total of 250 patients.
Analyses were performed using IBM SPSS Statistics for Windows version 26. The Kolmogorov-Smirnov test was used to determine whether the continuous variables were normally distributed. The non-normally distributed variables were tested by two independent samples nonparametric test (the Mann-Whitney test) and expressed as the median (interquartile range). Enumeration data were presented as count (percentage). The chi-square test was used to compare categorical variables. We estimated the effect of TWA drop using the 2-sample Wilcoxon rank-sum test. This method was appropriate because the TWA drop < 65mmHg exhibits a skewed distribution with many patients having TWA drop of zero. We substituted zeros with small nonzero value for the modeling purposes. Values of P < 0.05 were considered statistically significant.









留言 (0)