
記住我






The study protocol (2014/1306–31/3) was approved by the Regional Ethics Committee of Stockholm, Sweden. We adhered to the Strengthening of the reporting of observational studies in epidemiology (STROBE) and a checklist can be found in the “Appendices” section.
This observational, registry-based cohort study prospectively collected data from 23 Swedish hospitals. The study population was identified from university-, county- and district hospitals of all levels in Sweden between 2007 and 2014 using the Orbit surgical planning system software, which at the time of the data collection covered approximately 40% of the Swedish population. The Orbit system includes Swedish identity number, patient demographics, American Society of Anaesthesiologists (ASA) physical status classification, date, and duration of anesthesia and surgery.
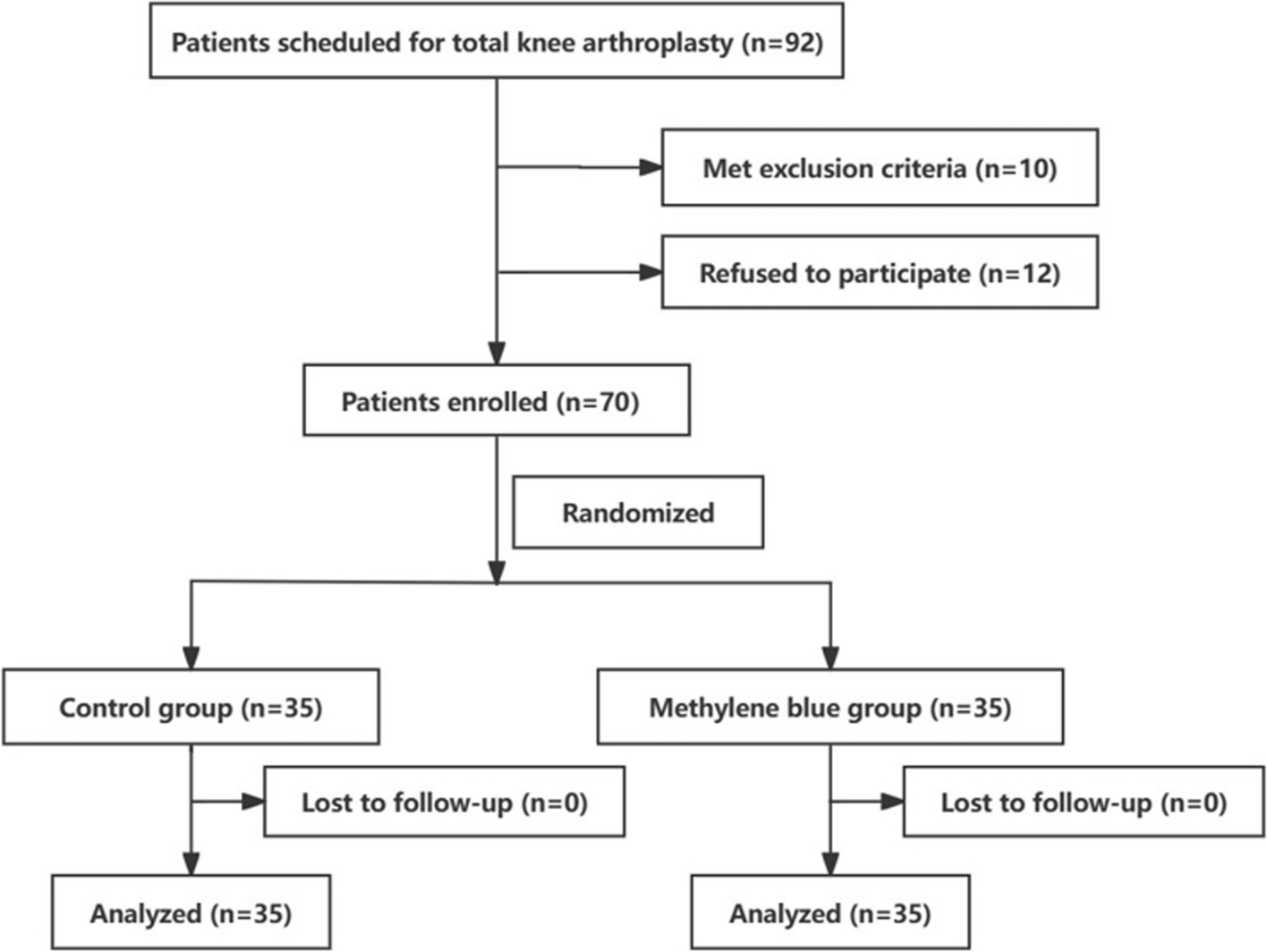
The study cohort included patients ≥ 18 years old who underwent surgery between the 1st of January 2007, and the 31st of December 2014. Exclusions: cardiac, obstetric, ambulatory, minor, or multiple surgeries and those lacking a valid surgery code in Orbit or a corresponding surgery code in the National Patient Register (NPR) (see data sources below). Furthermore, we excluded patients identified from hospitals with a high proportion of missing ASA physical status classification. Figure 1 provides a CONSORT flowchart.
Fig. 1
Stroke was defined as all participants with International Statistical Classification of Diseases Code (ICD-code) I63 up to 5 years prior to surgery. In a sensitivity analysis, we defined stroke as ICD-code I63 up to 1 year prior to surgery.
To acquire information on discharge dates, covariates, and drug exposure, surgical records were linked to the National Patient Register (NPR) and the Swedish Prescribed Drug Register (SPDR) using the personal identification number assigned to all residents at birth or immigration. Furthermore, the data was linked to the Swedish Cause of Death Register.
Data sourcesOrbitOrbit is an operational planning system, where all patients undergoing surgery are documented (Care 2023). The Orbit database includes pre-, intra-, and postoperative data.
The national patient registerNPR provides statistics on diseases and treatments in Swedish specialized healthcare, covering all in-patient care since 1987 (Socialstyrelsen. 2018a). The NPR comprises personal, geographic, administrative, and medical data, including ICD codes. The registry is obligatory for all Swedish county councils (Socialstyrelsen. 2018a).
The Swedish prescribed drug registerThe Swedish Prescribed Drug Register (SPDR) provides the basis for the official statistics on pharmaceuticals in Sweden (Socialstyrelsen. 2018b). The register, linked with social security numbers, was initiated in July 2005 and includes all prescription drugs dispensed at pharmacies (Socialstyrelsen. 2018b). The SPDR also consists of information about the patient (such as sex and age), the drug (such as ATC code, dosage, and price) as well as information about the drug prescriber and the workplace where the prescription was made (Socialstyrelsen. 2018b).
Swedish cause of death registerThe Swedish Cause of Death register is a complete register of all deaths in Sweden since 1952 (Brooke et al. 2017).
Outcome measuresPrimary outcomeOur primary outcome was 1-year-mortality in patients with preoperative stroke up to 5 years prior to the operation.
Secondary outcomeOur secondary outcome was DAH30 in patients with preoperative stroke up to 5 years prior to the operation. This comprehensive outcome includes length of stay (LOS) and readmissions, as well as mortality within 30 days after surgery.
Calculating DAH30DAH30 was calculated as previously described in detail (Bell et al. 2019; Myles et al. 2017), using the date of index surgery (day 0) with hospitalization and mortality data up to day 30. Hospital—to home—discharge dates were used to calculate hospital length of stay (ignoring preoperative in-hospital days, and taking into account discharge to nursing homes or other hospitals). Death in hospital or after discharge within the first 30 days after surgery, equals 0 DAH30. If a patient was discharged from the hospital on day 13 after surgery but readmitted for 7 days before their second hospital discharge, then the patient would be assigned 10 DAH30.
Statistical methodsData were analyzed using RStudio (Team RC. R n.d.). Categorical data were presented as numbers and percentages, while continuous data were presented as means and standard deviations. P values < 0.05 were interpreted as statistically significant. Descriptive statistics were presented by p values using Pearson’s chi-squared test for binary categorical variables and an unpaired two-sample t-test for continuous variables.
To evaluate the primary and secondary outcomes, multiple logistic regression analyses were used. Separate analyses were performed for ASA class and ICD-codes, each one as a proxy for comorbidity, to minimize the risk for collinearity. We adjusted for age, sex, and type of surgery. As mentioned above, a sensitivity analysis was performed among patients with more recent diagnosis of stroke.
DAH30 was dichotomized into 1 = DAH ≤ 15, and 0 = DAH > 15. A DAH30 less than 15, indicates death and/or complications. This cut-off allows us to calculate adjusted odds ratios (ORs) for preoperative stroke; both for mortality at 365 days and for having a DAH30 less than 15.
留言 (0)