
記住我
This study was a random controlled clinical trial, with a split-mouth design, performed in the pediatric dentistry department, Mansoura University, Egypt. It was conducted at the period from Sep 2020 to Dec 2022.
This study was ethically approved by the Faculty of Dentistry, Mansoura University (A05031219). The study was simply explained to the parent and the benefit for the children was pointed out and parent /child consent and assent were obtained before starting the treatment. The study protocol was registered on Clinical Trials (NCT05931822–3rd of July 2023).
Sample size was calculated by using Power Analysis and Sample Size (PASS) Software (2017). NCSS, LLC. Kaysville, Utah, USA. A factorial design with two factors (factor A is moderate and severe grades, and factor B is the SDF vs. Varnish) at 2 and 2 levels, respectively, has 4 cells to test their effects on restoration integrity. A total of 56 teeth are required to provide 14 teeth per cell. This design achieves 84% power when an F test is used to test factor A at a 5% significance level and the effect size is 0.400, achieves 84% power when an F test is used to test factor B at a 5% significance level and the effect size is 0.400, and achieves 84% power when an F test is used to test the A*B interaction at a 5% significance level and the effect size is 0.400 [14, 15].
Diagnosing, training and calibrationBefore starting the study, the examiner was thoroughly calibrated by using the EAPD scale under an expert supervision. Thirty pictures were used with different severities until a suitable intra-examiner reliability was attained through discussions and practical exercises. Molars which were presented with opacities and post eruptive breakdown restricted to the enamel, were judged to be moderate MIH. While, teeth erupted with breakdown involving dentin, were judged to be severe MIH [16].
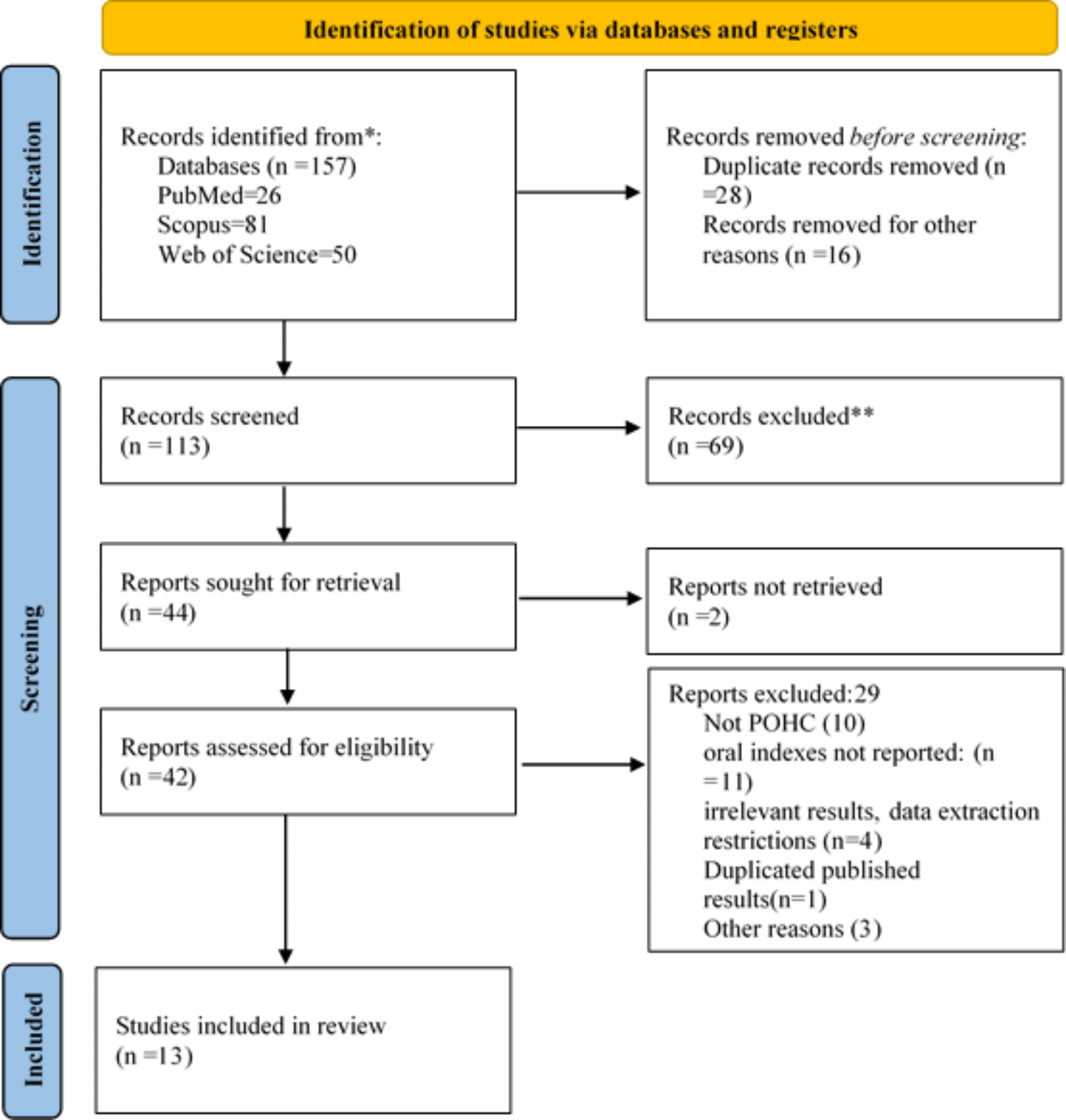
Study designThe study was conducted on 56 molars for 28 children (20 girls and 8 boys) with at least 2 hypomineralized molars with the same defect severity. The study comprised 2 groups; MOD group (moderate hypomineralized molars) and SEV group (severe hypomineralized molars) (n = 28 each). Each group was further subdivided into 2 subgroups; SMART subgroup 1 and conventional-HVGIR (CONV) subgroup 2 (n = 14 each) according to the technique of restoration. All children were successfully followed for 12 months with no complications as shown in Fig. 1.
Fig. 1
Flow diagram of participants up to 1 year
Setting and participantsAfter examining 80 children diagnosed as having hypo mineralized first permanent molars, 28 children met the following inclusion criteria:
Children aged 6–10 years with moderate or severe hypomineralized first permanent molars.
Presence of bilateral first permanent molars with the same degree of hypomineralization severity and ICDAS-II score (international caries detection and assessment system) [17] ranging from 3 to 5 for the MOD and SEV groups.
Molars should be free of any symptoms and signs of irreversible pulpitis or pulp necrosis.
Children should be free from any systemic diseases.
The rest of the children were excluded from the study due to having pulpal symptoms or lacking cooperation but were treated as indicated.
Children were examined clinically in a dental chair under the light source of the dental unit, using a dental oral mirror (No. 4). Teeth were cleaned before examination under wet conditions to better visualization. the modified European Academy of Pediatric Dentistry criterion was followed for defining MIH [18, 19].
Randomization and blinding methodsSimple randomization was carried out through two principals: the restorative technique (SMART/CONV) and the site of the molar (left/right). To select the restoration and the tooth to be treated, each qualified child drew twice from four opaque envelopes. The first draw decided the restoration to be applied, while the second determined the site [20].
Materials and clinical proceduresA split mouth design was performed for all groups, and each molar on either side was restored in a separate visit and local anesthesia was administered as needed. After that, hypomineralized enamel at the margins of the cavity was selectively removed using a high-speed, water- cooled diamond fissure burs. While at the enamel-dentin junction, a sharp sterile spoon double-ended excavator was used until hard and dry dentin remained with clean enamel margins. low-speed smart burs (SAMARTBURS II, RA-8) were used to remove the remaining caries in the depth of the cavity (pulpoaxial walls). Finally, dentine hardness was checked using a dental probe.
In subgroup 1, after caries removal, SDF (FAgamin 38%; Tedquim, Argentina) was applied in the cavity for 1 min then blot dried and the cavity was sealed with temporary filling. In the next visit after one-week, the temporary filling was removed and acidic conditioner was applied in the cavity for 10 s, washed with air water spray then dried with cotton pellets. Afterwards, the tooth was restored with HVGIR (Equia Forte HT; GC, Tokyo, Japan) following the instructions manual then covered by Vaseline. After setting time (2.5 min), the occlusion was checked with an articulating paper then adjusted.
In subgroup 2, caries was removed with the same technique, then the cavity was conditioned for 10 s then washed and dried with cotton pellets and restored by HVGIR. Finally, fluoride varnish (MI varnish; GC, Tokyo, Japan) was applied to all teeth of the child. Instructions were given to the children not to eat or drink for at least 1 h.
MI paste plus (MI paste plus; GC, Tokyo, Japan) was given to the children to use daily at night as tooth paste before going to sleep without rinsing. Oral hygiene measures instructions were illustrated to the parents/caretakers and children, with the use of auxiliary aids. Also, the brushing technique was demonstrated using toy models. Children were recalled every three months for fluoride varnish application on all teeth for one year.
EvaluationAll children were evaluated for restoration and tooth integrity, hypersensitivity and occlusal surface area change.
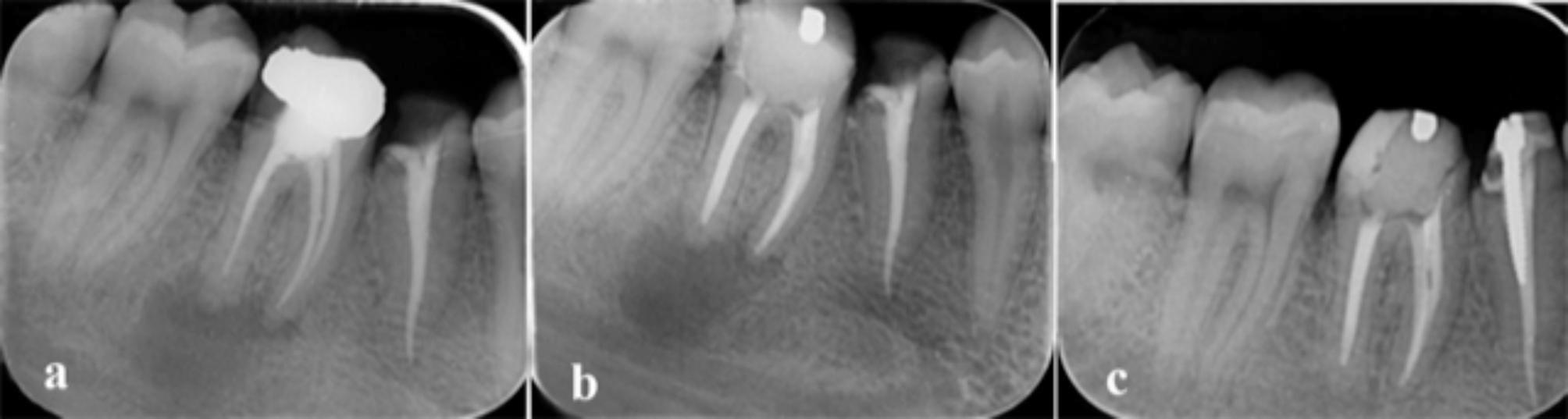
The examiner did the evaluation after high reliable scores for restoration and tooth integrity. The standard ART criterion [21] was used for the evaluation, with codes from 0 to 9, in which 0, 1 and 7 are considered successful and rated “survived” while other scores rated as “failed to survive”. Photographs were taken postoperatively, at 6 months (T1) and at 12 months (T2) as shown in Figs. 2 and 3.
Fig. 2
Severely affected first permanent molars treated with SMART (left) and conventional restoration (right) through one year (a: preintervention, b: postintervention, c: 12 months)
Fig. 3
Moderately affected first permanent molars treated with SDF (left) and conventional restoration (right) through one year (a: preintervention, b: postintervention, c: 12 months)
The Schiff Cold Air Sensitivity Scale (SCASS) was used to assess the molars hypersensitivity to air (0 = no response to the air; 1 = no response to the air, patient felt pain; 2 = response to air, patient moves away from air stimulus; 3 = response to the air, patient moves away from air stimulus and requests immediate discontinuation of the stimulus) [22].
Air was blown in a perpendicular position on the occlusal surface of the tooth using air syringe at a distance of 1 cm and if neighboring teeth were found, cotton rolls were used to cover them. Hypersensitive molars had a positive response to air stimulus when applied for 1 s, with a score of 2 or 3 [22].
For occlusal surface area change, two impressions were taken for the two groups and scanned at baseline and after 12 months. One step technique Impressions were taken for all groups twice, using additional silicone rubber base (Elite HD + putty soft and light, Zhermack, Italy), once immediately after restoring both molars then one-year after. Impressions were poured and casts were obtained for scanning using intraoral scanner (Medit i700) and analyzing the scans using Medit link 3.1.1 software program.
A 3-dimensional (3D) comparison was achieved by aligning the two scans for each impression by best fit alignment. A 3D comparison provides a heatmap with a spectrum of colors to show the differences between both scans, where the postoperative scan was selected as reference and the 12 months scan as test. The blue colour indicated the decrease in the vertical dimension and the red colour indicated an increase in the vertical dimension. A standard “best-fit alignment” uses an iterative closest point algorithm to align both scans that do not involve operator-based decisions [23, 24].
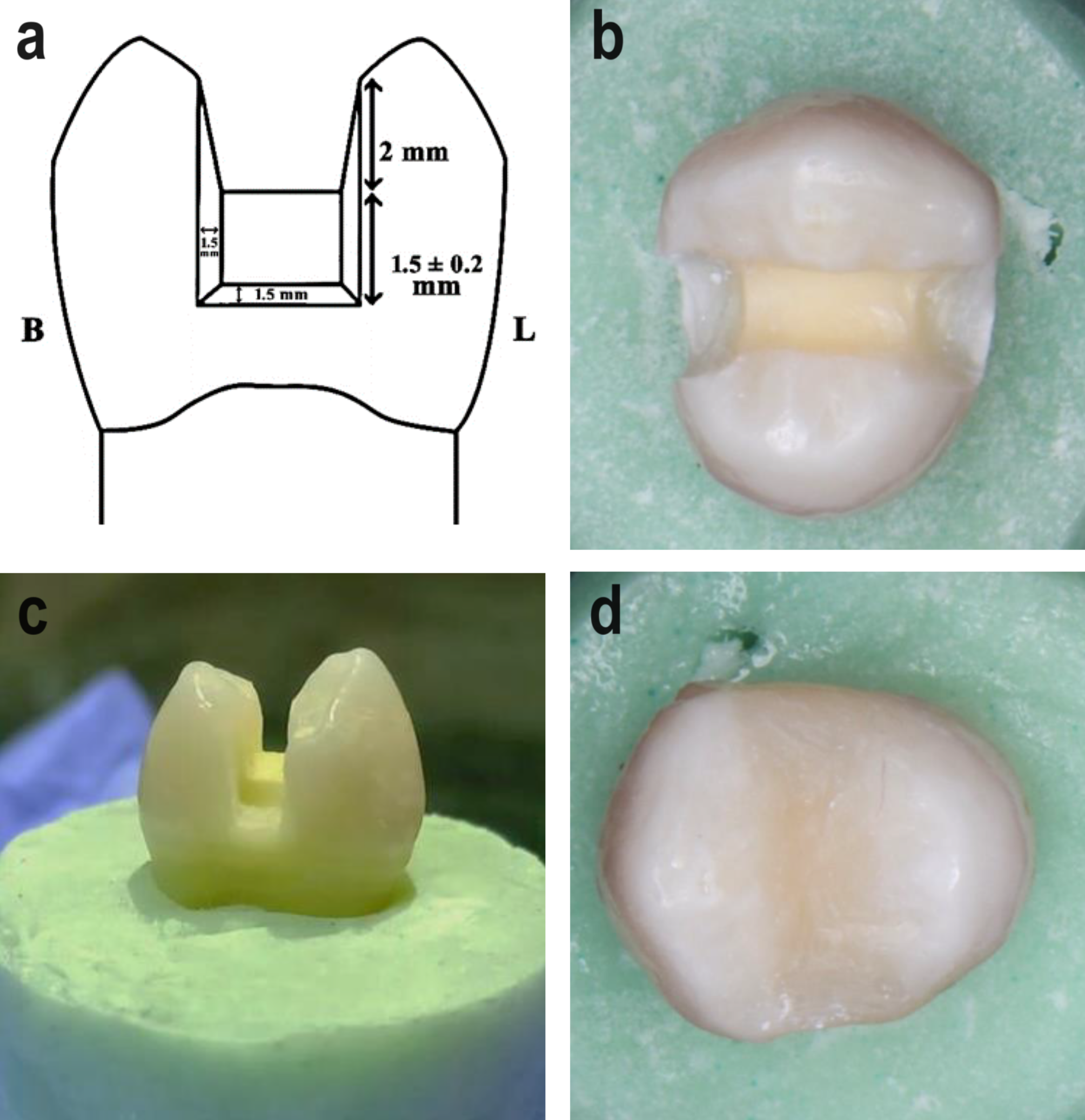
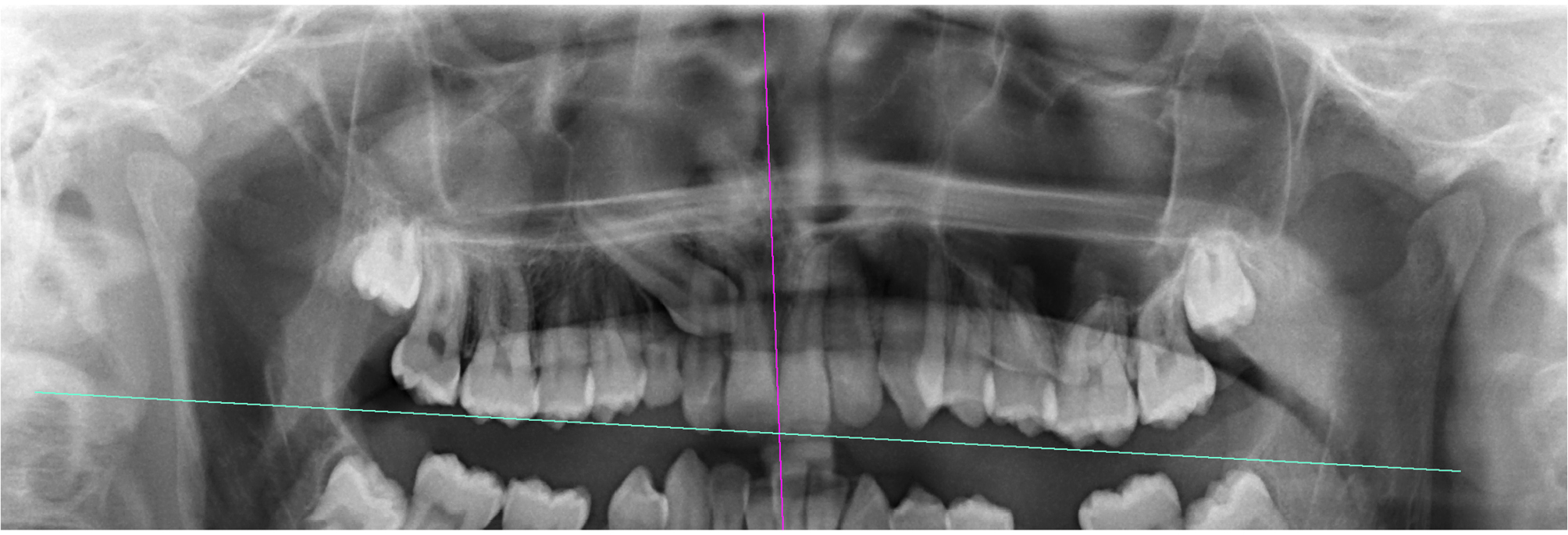
The best fit alignment was done by creating a new modified reference area and the quality of the best fit was double checked using a 3D comparison. Quantitative measurements were obtained using the reference points for each first molar; mesiobuccal and distobuccal cusp tip, distal cusp tip, mesiolingual and distolingual cusp tip, central pit, mesial and distal marginal ridge as in Fig. 4.
Fig. 4
Heat map for different severities of MIH molars after matching both scans (postintervention and after one year) a: MOD/ SMART, b: SEV/CONV
Statistical analysisIBM/SPSS software (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp) was used to evaluate the data. Qualitative data were expressed as N (%) and Quantitative data were initially tested for normality using Shapiro-Wilk’s test with distributing the data normally if p > .050. Significant extreme values were tested by reviewing boxplots. Quantitative data were expressed as median and range (minimum – maximum).
Comparing the pre-post data was done using the Wilcoxon signed rank test as the difference was not normally distributed with ± significant outliers. While the non-normally distributed repeatedly measured quantitative data were compared using Friedman’s test. As for statistically significant difference, pairwise comparisons with Bonferroni correction for multiple tests were performed. The Kruskal-Wallis H-test was used to compare non-normally distributed quantitative data between groups. For statistically significant difference, pairwise comparisons with Bonferroni correction for multiple tests were performed. Results were considered as statistically significant if P ≤ .050 for all of the used tests. The results were graphically presented using proper charts whenever needed.
留言 (0)