At present, surgery is still the first choice of treatment for differentiated thyroid cancer. The prognosis of differentiated thyroid carcinoma is good, but tracheal invasion is considered to be one of the important reasons affecting the prognosis of THCA [20]. Complete resection of THCA and invaded tissues can improve the survival rate of patients. Therefore, one-stage surgery for thyroid cancer invading the trachea has been approved to remove the involved organs simultaneously [11, 21]. For THCA with trachea invasion, whether tracheal reconstruction can be completed in one stage after the involved trachea resection is the most important technical issue of surgery. Especially for deep or full-thickness tracheal lesions, adequate tracheal resection and one-stage reconstruction can improve the survival rate and quality of life of patients. The most common reconstruction methods after tracheal resection are end-to-end anastomosis repair and tissue flap repair and so on. End-to-end anastomosis repair after tracheal sleeve resection has been recognized to help preserve the tracheal function of patients. Tracheal window resection can be used if the tumor invading from the lateral or anterior wall of the trachea does not exceed 50% of the circumferential, and the tracheal ring invading does not exceed 4 rings. After tracheal window resection, sternocleidomastoid muscle, banded myohyoid bone flap, clavicular membrane flap, pectoralis major myocutaneous flap or supraclavicular island flap can be used for repair [22, 23]. If the tumor invasion is more than 50% of the circumferential, then tracheal sleeve resection and end-to-end anastomosis can be performed. The sleeve resection trachea is generally 4 to 5 rings, and the longest can be 6 to 7 rings. In clinical practice, it may be encountered that the tracheal defect is close to 50%, and the tracheal ring defect is more than 5 rings. In such cases, tissue flap repair after window resection may cause postoperative airway collapse, while end-to-end anastomosis after sleeve resection may cause ischemic rupture of the anastomosis due to excessive tension [24, 25]. In this study, we analyzed the application of modified spiral tracheoplasty in the repair of large scale tracheal defects. Modified spiral tracheoplasty not only reduced the tension of the anastomosis, but also had no obvious airway collapse and stenosis after operation.
According to the Shin [26] classification, the depth of tracheal involvement can be divided into 5 grades. Grade 0: tumor confined to the thyroid gland. Grade I: the tumor had penetrated the thyroid capsule adjacent to but not invaded the tracheal cartilage. Grade II: tracheal cartilage destruction caused by tumor invasion; Grade III: the tumor invaded the tracheal lumen but the tracheal intima was intact. Grade IV: The tumor penetrates the full thickness of the tracheal wall. Tumor shaving can be considered for grade I and some grade II cases, while most grade II, III and IV cases must undergo involved trachea resection, including window resection and sleeve resection. In the cases included in this study, the tumors invaded the tracheal lumen and the depth of tracheal involvement was grade IV, so we chose to perform a total resection of the involved trachea. In addition to the depth of involvement, the width at the circumference of the defect also determines the method of tracheal resection. When the defect exceeds 50% of the circumference, the window defect is difficult to repair, and sleeve resection and end-to-end anastomosis are often required. In our case, the defect accounted for 40–60% of the circumferential area, and the risk of tracheal stenosis was high for simple window resection repair, but the end-to-end anastomosis was limited by the length of the defect. According to our experience, the length of the defect can be sutured directly within 4 cm, but if the length of the defect is too long, the tension of the anastomosis can be reduced by separating the lower trachea and the upper laryngeal body. All patients included in this study had a defect length of more than 5 cm, and the longest was 7.5 cm. Simple end-to-end anastomosis required the dissection of the upper larynx and the lower trachea. The risk of recurrent laryngeal nerve injury is increased during dissection. In 2009, Wu [17] reported a case of spiral tracheoplasty for repair after resection of window tracheal wall. Spiral tracheoplasty is to transection the remaining healthy trachea, rotate the upper and lower ends by 90 degrees in the opposite direction (one clockwise and the other counterclockwise), and perform preliminary anastomosis to reduce anastomotic tension. The subsequent reports on this technique were all case reports. Otsuki [27] reported two cases of reconstruction of large tracheal defects by modified spiral tracheoplasty. On the basis of Wu’s spiral tracheoplasty, he separated the trachea and esophagus by 2 cm, and only rotated the lower trachea by 90 degrees to reconstruct. Inspired by this technique, we performed repair after extensive tracheal defects by further improving spiral tracheoplasty. The residual trachea on the healthy side was transected in the middle, separated from the posterior esophagus, and designed as a tracheal valve. The upper and lower ends were twisted about 90° in the opposite direction and anastomosed up and down. This method can reduce the distance between the upper and lower trachea and reduce the tension of the anastomosis. Due to the elastic action of the tracheal wall, the lumen formed by the upper and lower tracheal valves has a rebound force to the original position when it is twisted. Under the action of the rebound force, the lumen is easy to expand, so tracheal stenosis almost does not occur. Moreover, because the trachea and esophagus are separated to a certain extent, the lower trachea can be twisted about 180° and anastomosed with the affected thyroid cartilage in the case of cricoid cartilage invasion. In the cases included in this study, we used simple modified spiral tracheoplasty without dissection of the laryngeal body. Combined with the results of endoscopy and airway CT after operation, no airway stenosis occurred in all cases. In conclusion, we conclude that modified spiral tracheoplasty is suitable for reconstruction of defects with 6 to 8 tracheal rings of length and 40–60% of the width of the tracheal lumen.
We summarized the details of the operation based on the analysis of 15 cases of large tracheal defects repaired by modified spiral tracheoplasty. (1) When making a tracheal flap by transection of the residual trachea on the healthy side, it is necessary to separate the esophagus and trachea properly to reduce the tension caused by esophageal traction during tracheal torsion; (2) In cases where the cricoid cartilage is invaded by THCA, tracheal torsion can also repair the partial loss of the cricoid cartilage. In this study, 3 cases invaded the cricoid cartilage and underwent partial resection of the cricoid cartilage. During reconstruction, the cartilage part of the lower tracheal valve was sutured with the lower edge of the thyroid cartilage. However, it is difficult to preserve the recurrent laryngeal nerve during the resection of the affected cricoid cartilage. In this study, 3 cases were found to have the invasion of the recurrent laryngeal nerve into the larynx during the operation, and both were resected. (3) Due to the total thyroidectomy in these cases, the tracheal anastomosis lacks tissue reinforcement, so we generally use the strap muscle to wrap the anastomosis to strengthen and increase blood supply. (4) The choice of tracheotomy. Preventive tracheotomy is recommended for predicting recurrent laryngeal nerve involvement during operation. One patient in this study underwent tracheotomy during resection of thyroid cancer. The main reason was that the patient had undergone unilateral thyroidectomy and had developed vocal cord immobilization. In this case, the tumor invaded the cricoid cartilage, and the recurrent laryngeal nerve was found to be involved during the operation, which was resected at the same time. Postoperative bilateral vocal cord paralysis could already be predicted during the operation, so tracheotomy was chosen during the operation. One patient was extubated 72 h after surgery and developed obvious laryngeal obstruction, so tracheotomy was performed after re-intubation. The patient was re-evaluated as having unilateral vocal cord paralysis with laryngeal cavity edema. The tracheal cannula was extubated 1 month later.
Recurrent laryngeal nerve injury is the main complication after modified spiral tracheoplasty. The recurrent laryngeal nerve is easily injured when making the tracheal flap and performing the tracheoesophageal separation. Therefore, the recurrent laryngeal should be fully dissociated and protected during the whole operation. In this study, recurrent laryngeal nerve palsy occurred in three patients after surgery. In addition, there is the possibility of rupture and stenosis of the tracheal anastomosis in both window-based tracheal resection and end-to-end tracheal anastomosis, which is related to the large scope of window-based resection and the excessive tension of the anastomosis [28, 29]. There was no tracheal anastomotic rupture and stenosis after operation.
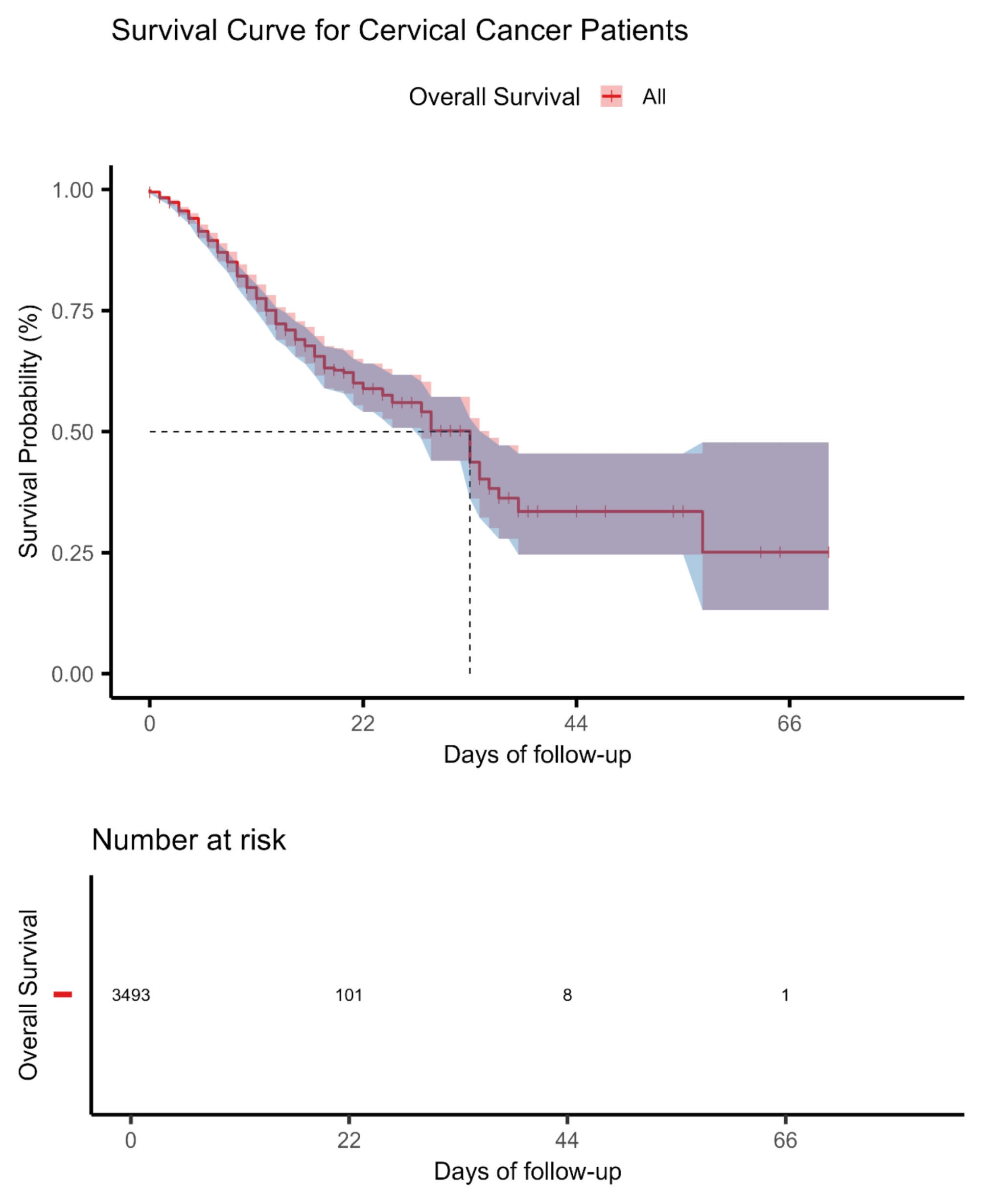
The oncologic outcome of patients with THCA who use modified spiral tracheoplasty to repair the defective trachea is also of concern. Ebihara [27] et al. conducted a retrospective analysis of 41 patients with THCA invading deep trachea after window resection. The 5-year and 10-year survival rates were 78.9% and 74.5%, respectively, and the 5-year and 10-year local control rates of tumor and invaded trachea were 92.4% and 73.4%, which fully confirmed the therapeutic effect of window resection. For THCA involving the cervical trachea, the 3-year and 5-year survival rates of tracheal sleeve resection and end-to-end anastomosis were 93.8% and 70.3% respectively. In this study, the follow-up time was from 24 to 60 months. The 2-year survival rate was 100%, the 2-year tracheal local control rate was 100%, and the 2-year tumor-free survival rate was 81.8%. The survival rate and local control rate were similar to those reported in the literature. For THCA with tracheal involvement, iodine 131 has a role in the diagnosis and treatment, which is beneficial to the control of local recurrence and distant metastasis. All 11 cases in this study had complete tumor resection, and all patients were treated with iodine-131. One patient received a second iodine-131 therapy and targeted therapy because of lung metastasis at 17 months after surgery.




留言 (0)