
記住我







Retrospective case series.
Ethics approvalThe research adhered to the tenets set forth in the Declaration of Helsinki and was approved by our local ethics committee (CE 2023/157). Written informed consent for publication was obtained from both patients.
Case descriptionsCase 1An 18-year-old man complained of visual field defects, mostly at nighttime, that started during childhood. There was no notable general or family history. He was of Moroccan ethnicity, and was not taking any medication.
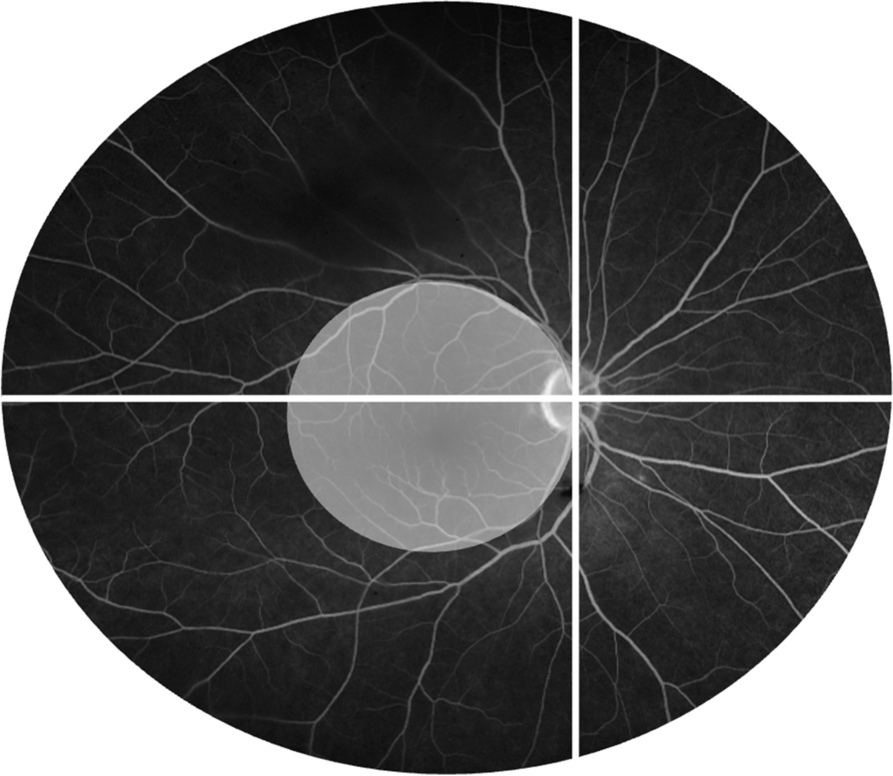
On examination, best-corrected visual acuity (BCVA) was 20/32 in both eyes (OU). Slit-lamp examination (SLE) was normal except for 1 + anterior vitreous cells. Fundoscopy showed vascular attenuation and mid-peripheral outer retinal atrophy (ORA) (Fig. 1, A – B). There were no intraretinal pigment migrations (IPMs). Macular spectral-domain optical coherence tomography (SD-OCT) showed CME and perifoveal ORA (Fig. 1, C – D). Fluorescein angiography (FA) demonstrated peripapillary leakage and CME (Fig. 1, E – F). Humphrey 24 − 2 visual fields (HVF) showed pericentral sensitivity loss. Full-field electroretinogram (ffERG) was uninterpretable because of contact lens electrode aversion.
Posterior uveitis (PU) in the form of peripapillary retinal capillaritis was suspected and a targeted uveitis work-up (syphilis, tuberculosis, sarcoidosis, Birdshot retinochoroiditis [BRC]) was negative. Owing to perifoveal ORA, RP masquerading as PU was then suspected and an inherited retinal disease (IRD) gene panel was ordered.
Treatment for waxing and waning CME was initiated with partial and inconsistent response. This included topical diclofenac sodium 0.1% bid, topical brinzolamide 1% tid, oral methylprednisolone, oral methotrexate (MTX), anti-VEGF intravitreal injections (IVT), MTX IVT, dexamethasone implant (DEX) IVT, and intravenous (IV) infliximab, before obtaining CME and RVL control using IV TCZ 8 mg/kg every 4 weeks (Fig. 1, G – J). It took approximately 2 to 3 weeks to obtain CME and RVL control with TCZ.
Ultimately, a homozygous pathogenic variant in the EYS gene was found and a diagnosis of EYS-related autosomal recessive RP was made. Scarce peripheral IPMs had appeared over the follow-up.
Comprehensive explanations were given to the patient concerning the genetic nature of the disease, and the absence of a specific treatment. However, considering the obvious benefit of TCZ on the inflammatory component of the disease, the patient opted to pursue treatment.
At the last follow-up, macular SD-OCT remained dry under IV TCZ 8 mg/kg every 8 weeks. Final BCVA was 20/25 OU. Total follow-up was 129 months, of which 103 were under treatment with TCZ.
Case 2A 61-year-old woman presented with nyctalopia, difficulty stumbling over things, and photopsia for the past year. She was of Chinese ethnicity, and had a history of cysticercosis for which she had been inconsistently self-medicating with praziquantel.
On examination, BCVA was 20/30 in the right eye, and 20/25 in the left. SLE was normal. Fundus examination revealed subtle mid-peripheral ORA, and mild vascular attenuation (Fig. 1, M – N). Macular SD-OCT showed symmetrical perifoveal ORA, and CME (Fig. 1, O – P). FA revealed intense vascular leakage from the optic disc, veins, capillaries, and fovea (Fig. 1, Q – R). HVF showed concentric defects. ffERG revealed rod-cone dysfunction (RCD). Overall, findings were felt to be compatible with RP and an IRD gene panel was ordered.
However, owing to intense CME and RVL, a targeted uveitis (syphilis, tuberculosis, sarcoidosis, BRC, cysticercosis) work-up was performed, which was negative, and treatment with topical prednisolone acetate 1% tid, topical ketorolac trometamol 0.5% tid, and 0.8 mg/kg oral methylprednisolone was initiated. This treatment yielded no benefit after 1 month and was discontinued.
Over the ensuing months, BCVA dropped further to 20/50 in the right eye, and 20/32 in the left. Gene panel results showed a heterozygous pathogenic variant in the KCNV2 gene, and a variant of unknown significance in the TSPAN12 gene. These findings did not help establish a molecular diagnosis of RP. Scarce perivascular IPMs had appeared in the retinal periphery. Given the absence of RVL and CME improvement with corticosteroids, alongside compatible ancillary examination findings, a formal clinical diagnosis of RP was made.
The dual nature of the disease was explained to the patient (RP with inflammatory features, or possible associated non-infectious PU), and she agreed to a stepladder immunosuppressive approach.
Treatment for CME and RVL was then initiated with inconsistent responses. This included topical brinzolamide 1% tid, topical ketorolac trometamol 0.5% tid, oral methylprednisolone, oral MTX, DEX IVT, and subcutaneous adalimumab, before ultimately obtaining CME and RVL control using IV TCZ 8 mg/kg every 4 weeks (Fig. 1, S – V). It took approximately 2 to 3 weeks to obtain CME and RVL control with TCZ.
At the last follow-up, macular SD-OCT remained dry under IV TCZ 8 mg/kg every 4 weeks. Final BCVA was 20/32 in the right eye, and 20/40 in the left. Total follow-up was 63 months, of which 19 were under treatment with TCZ.
Fig. 1
Retinal findings before and after treatment with intravenous tocilizumab in patients 1 and 2. Patient 1, EYS-related autosomal recessive retinitis pigmentosa – A, Fundoscopy of the right eye showing mild disc hyperemia, cellophane maculopathy, vascular attenuation, and mid-peripheral outer retinal atrophy (ORA). B, Fundoscopy of the left eye showing similar findings except for mild temporal disc pallor. C – D, Before treatment with intravenous tocilizumab (IV TCZ), macular spectral-domain optical coherence tomography (SD-OCT) shows an epiretinal membrane, cystic changes in the outer (ONL) and inner nuclear layers (INL), some very large at the level of the fovea, and perifoveal ORA in both eyes. E – F, Before treatment with IV TCZ, fluorescein angiogram (FA) shows intense peripapillary retinal capillaritis, foveal leakage, and patchy hyperfluorescent defects over the posterior pole and beyond the vascular arcades in both eyes. G – H, Macular SD-OCT showing perifoveal ORA, and complete resolution of the cystic changes in both eyes after treatment with IV TCZ. I – J, FA shows generalized patchy window defects over the posterior pole and beyond the vascular arcades, and mild capillary leakage along the proximal temporal vascular arcades in both eyes. Note the substantial reduction in vascular leakage after treatment with IV TCZ when compared with pre-treatment images. K – L, Blue light autofluorescence (BAF) shows a perifoveal hyperautofluorescent ring and patchy mid-peripheral hypoautofluorescence in both eyes. Patient 2, RP without molecular explanation–M – N, Fundoscopy showing mild optic disc hyperemia, blunted foveal reflex, subtle mid-peripheral ORA and mild vascular attenuation in both eyes. O – P, Before treatment with IV TCZ, macular SD-OCT shows an epiretinal membrane, cystic changes predominantly in the INL, and perifoveal ORA in both eyes. Q – R, Before treatment with IV TCZ, FA shows severe multifocal leakage from the optic disc, fovea, capillaries, and veins in both eyes. S – T, Macular SD-OCT showing perifoveal ORA, and dramatic reduction of the cystic changes in both eyes after treatment with IV TCZ. U – V, After treatment with IV TCZ, FA shows patchy mid-peripheral window defects extending beyond the vascular arcades in both eyes. Some newly occurring hypofluorescent lesions secondary to intraretinal pigment migrations are visible in the temporal mid-periphery. Note the dramatic reduction in vascular leakage after treatment with IV TCZ when compared with pre-treatment images. W – X, BAF shows central hypoautofluorescence surrounded by a discrete perifoveal hyperautofluorescent ring in both eyes
留言 (0)