AppendixMethodsSearch strategy and study selection criteria
A systematic search of the existing world literature employing the NCBI Medical Subject Heading (MeSH) term “pilonid*,” further to a combination of “dermoid” AND “cyst,” was conducted across all databases available, including MEDLINE, PubMed, PubMed Central, Scopus, Ovid, EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL). In addition, a search using these terms in Google, Google Scholar, and ResearchGate was conducted. Furthermore, references cited in national and international guidelines, such as the S3 guidelines of the Association of the Scientific Medical Societies in Germany pertaining to pilonidal sinus disease (PSD) treatment, were scrutinized. We also examined the references included in the bibliographies of all documents obtained through these searches. The collected documents encompassed various study types, including randomized and non-randomized trials, prospective and retrospective studies, and observational studies like cohort studies, case-control studies, cross-sectional studies, and case reports. These documents spanned the period from 1833 to 2023.
Three authors (TH, HH, DD) meticulously reviewed the retrieved documents to ensure compliance with inclusion criteria. These criteria necessitated the presence of information on definitive treatment, recurrence, gender composition, and the duration of follow-up. Reports published in English, French, German, Italian, and Spanish were considered, and publications in other languages were included if they provided an English abstract detailing the definitive treatment, recurrence, and follow-up time. In instances where translations were required, authors were contacted via email or ResearchGate; alternatively, two different translation software packages were used to translate text passages of interest. Exclusion criteria encompassed PSD occurrences in locations other than the presacral region, involvement of neoplastic conditions, and duplicate publication of data by the same author. Studies lacking any component of the minimal data set, which includes information on the definitive treatment strategy, recurrence, and follow-up time, were also excluded. While previous meta-analysis reports and review articles were excluded, their reference lists were scrutinized for potential additions to the evidence. Moreover, unpublished data presented in review articles were considered.
Data collection, extraction, and quality assessment
All identified studies underwent thorough analysis and documentation. The transcribed data were subsequently entered into a Microsoft Excel spreadsheet (Version 2016, Microsoft Corp., Redmond, WA, USA) and subjected to verification to ensure accuracy. Each distinct therapeutic strategy reported in a study was allocated a separate line, with columns encompassing citation details, the number of included patients, therapeutic procedures, reported follow-up times, study particulars, and recurrence data. Given the variation in statistical measures used to report follow-up times across studies, we regarded mean and median reports as equivalent due to the concentration of disease incidence among young adults. For cases where minimum follow-up times were provided, these values were incorporated as reported.
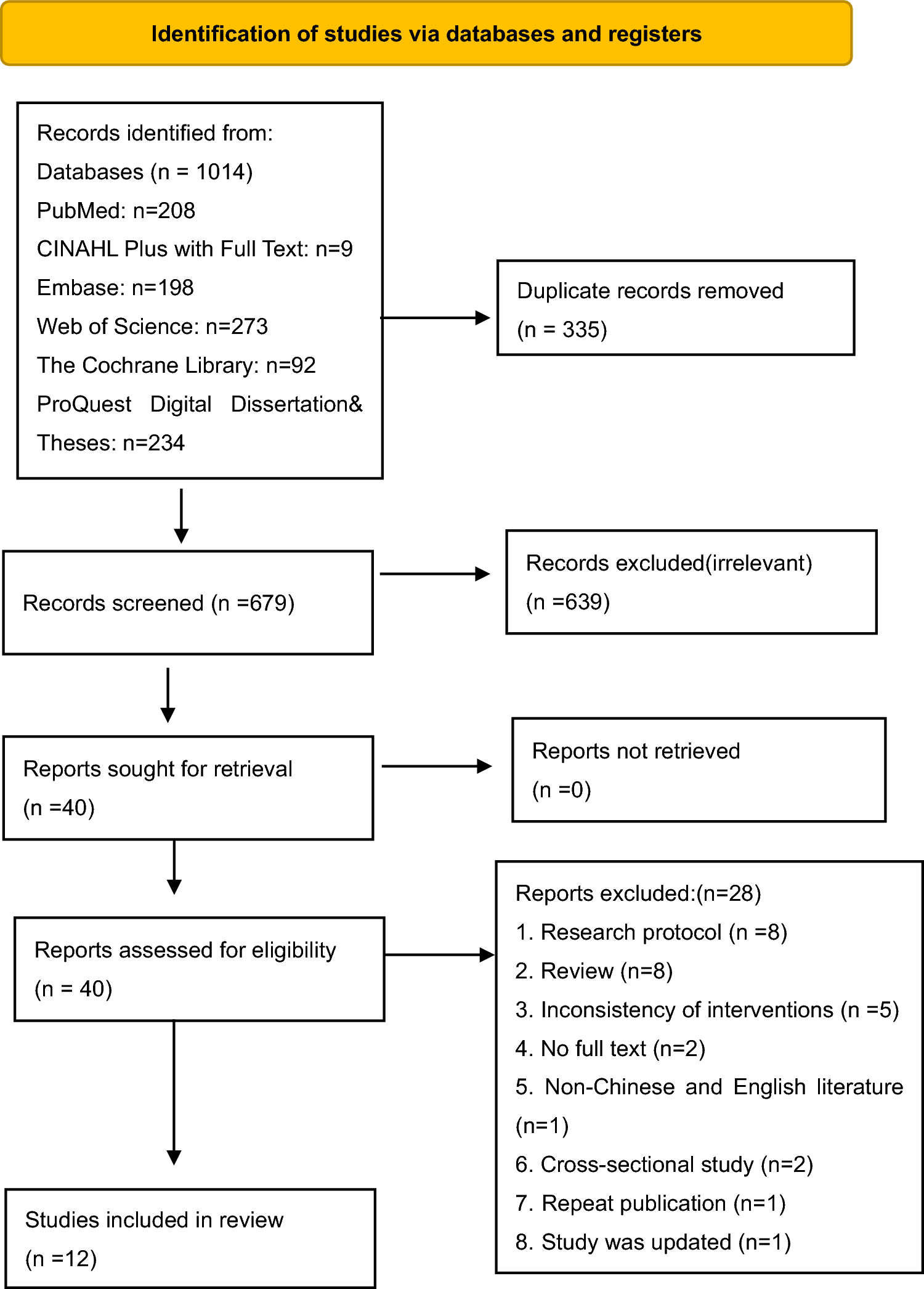
Individual studies were systematically scrutinized for methodological consistency and reported results to mitigate potential bias during data synthesis. A subgroup analysis was conducted for prospective randomized controlled trials (RCTs) to ensure alignment with the broader set of studies. The recurrence rates reported in each study were then associated with the respective follow-up time, whether defined as the mean, median, center of the range, or minimum. To facilitate uniform comparison across all studies, individual patients were statistically simulated, with each study participant represented as a data sample that included recurrence status, follow-up time, and therapeutic procedure. For example, if a study included 500 patients and reported a recurrence rate of 20% for a particular therapeutic procedure, we designated 100 single samples as having recurrent disease, while the remaining 400 samples were designated as recurrence-free. Certain information, such as gender ratios, was excluded as it was primarily available in aggregate form in the majority of studies. In cases where an article discussed multiple therapeutic strategies, data pertaining to each treatment strategy were separately analyzed. As pediatric PSD follows a completely different recurrence rate kinetic, which has been shown recently, only cohorts with a mean age of 18 years and older were accepted for this analysis [21]. As return-on-recurrence (ROR) studies are prone to large observation bias, which applies to PSD studies with ROR follow-up (SQ1) as well, these studies were also excluded (see PRISMA schedule Fig. 1).
A meta-regression analysis conducted beforehand on a cohort of 89,583 patients, which examined established RR modifying factors (choice of treatment, follow-up duration, age, methylene blue use) and potentially influential variables (year of therapy, country of treatment, annual caseload) on recurrence rates, confirmed the impact and ranking of these known factors. Other potential influences, such as family history and recurrence status (primary versus recurrent disease), were inconsistently reported in the global literature and were too sparse to be meaningfully analyzed. Cardiovascular comorbidities are rare in patients with PSD, who typically fall within the at-risk age range of 15–25 years. Previous co-interventions were also scarce and therefore not investigated.
Remarks on aspects of creating a worldwide database
This study aims for a comprehensive global survey, ensuring that the data presented represent nearly the entirety of the world literature on PSD rather than a selective subset. Thus, significant patient groups are unlikely to be omitted. Initial experimental therapies may go unrecognized if unpublished, but their numerical impact on the overall results is estimated to be minimal. The number of treated patients most likely exceeds the number published, and inferior therapeutic outcomes may be underrepresented due to publication bias. Therefore, our focus and commentary are restricted to published literature. The congruence between published and real-world results can be assessed by comparing international results (considering different publishing attitudes) or trends over time. These aspects have been previously examined through meta-regression and found to have a lesser impact [3].
Grouping of therapeutic procedures, gender cohorts, and statistical analyses
Therapeutic procedures were analyzed for RCT and non-RCT and subcategorized into therapeutic categories. Variants of therapeutic procedures were grouped according to the originating procedures, as outlined in Table 1.
Statistical analysis and visualization were performed using the R statistical software package (version 4.3.2) within the R‑studio framework (version 2023.6.1.524). Statistical significance was set at p < 0.05, and all tests were conducted in a two-tailed configuration. To evaluate the recurrence-free outcome over time, Kaplan–Meier survival analysis was employed, along with pointwise 95% confidence intervals (CI), implemented using the R‑package “survival” (version 3.5-7). These analyses were carried out for both RCT and non-RCT cohorts, and the results are presented as the percentage of recurrence-free outcomes along with their corresponding 95% CI. The package “survminer” (version 0.4.9) was used for graphical display. A two-tailed log-rank test was applied. Student’s t test was applied for two-group comparisons. The horizontal axes on the plots represented the number of patients within specific follow-up, given in months. In cases where specific data were not available for an interval, linear interpolation was applied to estimate recurrence-free outcomes based on the two nearest observed follow-up times. Time frame was truncated to 10 years postoperatively. To provide the most comprehensive assessment of recurrence, we evaluated the data of RCTs and non-RCTs. Due to the incremental nature of the Kaplan–Meier curves, minor discrepancies between the plotted and tabulated values may arise.
Table 1 Grouping of therapeutic strategies for analysis of recurrence rates in pilonidal sinus disease. * Bascom described and used two different procedures: “cleft closure/cleft lift” (merged with Bascom group) and “pit picking” (merged with pit picking group). Modified from Stauffer [11] and PiloNERDs [13] 





留言 (0)