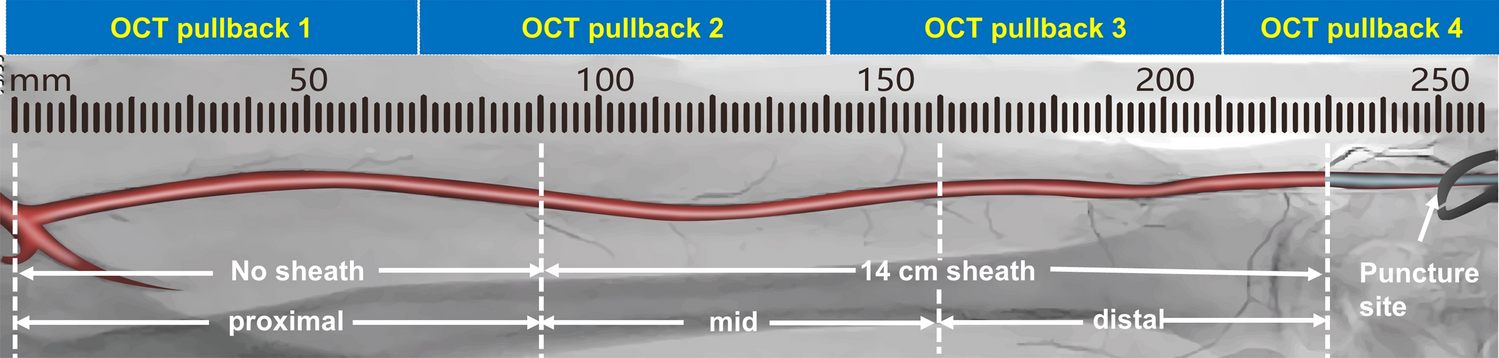
In the present study, dTRA was associated with acute RA injury in about half of the patients, as determined by OCT. The proximal segment, where no sheath was present, exhibited significantly more dissections and spasms than the mid and distal segments, which were sheathed. No significant differences were observed in the frequency or localization of intimal tears, perforations, and thrombi among the proximal, mid, and distal segments. These findings indicate the potential for sheath protection of the RA via dTRA.
Acute RA injury may be caused by RA puncture, sheath introduction, sheath friction from the RA inner diameter-sheath outer diameter mismatch or catheter, advancement of standard or hydrophilic guidewires, diagnostic catheters, or guiding catheters [8]. Currently, imaging methods used to clinically evaluate the structure of the RA include non-invasive high-frequency Doppler ultrasound, ultrasound biomicroscopy (UBM), invasive intravascular ultrasound (IVUS), RA angiography, and OCT. Non-invasive high-frequency Doppler ultrasound (spatial resolution 30–50 µm) and ultrasound biomicroscopy (UBM) (spatial resolution <70 µm) can display the rough outlines of blood vessels. Although these methods have certain advantages in evaluating injuries such as radial artery occlusion (RAO) or pseudoaneurysms, they are unable to clearly display the radial artery wall and the intraluminal structures [9, 10]. IVUS can assess the intraluminal structure of the RA and acute injuries; however, its resolution is limited to only 100 µm, which is considered low [11]. Meanwhile, OCT with a high resolution of 10–20 µm, can provide clear images of vascular walls and lumen structures. It is also more sensitive in detecting structural damage to the RA.
Determining the incidence of acute RA-injury post-procedure is challenging and varies due to factors including the observation period of the RA, sheath type and length, prophylactic vasodilatory spasmolytic therapy use, sample size, and access techniques. Reports from multiple studies indicate variances in the incidence of intimal tears (8.0–43.8%), dissections (3.0–35.6%), thromboses (0.0–24.2%), and spasms, with rates as high as 45.1% incidence detected by OCT following transradial intervention (TRI) [5,6,7,8, 12, 13]. In our study, the incidence rates of tear, dissection, thrombi, and spasm among all patients were 11.5%, 16.5%, 17.5%, and 17.5%, respectively, aligning with the previously mentioned reports.
Prior research using RA-OCT examination has demonstrated that intimal tears were observed more frequently in the distal portion with sheath protection than in the proximal portion with no sheath protection (43.8% vs. 17.8%, P < 0.001). Medial dissection frequencies were comparable between the distal and proximal portions (23.3% vs. 20.5%, P > 0.05) after TRI on time domain-OCT using a 16-cm long sheath, highlighting no benefit of sheath protection for the RA [5]. In the present study, we employed the same type and length of sheath and adhered to the same RA segmentation model with three segments outlined by Yonetsu et al. [5] yet reached different conclusions. We observed a lower rate of intimal tears that was not significantly different (5.0% in distal vs. 2.5% in proximal, P > 0.05), with dissection more frequent in the proximal segment (4.5% in distal vs. 11.0% in proximal, P < 0.05), suggesting a protective role for the sheath in preventing the razor effect of the guiding catheter during distal TRI (dTRI). These differences could be attributed to variations in sample size (42 vs. 200), the type of acute RA injury (with only tears and dissections noted in the prior study), access method (RA access vs. dTRA), vasodilators (isosorbide dinitrate vs. nitroglycerin plus verapamil), and OCT technology (first generation time-domain vs. second generation frequency-domain).
In another study, Di Vito et al. [6] used a 25-cm-long hydrophilic coated introducer sheath to cover the entire length of the RA, dividing it into proximal and distal segments. No significant differences were found in the incidence of RA acute injuries (intimal tear, medial dissection, thrombus, and spasm) between these segments, indicating that such sheaths could protect the RA against damage. Consistent with previous findings, our study revealed similar acute RA injuries within the sheath-protected segments (specifically, the mid and distal segments).
TRA causes significant structural and functional damage to the RA in situ, potentially leading to the severe complication of RAO. Injuries to RA have an important impact on the long-term patency of the RA conduit and arteriovenous fistula creation in patients requiring haemodialysis [14]. One strategy to lower the incidence of RAO is the use of dTRA. Several randomized controlled trials and meta-analyses have shown that dTRA is associated with a substantial reduction in the incidence of RAO [15,16,17]. In our study, RAO was diagnosed in six patients (3.0%) by ultrasonography 24 h after dTRA, aligning with previous studies yet significantly lower than the reported incidence of 7.7% of RAO within 24 h in TRA [14].
To the best of our knowledge, this is the first study to assess the incidence of acute injury throughout the entire length of the RA following a coronary procedure via dTRA using OCT. Our results provide compelling evidence that dissection and spasm are more frequently detected in the proximal RA (the sheathless part), indicating that the sheath acts as a protective factor in reducing such injuries.



留言 (0)