
記住我
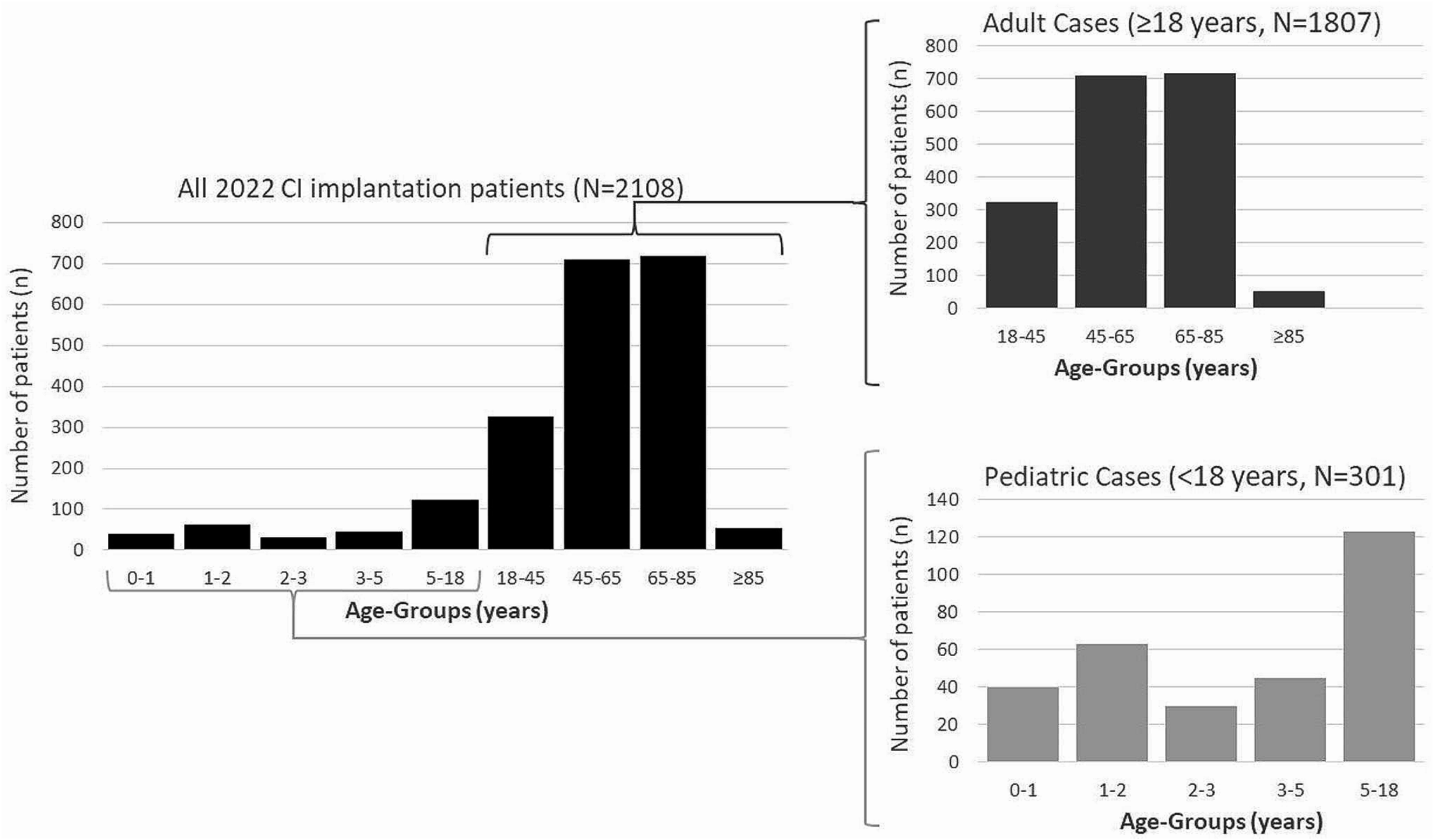



In 2022, data from 2,296 CI surgeries were collected from 63 ENT hospitals. Of those, 2,292 involved implanting a CI (2,176 first-time or primary implantations, 99 explantations with immediate re-implantations, and 17 re-implantations following an earlier explantation), while 4 surgeries were explantations only (without re-implantation during the same surgery). Of the 2,108 patients who received a CI in 2022, 1,807 were adults (≥ 18 years, 85.7%) and 301 were children (“pediatric patients”, < 18 years, 14.3%). The largest group of patients treated was aged between 65 and 85 years (N = 718, 34.1%), followed by the age group between 45 and 65 years (N = 709, 33.6%). Patients older than 85 years made up 2.6% (N = 55), patients younger than 1 year 1.9% (N = 40), and younger than 2 years 4.9% (N = 103). Within the group of pediatric patients (< 18 years, 301 patients), the age group up to 2 years represented just over a third of the pediatric patients treated (34.2%), while the age group under 1 year accounted for 20.9% of the pediatric patients (Fig. 1). There were 1,048 female (49.7%) and 1,060 male (50.3%) patients who received a CI. No patient was documented as diverse.
Fig. 1
Age distribution of the 2108 patients who received a CI in 2022. Right: detailed distribution of adult cases (upper panel) and pediatric cases (lower panel)
The number of surgeries registered by a hospital varied between 1 surgery (5 hospitals) up to 128 surgeries (1 hospital) with an average of 36.4 surgeries per hospital (median 26, Fig. 2). There were three institutions that contributed more than 100 surgeries to the registry and 18 hospitals which recorded more than 50 surgeries.
Fig. 2
Distribution of the number of cochlear implant (CI) surgeries registered in 2022 among the participating hospitals, dotted line: median value across all 63 hospitals
Unilateral and bilateral implantationsThese 2,292 implantations were carried out on a total of 2,108 patients, of whom 113 (5.4%) received a CI in each ear on the same day (simultaneous bilateral implantation). In comparison, a total of 428 patients received a second CI for the first time in their opposite ear, albeit not on the same day (sequential bilateral implantation) with 50 patients having received both their CIs sequentially in 2022. Twenty-one implantations were repeated (multiple) implantations in the same ear. Of the 226 simultaneous bilateral implantations, 162 (71.7%) were performed in children (< 18 years, 81 patients) and 64 (28.3%) in adults (≥ 18 years, 32 patients).
First language of patientsData on the main first language was collected for 1,831 patients. German was reported as the first language in 1,586 patients (86.6%). Of the 1,831 patients, 1,568 patients (85.6%) were older than 18 years. In 70% (N = 184) of the 263 pediatric patients stated German as their first language. In the group of the adult patients 1,402 patients (89.4%) used German as a first language.
Onset and duration of hearing lossFor the group of adult patients, the onset of hearing loss was documented for 1,578 implantations. In more than half of these implantations (N = 960; 60.8%), the onset of hearing loss had already been noticed > 10 years ago, while 129 implantations (8.2%) were reported to have a hearing loss less than 1 year before receiving the CI (Fig. 3).
Fig. 3
Distribution of hearing loss history among implanted ears for adult (aged ≥ 18 years) patients. In light gray the history of hearing loss (of any severity level) and in dark gray the history of severe-to-profound hearing loss
In addition, the duration of severe hearing loss or deafness in the ear to be treated was recorded. Of the 1,481 recorded ears in adult patients, 231 ears (15.6%) had severe hearing loss or deafness for less than one year. In contrast, 207 ears (14%) had severe hearing loss or deafness between 10 and 20 years, and 238 ears (16.1%) for more than 20 years. The group with hearing loss between one and 10 years included 805 ears (54.3%) (Fig. 3).
It was possible to classify the time of onset of hearing loss in relation to language acquisition for 2,068 implanted ears. The collection of this parameter is particularly relevant for the group of adult patients, for which data were available for 1,739 implanted ears. Of these, 95 (5.5%) showed a prelingual onset of hearing loss and 85 (4.9%) showed a perilingual onset of hearing loss. For the remaining 1,559 (89.6%), a postlingual onset of hearing loss was documented.
Etiology of hearing lossThe etiology of hearing loss was documented as known or unknown for 1,669 implanted ears. More than half of these (995; 59.6%) had an unknown etiology. Of the remaining 674 implanted ears, specific etiologies were documented in 646 instances. Of these 646 instances, the three most common causes that accounted for 55.4% of the known etiologies, were “age-related hearing loss”, a “genetic cause” and an “infection”. For further details, see Table 1.
Table 1 Etiologies of hearing loss*Preoperative hearing aid useData were collected from 2,202 implantations regarding the preoperative use of a hearing aid in the ear to be implanted just prior to cochlear implant surgery. For pediatric implantations, it was found that 220 of 387 cases (56.8%) had a hearing aid fitted on the implanted ear, while 167 cases (43.2%) did not. For adult patients, 1,034 out of 1,815 implanted ears (57%) had a hearing aid fitting just prior to implantation, while 781 ears (43%) did not.
Hearing in the contralateral earInformation on the hearing ability of the contralateral ear was documented for 2,162 implantations. Hearing loss was found in 1,750 ears (80.9%), whereas normal hearing in the contralateral ear was documented in 412 cases (19.1%, single sided deafness). Among the 412 implantations with contralateral normal hearing, 43 (10.4%) were children and 369 (89.6%) adults.
Data regarding the type of treatment of the contralateral ear at the time of surgery were available for 1,857 implantations. The most common treatment for the contralateral ear was a hearing aid (N = 1,064; 57.3%), followed by CI (N = 436, 23.5%). Seven cases (0.4%) were fitted with a bone conduction hearing system. No treatment with a hearing system was reported for 343 cases (18.4%). The information “unknown” or “other” was given in 7 cases (0.4%).
Surgical proceduresA total of 2,296 surgical procedures were documented. These consisted of 2,176 primary CI implantations (94.8%), 99 (4.3%) explantations with immediate re-implantation, 17 (0.7%) re-implantations following previous explantation, and 4 (0.2%) CI explantations without re-implantation. Thus, 2,292 CI implantations were documented in the DCIR in 2022.
Implants and implantation procedureIn 2022, data on four different manufacturers of CIs and their products was collected for 2,288 implantations (in alphabetical order: Advanced Bionics AG, Cochlear Corp., MED-EL Elektromedizinische Geräte GmbH, Oticon Medical GmbH). Of the documented implants, 1,617 (70.7%) had a so-called “lateral wall” electrode carrier, while 671 implants (29.3%) had a “preformed” electrode carrier.
For 2,284 implantations, information on the surgical insertion of the electrode could be obtained. In 1,911 cases (83.6%), the electrode was inserted via the round window. In 241 cases (10.6%), the electrode was inserted via a cochleostomy (other: 132; 5.8%).
For 2,265 implantations, data on the insertion depth was collected. Complete insertion was documented for 2,221 cases (98.1%), while in 44 cases (1.9%) there was partial insertion of the electrode.
Data on intraoperative measurement (e.g. stapedius reflex, neural response telemetry, eCAP) was collected for 2,241 implantations. In 2,082 cases (92.9%), the results were rated “normal”. In 134 cases (6%), the results were not “normal”. In 25 cases (1.1%), no intraoperative recording of electrically evoked compound action potential (eCAP) was done.
Radiological position control of the electrode carrierData on radiological position control of the electrode carrier were available for 2,176 (94.9%) implantations. Of these 2,176 implantations, information on the time of the examination was provided in 2,046 cases. In most cases, the radiological position control was performed postoperatively (1,635 of 2,046 implantations, 79.9%), and in 411 (20.1%), it was performed intraoperatively. Of the above 2,176 implantations where a radiological position control was performed, 2,001 implantations were documented as having either a regular (N = 1,965, 98.2%) or an irregular (N = 36, 1.8%) position of the electrode carrier. The used radiologic method was documented for 2,086 out of 2,294 implantations. The following methods were used: CT in 839 implantations (40.2%), DVT in 433 implantations (20.8%), conventional X-ray in 772 implantations (37.0%), other in 42 implantations (2.0%).
ExplantationsIn 2022, 103 surgeries were documented in which a CI had to be explanted. Of these, 99 cases (4.3% of all 2,296 surgeries) were explanted and immediately re-implanted, and 4 cases (0.2%) of CI explantation without re-implantation. Within the registry, the causes of explantation were assigned based on the recommendation of the 2005 “European Consensus Statement on Cochlear Implant Failures and Explantation” for categorization [19] (Table 2). The most common cause documented in the survey was class B2 (“Performance Decrement”) with 43 cases (41.7%), while a “Medical Reason” (e.g. explantation due to infection) was documented in 14 cases (13.6%).
Table 2 Reasons for explantationPostoperative fitting of the audio processorData from 1,371 patients or 1,549 CI-fitted ears were collected to record the postoperative fitting of the audio processor. For 440 ears (28.4%), it was documented that a “single-unit processor” was used. A behind-the-ear system was used in 1,034 ears (66.8%). In 75 cases (4.8%), the unspecific information “other” was given, so that no clear assignment of the processor type used was possible for this subgroup.
Postoperative CI useData on the usage time of CI use was collected for 1,060 patients (1,192 CI-fitted ears). Data logging was used for 963 ears (80.8%) and for 186 ears (15.6%) information was provided by the patient or their parents. “No information” was indicated for 43 ears (3.6%). The average daily usage time of the CI for each ear was 11.0 h.
ComplicationsComplications were recorded under the categories “hospitalization due to Cl-related complications”, “incorrect position of the electrode carrier requiring revision”, “meningitis after CI fitting”, “death in connection with CI fitting”, or postoperative facial nerve dysfunction (House Brackman grades I to VI). As more than one category may be present per reported case, the summary of these complications is shown in Table 3. Please note that in 3 cases, some of the categories were left blank. These are interpreted as being “No complication”.
In total, 19 complications were recorded, with 10 of these requiring “hospitalization due to Cl-related complications”, while the remaining 9 cases did not. Of these 10 “hospitalized” cases, only one was also documented as “incorrect position of the electrode carrier requiring revision”.
Of the 9 cases which did not require hospitalization, 4 cases were indicated as involving “incorrect position of the electrode carrier requiring revision”. Altogether, a total of 5 cases involved an “incorrect position of the electrode carrier requiring revision”, with only one of these 5 cases requiring hospitalization. There were no cases of documented “meningitis after CI fitting" or “death in connection with CI fitting”.
Postoperative impairment of facial nerve function of varying degrees of severity (from mild to moderate severe dysfunction) was reported in 7 of the 19 cases with complications. Four of these were mild (House-Brackman grade II), one was moderate (grade III) and two were moderate severe (grade IV). One patient with a grade III facial nerve dysfunction involved hospitalization, while one patient with a grade IV was also indicated as involving an “incorrect position of the electrode carrier requiring revision”. No case of a severe or total dysfunction (House-Brackmann grade V or VI) was documented.
留言 (0)