Over the years, FMF research has been fraught with debate on whether the pure p.E148Q variant is an insignificant variant [11,12,13,14], a disease-causing variant with low penetrance and mild symptoms [15], or a significant variant in specific ethnic groups [16, 17]. This study aimed to clarify the clinical characteristics and disease severity associated with the p.E148Q variant in FMF patients and contribute to the ongoing debate regarding its pathogenicity.
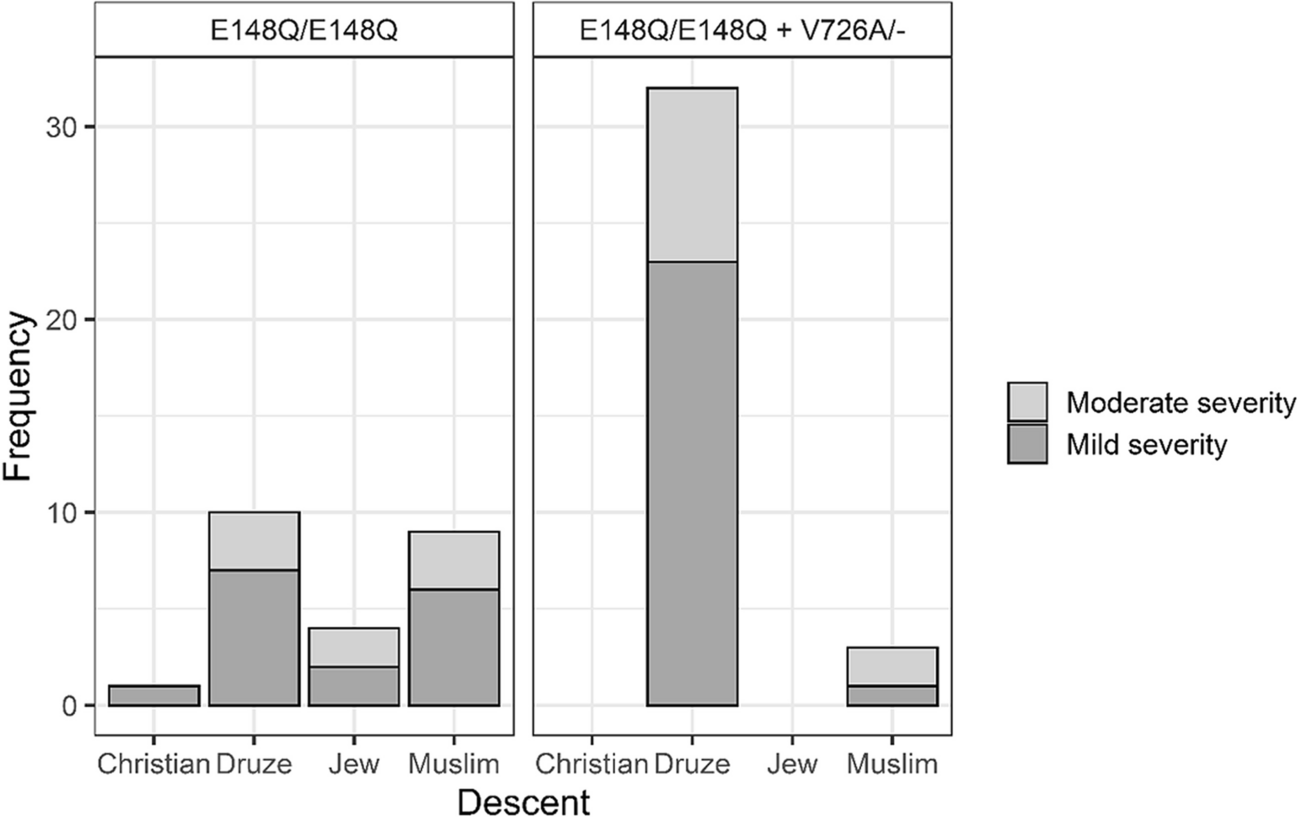
Our results demonstrated that the p.E148Q variant, whether in the homozygous state (p.E148Q/p.E148Q) or combined with the p.V726A mutation (p.E148Q/p.E148Q + p.V726A), is generally associated with mild to moderate disease severity according to Tel Hashomer Key to Severity Score [3]. Specifically, 40/59 = 67.7% of the patients exhibited mild disease, while 19/59 = 32.2% had moderate disease, and no patients presented with severe disease. This supports the hypothesis that patients who are homozygous for the p.E148Q variant with or without p.V726A may display a clinical FMF phenotype with mild to moderate severity.
Previous studies have yielded mixed results regarding the significance of the p.E148Q variant. For instance, a genetic study from Israel on patients of Jewish-Sephardic descent found similar frequencies of the p.E148Q allele among patients and controls, suggesting it might be a benign polymorphism [11]. Another study from Israel could not provide evidence to support the notion that p.E148Q is a disease-causing variant and not a mere genetic polymorphism, despite the large sample size [18]. Conversely, Aydin et al. reported that Turkish FMF patients with the p.E148Q variant alone presented later in life and had a milder disease course but exhibited similar clinical findings to those with more severe variants [15]. Similarly, Topaloglu et al. found that Turkish patients who are homozygous for p.E148Q and negative for other pathogenic MEFV variants may display a clinical FMF phenotype with moderate to severe disease activity, although the severity may be milder compared to patients with other variants [17].
A study on Egyptian FMF patients uniquely found the p.E148Q variant to be the most frequent MEFV variant (38.6%) in their FMF cohort, associating this variant with abdominal pain, fever, and high serum amyloid A. Notably, in this study, all patients were of Arabic descent, and 57.2% of this group had undefined variants [16].
Our current study strengthens these findings from several cohorts worldwide, suggesting that the p.E148Q variant is associated with a clinical phenotype rather than being a benign variant. The differences observed in different cohorts likely result from the varying prevalence of variants among different ethnic groups. In Israel, while the homozygous p.M694V mutation is the most prevalent among Jews, the p.E148Q variant is the most common among Druze (56%). Among other Arab citizens in Israel (Muslims and Christians), the three most prevalent homozygous mutations are p.V726A, p.M694V, and p.M694I [8]. This may explain the high percentage of Druze patients homozygous for the p.E148Q variant in our current study (72%) in addition to their significant geographical distribution in our region.
In a recent article, Ben-Chetrit et al. discuss the significance of carrying MEFV variants in symptomatic and asymptomatic individuals, since many MEFV gene variants remain unclassified, with around 30% as variants of uncertain significance (VUS). They conclude that only the presence of likely pathogenic variants on both alleles should result in a definitive diagnosis. Otherwise, diagnoses such as probable FMF or FMF-like disease are considered. Additionally, they emphasize that genetic testing is only part of the diagnostic process; a comprehensive evaluation of a patient’s medical history and clinical symptoms is essential for accurate diagnosis and treatment [19].
Adding to the ethnic diversity, the overall disease severity in our study was mild to moderate across all ethnic groups, except for Muslim patients with the p.E148Q/p.E148Q + p.V726A variant, who exhibited predominantly moderate disease severity. This ethnic variability underscores the importance of considering genetic background, in addition to the environmental factors, when evaluating FMF patients.
It is generally known that the addition of another heterozygous variant typically causes more serious disease phenotype in FMF. For instance, the p.V726A ± p.E148Q allele is considered to be associated with severe disease and strongly predisposes to renal amyloidosis, in contrast to an isolated p.E148Q variant [20]. Also, patients homozygous for the complex allele p.E148Q-p.V726A/ p.E148Q-p.V726A, or p.E148Q-p.V726A/ p.V726A compound heterozygotes have more severe disease compared to patients homozygous for p.V726A [18]. Interestingly, in our study, the addition of the p.V726A mutation did not aggravate the clinical phenotype in our cohort. However, knowing that p.V726A is a pathogenic variant, it is possible that with an increased number of patients in the cohort, the number of patients with moderate disease and carrying the p.E148Q/p.E148Q + p.V726A genotype will be significantly higher than those affected with the mild form and homozygous for p.E148Q. The fact that p.E148Q variant may have clinical significance even without additional MEFV mutations is further supported by the significant reduction in CRP levels following colchicine treatment, confirming the pathogenicity of the p.E148Q variant through objective inflammatory markers. In addition, this finding supports the importance of identifying and treating also cases with a mild disease severity.
Our study also examined clinical parameters such as age at disease onset, frequency of attacks, and colchicine dosage. Patients with moderate disease had an earlier onset, more frequent attacks, and required higher doses of colchicine compared to those with mild disease. These findings align with the expected progression of FMF, where earlier onset and higher attack frequency indicate more active disease.
However, our study has several limitations. Its retrospective design and reliance on electronic medical records may not capture all relevant clinical details. Additionally, the genetic analysis did not include the full length of the MEFV gene, potentially missing other pathogenic variants. Future research should include larger, multicenter cohorts and comprehensive genetic testing to validate these results and explore the molecular mechanisms underlying the variable expressivity of the p.E148Q variant.
In conclusion, our study provides valuable insights into the clinical characteristics and disease severity associated with the p.E148Q variant in FMF patients, supporting its pathogenic role in particular ethnicity. The findings suggest that p.E148Q, whether alone or in combination with p.V726A, generally results in mild to moderate disease, responds well to colchicine treatment, and exhibits variability across different ethnic groups. Continued research is essential to fully elucidate the pathogenic nature of the p.E148Q variant and its implications for FMF diagnosis and treatment.








留言 (0)