
記住我



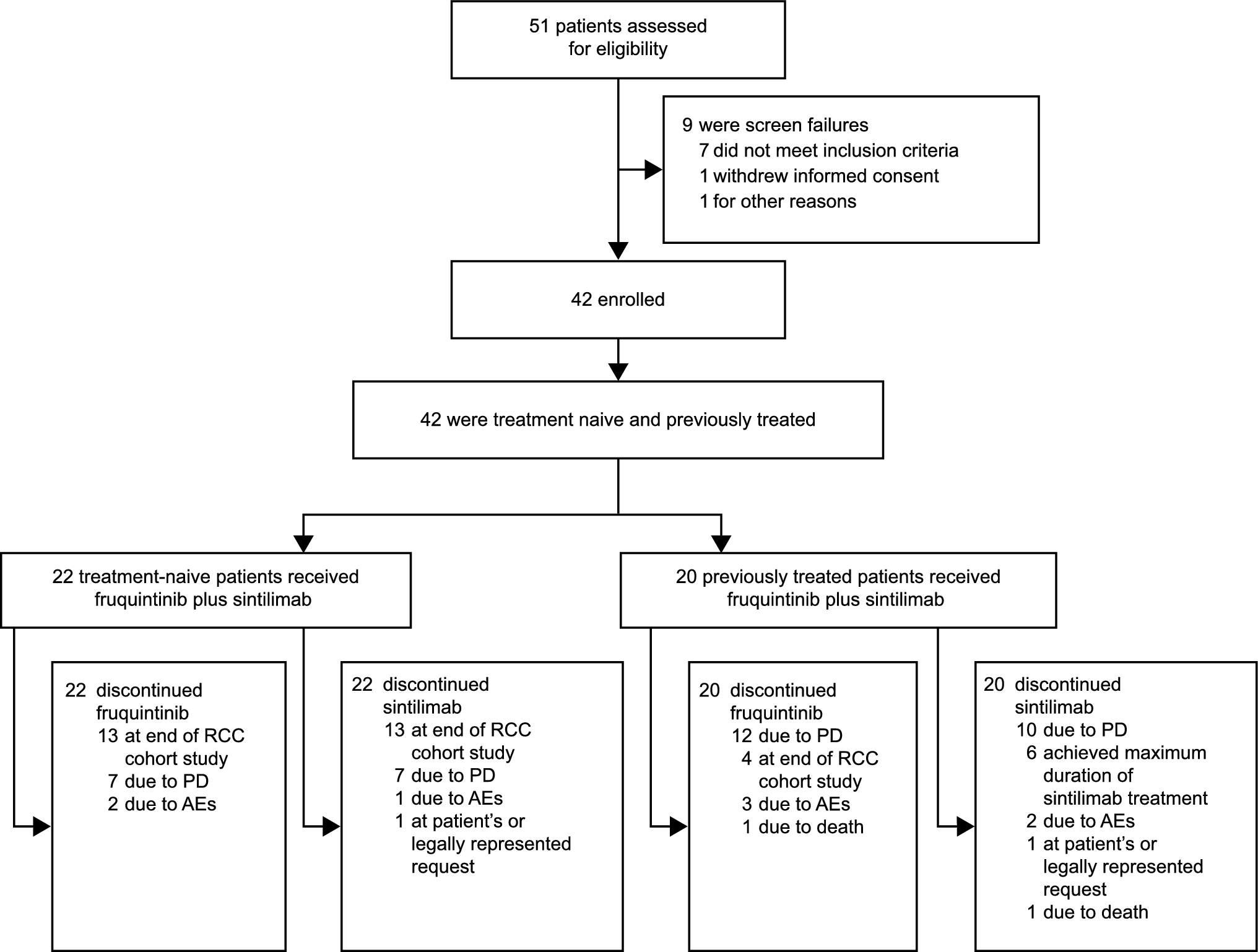




A flowchart of the study participant selection process is shown in Fig. 1. Of the 1380 patients considered for enrollment, 1062 patients with EGFR-mutated advanced or recurrent NSCLC, treated with any EGFR-TKI as first-line palliative treatment, were eligible. We identified 555 patients who received at least one dose of osimertinib during the treatment period: 416 and 139 patients in the 1L-Osi and 2L/later-Osi groups, respectively, with 103 and 36 receiving it as second-line and later-line treatments, respectively. A total of 646 patients were included in the 1L-non-Osi group: 404 received gefitinib, 119 received erlotinib, and 123 received afatinib as first-line treatment. Among the 293 patients for whom first-line treatment was initiated after March 2016 in the 1L-non-Osi group, 75 (25.6%) received osimertinib as second-line or later-line treatment. In contrast, among patients whose first-line treatment was started before this period, 64 of 353 patients (18.1%) received osimertinib as second-line or later-line treatment. The difference between these proportions was significant (p = 0.03).
Fig. 1
Patient flowchart. EGFR epidermal growth factor receptor, TKI tyrosine kinase inhibitor, VEGF vascular endothelial growth factor
The baseline demographics and clinical characteristics of the included patients are summarized in Table 1. The predominant histological subtype was adenocarcinoma, with most patients in Stage IV and a high prevalence of patients with a good performance status. A significant proportion of patients were never smokers. Mutations in addition to Del19 and L858R included G719X (n = 44), L861Q (n = 25), S768I (n = 8), exon 20 insertions (n = 5), exon 19 insertions (n = 1), G719X with S768I (n = 6), and G719X with E709A (n = 2).
Table 1 Clinical characteristics of patients treated with osimertinib or non-osimertinib epidermal growth factor receptor-tyrosine kinase inhibitors as first-line treatment before propensity score matching adjustmentApplying PSM at a 1:1 ratio, the study cohort comprised an equal number of 399 patients each in the 1L-Osi and 1L-non-Osi groups, including 283 with initiation dates for first-line treatment after March 2016. After PSM, there were no significant differences in clinical characteristics between the groups (Table 2). The baseline demographics and clinical characteristics of patients in the 2L/later-Osi group are summarized in Table 3.
Table 2 Clinical characteristics of patients treated with osimertinib or non-osimertinib epidermal growth factor receptor-tyrosine kinase inhibitors as first-line treatment, aligned through propensity score matchingTable 3 Clinical characteristics of patients treated with osimertinib as a second-line or later-line treatment following first-line treatment with non-osimertinib epidermal growth factor receptor-tyrosine kinase inhibitors3.2 Survival AnalysisThe median follow-up period for OS was 16.2 (IQR, 6.2–27.0), 20.3 (IQR 7.9–40.2), and 44.6 months (IQR 25.5–60.3) for the 416 patients in the 1L-Osi, 646 in the 1L-non-Osi, and 139 in the 2L/later-Osi groups, respectively. At the data cutoff point, the number of deaths in each group was as follows: 114 (27.4%) in the 1L-Osi group, 410 (63.5%) in the 1L-non-Osi group, and 84 (60.4%) in the 2L/later-Osi group.
The 1L-Osi group demonstrated an extended median OS of 42.0 months (95% CI 35.8 to not available [NA]), which significantly exceeded the median OS of 28.3 months (95% CI 24.9–31.0) in the 1L-non-Osi group (HR 0.63; 95% CI 0.51–0.78, p < 0.001) (Fig. 2a). However, in the cohort of patients for whom first-line EGFR-TKI treatment was initiated after March 2016, there were no significant differences in OS between the 1L-Osi (42.0 months: 95% CI 35.8 to NA) and 1L-non-Osi (42.4 months: 95% CI 33.8–51.0) groups when comparing all patients (HR 0.92; 95% CI 0.71–1.20, p = 0.55) (Fig. 2b). These trends for the 1L-Osi and 1L-non-Osi groups remained in the PSM cohort, where the median OS reached 42.0 months (95% CI 35.8 to NA) and 28.7 months (95% CI 24.8–33.0), respectively (HR 0.61; 95% CI 0.48–0.77, p < 0.001) (Fig. 2c), and the median OS reached 42.0 months (95% CI 35.8 to NA) and 42.4 months (95% CI 34.0–51.0) in the post-March 2016 cohort, respectively, with an HR of 0.89 (95% CI 0.67–1.18, p = 0.42) (Fig. 2d).
Fig. 2
Kaplan–Meier curves for overall survival (OS) in the first-line treatment with osimertinib (1L-Osi) and first-line treatment with non-osimertinib epidermal growth factor receptor-tyrosine kinase inhibitors (1L-non-Osi) groups: a throughout the study period, b after March 2016, c throughout the study period using propensity score matching, and d after March 2016 using propensity score matching. CI confidence interval, HR hazard ratio, NA not available
The median OS of the 2L/later-Osi group over the entire study period was 54.1 months (95% CI 47.0–60.2), and that for the cohort of patients who initiated first-line EGFR-TKI treatment after March 2016 was 60.2 months (95% CI 49.9–95.9) (Fig. 3) Conversely, for the 1L-non-Osi group without sequential osimertinib over the entire study period (n = 507), the median OS was 22.3 months (95% CI 19.7–25.0). For this group after March 2016 (n = 218), the median OS was 32.2 months (95% CI 24.0–40.0).
Fig. 3
Kaplan–Meier curves for overall survival (OS) in the second-line/later-osimertinib (following first-line treatment with non-osimertinib epidermal growth factor receptor-tyrosine kinase inhibitors) group. The black line represents data from the entire study period, whereas the red line represents data from patients who received first-line treatment after March 2016. CI confidence interval
Subgroup analysis of OS was conducted based on three EGFR mutations: Del19, L858R, and other EGFR mutations. Throughout the study period, for patients with Del19, the 1L-Osi group showed better OS outcomes (median OS, NA; 95% CI 35.8 to NA) than the 1L-non-Osi group (median OS, 30.9 months; 95% CI 27.5–38.4; HR 0.61; 95% CI 0.45–0.84; p = 0.002). Similarly, for patients with L858R, the 1L-Osi group had longer OS (median OS, 38.8 months; 95% CI 27.0–45.3) than the 1L-non-Osi group (median OS, 25.8 months; 95% CI 22.3–30.8; HR 0.67; 95% CI 0.49–0.91; p = 0.01) (Fig. 4a). No significant differences were observed for other mutations (1L-Osi: median OS, 22.0 months; 95% CI 7.3 to NA vs 1L-non-Osi: median OS, 19.0 months; 95% CI 12.3–36.7; HR 0.73; 95% CI 0.35–1.51, p = 0.39) (Fig. 4a).
Fig. 4
Kaplan–Meier curves for overall survival by epidermal growth factor receptor mutation type. a First-line treatment with osimertinib (1L-Osi) and first-line treatment with non-osimertinib epidermal growth factor receptor-tyrosine kinase inhibitor (1L-non-Osi) groups during the entire study period, b 1L-Osi and 1L-non-Osi groups after March 2016, c 2L/later-Osi (osimertinib in second-line or later-line treatment following first-line treatment with non-osimertinib epidermal growth factor receptor-tyrosine kinase inhibitors) group during the entire study period, and d 2L/later-Osi group after March 2016
In the cohort where initial treatment was initiated after March 2016, for Del19, there were no significant differences in OS between the 1L-Osi (median OS, NA; 95% CI 35.8 months to NA) and 1L-non-Osi (median OS, 49.9 months; 95% CI 36.1–82.5 months) [HR 0.83; 95% CI 0.56–1.21; p = 0.33] groups of patients. Similarly, for L858R, there were no significant differences in OS between the 1L-Osi (median OS, 38.8 months; 95% CI 27.0–45.3) and 1L-non-Osi (median OS, 38.4 months; 95% CI 27.1–47.3) (HR 1.04; 95% CI 0.70–1.54; p = 0.85) groups. For other mutations, there were no significant differences in OS between the 1L-Osi (median OS, 22.0 months; 95% CI 7.33 to NA) and 1L-non-Osi (median OS, 36.7 months; 95% CI 13.7–51.0) (HR 1.25; 95% CI 0.53–2.94, p = 0.61) groups (Fig. 4b). In the entire 2L/later-Osi group, the median OS was 58.4 months (95% CI 45.1–74.5), 50.9 months (95% CI 35.3–59.0), and 51.0 months (95% CI 5.5 to NA) for Del19, L858R, and other mutations, respectively, with no significant differences among the groups (Fig. 4c). A comparison of the L858R mutation with the Del19 mutation yielded an HR of 1.22 (95% CI 0.77–1.94, p = 0.39), and a comparison of other mutations with the Del19 mutation yielded an HR of 1.55 (95% CI 0.92–2.59, p = 0.10). Additionally, a comparison of other mutations with the L858R mutation yielded an HR of 1.79 (95% CI 0.63–5.12, p = 0.28). However, in the subset of patients where initial treatment was initiated after March 2016 in the 2L/later-Osi group, the median OS was 82.5 months (95% CI 58.4 to NA), for 49.1 months (95% CI 32.8 to NA), and 31.9 months (95% CI 5.5 to NA) for Del19, L858R, and other mutations, respectively (Fig. 4d). In the subset, there were significant differences between the L858R and Del19 groups, with an HR of 2.13 (95% CI 1.01–4.48, p = 0.046) and between the other mutation and Del19 groups, with an HR of 2.47 (95% CI 1.29–4.70, p = 0.006). However, the difference between the other mutation and L858R groups was not significant (HR 3.28; 95% CI 0.90–11.94; p = 0.07). In the population that began treatment after March 2016, a multivariate analysis identified several significant factors associated with OS. These factors include EGFR mutation type (HR 1.36, 95% CI 1.11–1.66, p = 0.003), histological type (HR 1.46, 95% CI 1.06–2.00, p = 0.02), ECOG PS (HR 1.39, 95% CI 1.22–1.57, p < 0.001), and disease stage (HR 1.76, 95% CI 1.37–2.26, p < 0.001). Conversely, the use of osimertinib as a first-line treatment was not a significant predictor of OS (HR 0.86, 95% CI 0.66–1.12, p = 0.27).
In the 1L-non-Osi group, in which the initial treatment was initiated after March 2016, a subgroup analysis of OS was conducted based on the EGFR-TKI used as first-line treatment. The median OS of patients initially treated with gefitinib, erlotinib, and afatinib was 40.2 months (95% CI 28.5–57.1), 33.1 (95% CI 23.6–45.2), and 46.8 months (95% CI 32.2 months to NA), respectively (Fig. 5). The differences among the three groups were not significant (p = 0.33). In the subgroup of patients who began their treatment with agents other than osimertinib after March 2016, a multivariate analysis identified several significant factors associated with OS. EGFR mutation type (HR 1.35, 95% CI 1.04–1.75, p = 0.03), ECOG PS (HR 1.28, 95% CI 1.07–1.53, p = 0.007), and disease stage (HR 1.71, 95% CI 1.26–2.32, p < 0.001) were significant predictors. Conversely, the type of EGFR-TKI used as first-line treatment was not a significant predictor (HR 0.93, 95% CI 0.76–1.14, p = 0.49).
Fig. 5
Kaplan–Meier curves for overall survival (OS) based on the epidermal growth factor receptor-tyrosine kinase inhibitors used in first-line therapy among patients treated with non-osimertinib epidermal growth factor receptor-tyrosine kinase inhibitors as their initial treatment (treatment initiated after March 2016). CI confidence interval, NA not available
In the 2L/later-Osi group, a subgroup analysis of OS was conducted based on the EGFR-TKI used as a first-line treatment. The median OS for patients initially treated with gefitinib, erlotinib, and afatinib was 54.1 months (95% CI 43.2–59.2), 41.8 months (95% CI 25.2–82.5), and 73.3 months (95% CI 46.8 to NA), respectively (Fig. 6). The differences among the three groups were not significant (p = 0.21). In this cohort, multivariate analysis identified the disease stage as a significant factor associated with OS (HR 1.68, 95% CI 1.06–2.65, p = 0.03). Other factors, including the type of first-line treatment used (HR 0.79, 95% CI 0.61–1.03, p = 0.08), were not significant predictors.
Fig. 6
Kaplan–Meier curves for overall survival (OS) based on the epidermal growth factor receptor-tyrosine kinase inhibitors used in first-line therapy among patients treated with osimertinib as second-line or later-line treatment following first-line treatment with non-osimertinib epidermal growth factor receptor-tyrosine kinase inhibitors. CI confidence interval, NA not available
3.3 Rationale Behind Transitioning Treatment to OsimertinibThe reasons for changing the treatment regimen to osimertinib in the 2L/later-Osi group (osimertinib as second-line or later-line treatment following first-line treatment with non-osimertinib EGFR-TKIs) were the following: disease progression in 111 cases (79.9%), of which 91 (65.5%) had T790M confirmed through rebiopsy before initiating second-line or later-line osimertinib treatment, 17 (12.2%) had unconfirmed T790M, and 3 (2.2%) were de novo T790M-positive cases; adverse events during first-line treatment in 25 cases (18.0%); and availability of osimertinib, recently launched in Japan, during the effectiveness of first-line treatment in three cases (2.2%).
留言 (0)