
記住我








This study utilised a socioecological framework and a participatory action research (PAR) methodology, focusing on the active engagement and empowerment of migrant and refugee youth (MRY) in the research process. PAR is known for its emphasis on the active participation and collaboration of communities in research, particularly effective in health research for addressing complex social issues [26, 27]. In SRHR research, employing PAR necessitates creating a space where research participants, researchers, and project advisory committee members collaborate as equal partners. In this way, they all contribute to defining key issues, co-creating solutions, and implementing changes while ensuring confidentiality and respecting the diverse backgrounds of participants. This methodology allowed research participants to participate actively in shaping research questions, data collection, and analysis, providing essential insights for the study. Bronfenbrenner's socioecological framework was used to analyse and interpret the data, categorising SRHR facilitators for MRY across different levels of influence. This approach helped in systematically examining how factors at each socioecological level interact to shape MRY's SRHR experiences.
Participants and procedureThe recruitment for this study was conducted in stages commencing 1 June 2020 to 12 June 2021, with the aim of including MRY participants in the research development (Table 1). The study engaged 87 MRY with varying migration backgrounds, and from diverse racial, ethnic, religious, socioeconomic, educational, sexual, and geographical backgrounds, comprising youth project liaisons (YPL, n = 8) and MRY (n = 79). Demographic data was collected from 75 participants, with a majority identifying as female (n = 56, 65.12%) and a minority as male (n = 19, 22.09%), aged between 15 and 29 years. Participants were eligible if they were between 16 and 26 years old, as per the ethics approval (Table 1). However, a 15-year-old nearing their 16th birthday, with parental consent and informed assent, and a 29-year-old who met all other criteria were also included. These deviations were considered to enhance the study’s comprehensiveness while maintaining ethical integrity. Appendix A shows that 50.67% of participants were born in Australia, while the remainder were born in countries such as Nigeria, Fiji, New Zealand, Thailand, and Iraq. This sample included both first-generation migrants (overseas-born) and second-generation migrants (Australia-born with at least one migrant parent), capturing a range of experiences with different levels of acculturation and connection to their migrant heritage. The sample represented children of economic migrants, refugees, and potentially expat families, though specific visa categories were not collected.
Table 1 YPL-Led SRHR focus group overview and participant criteriaAdvisory Committee Members (ACM), selected from community leaders, health professionals, and workers in community-managed organisations, contributed to implementing the PAR framework and co-facilitated the recruitment of YPL and MRY in collaboration with the research team. Central to the study, MRY provided qualitative data on their SRHR experiences based on the focus group probe questions (Appendix B). MRY were recruited through various channels, including ACM and YPL referrals, social media, community organisation newsletters, and postings in public spaces across Western Sydney University campuses and Western Sydney. This approach ensured the inclusion of a diverse range of youth in the study.
Data collectionWe conducted seventeen focus groups (M = 5.12 participants per session, with YPLs functioning as co-researchers and contributing as participants), predominantly via Zoom® to facilitate participation during the COVID-19 pandemic from 11 November 2020 to 12 June 2021. Using focus groups was important for vulnerable young people as it allowed the participants to interact with each other in a safe environment. It has been used extensively in research involving vulnerable people [26, 28]. In this study, "vulnerable young people" refers to MRY and their potential vulnerabilities regarding SRHR. These vulnerabilities stem from cultural differences, language barriers, unfamiliarity with the healthcare system, and conflicts between home and host culture values. Unlike other young people, MRY face added complexities in accessing SRHR information and services due to their backgrounds. The focus group sessions, primarily held in participants' preferred spaces, ranged from 60 to 90 min, with an average duration of 60 min. The first author co-facilitated 15 out of the 17 focus groups and the fourth author co-facilitated the remaining two sessions. These focus group discussions aimed to explore MRY's understanding and experiences regarding SRH, their rights, challenges, facilitators, and the solutions to address SRHR gaps in Western Sydney. The probe questions (Appendix B) were methodically crafted to explore the depth and breadth of MRY's experiences and understanding. To ensure the diversity of experiences and accessibility, the sessions were held in various formats. While focus groups were not specifically organised by demographic characteristics due to recruitment challenges with MRY populations, natural clustering occurred. This resulted from purposive sampling, where participants often brought in friends or acquaintances through word of mouth or community organisations. Three focus groups were conducted face-to-face to complement the online discussions. Two of these sessions occurred simultaneously in different areas of a local community-managed organisation in Greater Western Sydney, providing diverse and accessible settings for participant engagement.
Ethical considerationThe study received approval (H13798) from the Western Sydney University Human Research and Ethics Committee (HREC), ensuring ensuring adherence to ethical standards. Participants provided written informed consent and verbal consent at the start of each data collection session, with voluntary participation and the option to withdraw at any time. Confidentiality and anonymity were prioritised, with personal information securely stored on Cloudstor and anonymised. A debriefing process offered support for any distress during focus groups. The principal investigator maintained ongoing ethical oversight, promptly addressing concerns. YPLs, peers within the same age group as the MRY, facilitated the focus groups, reducing power differentials and enhancing the study's participatory nature, trustworthiness, and credibility.
Data analysisThe thematic analysis of the focus group data was conducted by the first, second, and last authors, following Braun and Clarke’s guidelines [29]. This analysis involved sifting through participants' narratives to identify recurring topics and substantial categories that align with the research objectives. To ensure confidentiality, pseudonyms replaced actual participant names. The software Quirkos® was employed to facilitate the identification of topical responses and the emergence of significant categories. Quirkos® is a user-friendly interface that simplifies the process of coding and analysing qualitative data [30]. It aided in coding various aspects of the data, such as word repetition, direct and emotive statements, as well as discourse markers such as connectives, evaluative clauses and intensifiers, following methodologies by Braun and Clarke and Liamputtong [29, 30]. Additionally, YPLs participated in a workshop to learn the basics of qualitative analysis, and two of them collaboratively analysed two of the 17 focus group transcripts in pairs. The codes they generated were integrated into the broader thematic analysis, enriching the study's qualitative data interpretation.
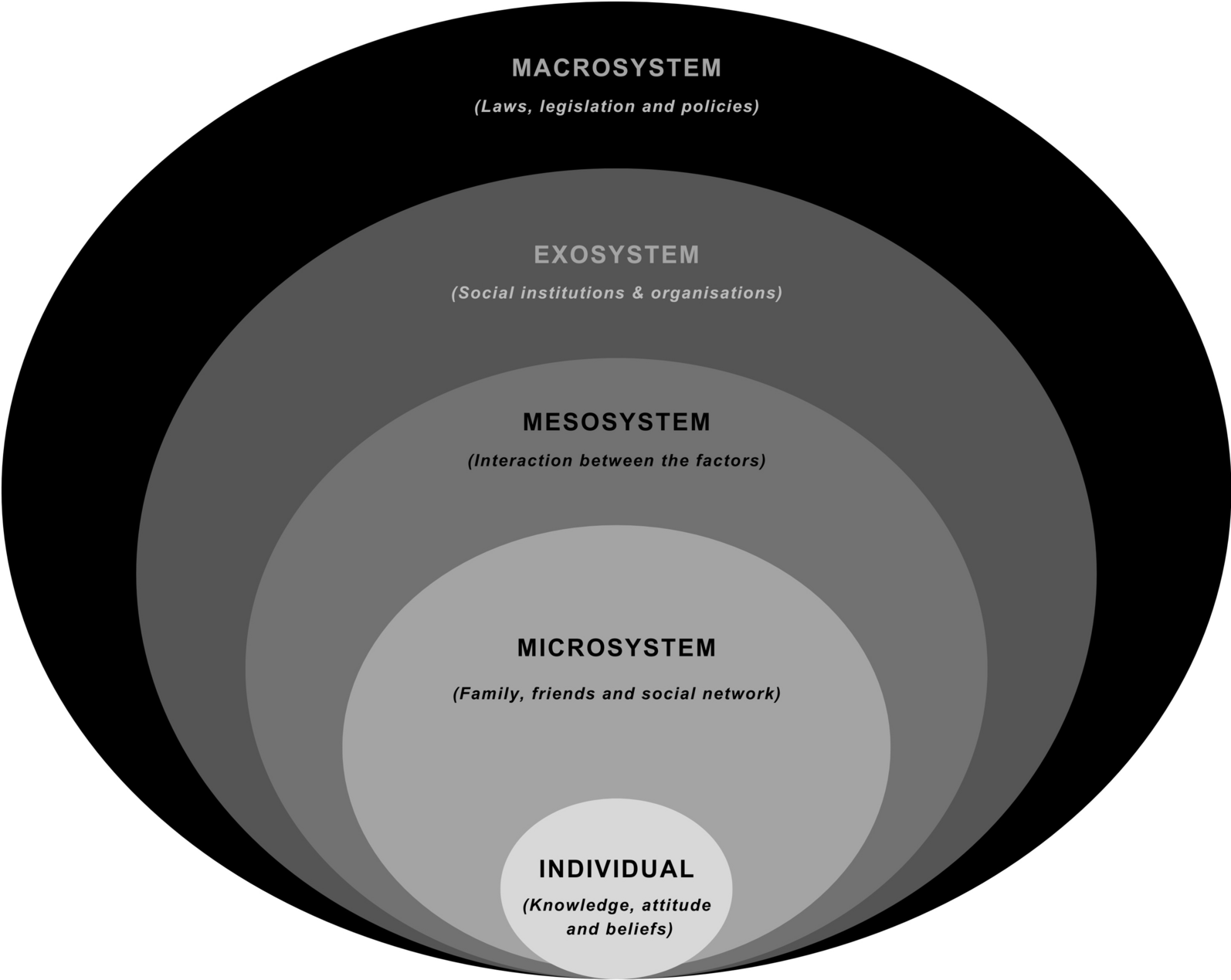
FindingsThe findings detailed below provide insights into the experiences and perceptions of MRY participants regarding the factors that facilitate the maintenance and protection of their SRHR. Through the thematic analysis of the focus group data, the analysis revealed three key socioecological facilitators of SRHR for MRY that were most relevant to the socioecological model's microsystem and exosystems (Fig. 2). These themes are (1) Peer Dynamics and Support, (2) Safety and Contraceptive Choices, and (3) Digital Information Access, as outlined in Table 2. These findings have also been shown in Table 3 to highlight the barriers and facilitators in the context of the socioecological framework.
Fig. 2
Bronfenbrenner’s socioecological framework: facilitators of sexual and reproductive health and rights in migrant and refugee youth (Sydney, July 2023)
Table 2 Themes and sub-themes emerging from dataTable 3 Themes highlighting barriers and facilitators under the socioecological frameworkMicrosystem influencesRepresenting immediate environments and relationships, the microsystem level is evident in the findings on peer dynamics and contraception choices, which highlight the crucial role of close interpersonal relationships and personal decision-making in shaping MRY's SRHR experiences.
Peer dynamics and supportThe data revealed significant insights into how MRY navigate their SRHR through peer dynamics and choices regarding contraception, representing the microsystem level encompassing direct and immediate environments. It revealed subthemes, which include:
Friends as confidants: MRY participants frequently reported the necessity of confiding in close friends when addressing SRH issues. This trust-based communication was pivotal in their understanding and decision-making processes. Amongst peers, the power dynamics at play are generally neutral which sets a comfortable engagement as summed up in the following statements among others,
“I feel like when you're with your friends, you're in a much more comfortable setting…, or for me anyway, I feel like I'm in a much more comfortable setting,” (Adebola, F, 16, Nigerian, FG 17),
and
“maybe like you feel more comfortable with your friends because we're all the same age and we're kind of learning this together.” (Kojo, M, 18, Ghanaian, FG 17).
Another participant added, “Just the level of trust I have with my friends is really different to my parents” (Georgina, F, 20, Nigerian, FG 17), emphasising the power dynamics usually present in the parent–child conversation, where the young person is constantly weighing the potential impact of their inquiry. Another stated,
“When I'm with my friends, they don't seem to be as judgemental or it's not really a topic that we have to think about” (Jana, F, 18, Iraqi, FG 17).
It reveals that MRY are foremost keen on their peer relationships to explore their SRH concerns before considering other options.
Seeking opinions and advice: Advice and opinions from friends, especially those with prior experiences in SRH matters, were crucial in shaping participants' attitudes and approaches towards their SRHR. MRY do this in their bid to make sense of their SRHR situations. A participant stated,
“Yeah, we talk to friends, and then friends give their experiences, and then we have [to] search our own mediums, just trying to understand it.” (Madi, F, 25, Sierra-Leonian, FG 4).
While participants alluded that their peers’ opinions may not be accurate, it provided the springboard for further exploration, consulting other information channels available to them. Nonetheless, participants agreed that the opinion or advice provided by friends is more likely to be acted upon, with one participant reflecting,
“So yeah, going to friends would be, would have been my first point in contact to making informed decisions at that time” (Angeline, F, 23, Indian, FG 4),
“Yeah, so, like, we learned about it in school for a little bit. And then if I needed further questioning, I had unanswered questions. I guess I would either ask people I knew, like my friends or like the Internet.” (Zantla, F, 18, Bangladesh, FG 2).
Although rare, participants also highlighted that their peer group could extend to family members with whom they share similar interests or trust. Lara (F, 19, Indian, FG 4) explained,
“I think the only person that I felt comfortable talking about it [sexual problem] to was one of my cousins, who was actually back home in India.”
This shows that MRY’s engagement with peer relationships goes beyond their immediate physical environment, provided a shared interest is embedded in mutual trust.
Experiences sharing: Conversations with friends who had personally encountered SRH issues provided practical insights and fostered a sense of shared understanding among the youth. Besides family members, participants expressed the ease in having SRH conversations with peers with similar experiences, highlighting that:
“Except like people our age, like our friends or our siblings [like], and they (peers) have as much experience as we do, like we're on the same level” (Merelita, F, 18, Fijian, FG 7).
“For me, it's mostly just friends who've done it, and mostly, I mean, if I get to hear something, which I would feel is like, OK, I need to look this up, it'll be mostly Google or again, porn, and it's mostly friends usually. Yeah, those are the main sources I would get information about sex from.” (Navdeep, F, 19, Indian, FG 4).
From the above, it shows MRY are more likely to solicit the experiences of peers who have had sexual experiences as a guide to making informed decisions.
Safety and contraceptives choicesPersonal experiences: The narratives shared by participants highlight the significant impact of personal encounters with SRH issues on their approaches to SRHR. These personal experiences serve as vital pathways for learning and shaping SRHR decision-making. One participant articulated the value of personal agency and the lessons learned from the outcomes of one's choices, stating,
“It's important to voice your own opinions and draw and then, as a result, have your choices as your actions. And if your actions aren't the best, then you'll have to face the consequences, which is all about the experience” (Johnny, M, 23, Indian, FG 10).
This reflection indicates that MRYs perceive their capacity to make and act upon decisions, regardless of the consequences, as a fundamental aspect of their SRH decision-making process. Another participant shared their perspective on making informed choices regarding contraception, reflecting,
“If I was using a pill, if I was using contraception, and even though that, for me, was… the best decision or the most informed decision I could make, and that was like to protect my sexual and reproductive health” (Nadia, F, 21, Polish, FG 4).
Nadia's account demonstrates how personal decisions about contraception are seen as critical to safeguarding one's sexual and reproductive health. These statements underscore the importance of experiential learning and personal autonomy in the SRHR journey of migrant and refugee youths.
Contraceptive options: The data also highlights the impact of the range of contraceptive choices available in facilitating informed decision-making in SRHR. Participants noted that while initially obtaining information and access to contraceptives posed challenges, the availability of various options significantly bolstered their sense of autonomy once these initial barriers were overcome. One participant highlighted the importance of accessible options by recounting,
“I've actually referred back a lot of my friends to them (YB Health) as well, because they used to say, like, oh, I couldn't get access to contraception.” (Peta, F, 22, Chinese, FG 4).
This indicates the broader community impact of accessible contraceptive solutions beyond MRY. Another participant highlighted the place of accessible contraceptive provisions, sharing,
“I guess having access to contraception, for one, because obviously I don't want any sort of direct threats, to put it safe, I guess.” (Daniel, M, 21, Australia, FG 1).
This highlights the empowering effect of having sustained access to contraception, underlining the importance of such services in supporting individuals’ SRHR needs and rights.
Access to Peer SRH information at student-organised events: This sub-theme focuses on how university campus events are vital platforms for enhancing knowledge and practices related to MRY’s SRH. The participants highlighted the significance of these events, where free and open conversations about SRH are encouraged, and resources like free condoms are readily available, fostering a supportive environment for safe sexual practices. One participant reflected on the open and informative nature of these gatherings, stating,
“And like people could just literally go up and ask questions and [the student organisers] were more than willing to talk to you about anything; …that kind of opened my eyes a bit. (Amina, F, 18, New Zealand-Arabic, FG 12).
This statement illustrates the importance of having a non-judgmental space where young people feel comfortable seeking and sharing information. Similarly, Peta, a 22-year-old Chinese female participant (FG 4), recounted,
“So while I was at Uni, like my first year, ages ago, we used to talk about this kind of things, sexual and reproductive health, and one of my friends actually referred me to this place called YB Health”
This narrative highlights the peer-to-peer learning and referral system that can emerge within university settings. Another participant shared her experience of a campus event focused on safe sex, noting the wide array of resources and discussions available:
“Like a month or two ago, and that was the first time, [like] there was a whole [like] stall on [like] safe sex on campus. I also read for the first time [like] me and my friends, [like wow, like, wow], like, just like it's just out there and [like] they were …like second years and third years [like] explaining stuff like that. There were [like] pamphlets on consent and [like] it was so [like it was like] really integrated well within [like] the week that we had at Uni. And for [like] many of my friends, it was the first time we ever [like]… I'm just using the word out in the open” (Amina, F, 18, New Zealand-Arabic, FG 12).
Her enthusiastic recount demonstrates the impact of these events in demystifying and normalising discussions around SRH, making them more accessible and less taboo for students.
Protection from STIs and unplanned pregnancy: Participants emphasised the importance of safeguarding themselves against sexually transmitted infections/diseases (STIs) and unplanned pregnancies as a fundamental component of their SRHR. One individual expressed,
“Using protection is [not] just for like really unwanted pregnancies, and you don't want an STI, anything (laughs); that's how I consider it, any form (Melinda, F, 23, Arab-Australian, FG 13).
This comment reflects a broad understanding of the dual purpose of protection, highlighting its role in preventing pregnancies and guarding against STIs.
The sentiment among participants was that prioritising the use of protection was crucial, irrespective of the type, provided it effectively prevented both unplanned pregnancies and STIs. This perspective underlines a proactive and informed approach to sexual health, acknowledging the dual risks involved in unprotected sex. Another participant further articulated this viewpoint,
“It's just a smart thing to do. Like, you never know, like there's other forms of contraception, obviously, but I feel like you still want to just make sure, I guess, like something can go wrong all the time and you know, people make mistakes.” (Li, F, 22, Thai, FG 13).
This statement suggests a pragmatic approach to contraceptive use, recognising its importance in mitigating risks and accounting for human error.
Exosystem influencesThe exosystem level, involving broader social settings that indirectly impact individuals, is reflected in the findings on digital platforms, showing how technology and media environments significantly influence MRY's SRHR information-seeking behaviours.
Digital and information accessThe significance of digital platforms, especially social media and various online resources, was identified as a crucial exosystem influence on MRY. MRY reflected on their major source of information being internet resources such as health e-magazines, social media groups, and specialised websites to gather information on SRHR, significantly shaping their understanding and decision-making. Participants shared insights suggesting, “Google search health organisations” (Li, F, 22, Thai, FG 13), illustrating their reliance on internet searches to find relevant health organisations and information. Further emphasising the role of digital media in filling educational gaps, another participant noted,
“I had to figure it out, what sex really is, and what consent really is and how to have safe sex via social media instead of education.” (Leila, F, 21, Lebanese, FG 7).
This comment highlights how MRY are self-educating on critical SRHR topics through online platforms in the absence of formal education. Additionally, the ease of accessing specialised services online was underscored by a participant who shared,
“Personally, I just went to the sex clinic that I found online” (Shiv, M, 19, Fijian, FG 4).
This statement reflects the proactive steps taken by MRY to seek out services and information digitally to support their SRHR needs.
Google for SRH information: The data revealed evidence that Google serves as a vital tool for many participants seeking SRH information. This preference underscores the significance of readily accessible online resources in bridging SRHR knowledge gaps. Participants expressed a strong reliance on this platform, with one noting, “OK, so Google is kind of like, saving grace” (Ayelen, F, 17, Nigerian, FG 17). This sentiment was echoed by another who described Google as a "safe haven" for finding crucial health information:
“Literally, Google is like your safe haven, you know what to search up or what you need to make sure you're safe and whatever” (Rita, F, 18, Liberian, FG 7).
The straightforward nature of seeking information was further emphasised with the remark.
“Go Google it, and you find the information for yourself.” (Nas, M, 21, Indian, FG 7).
Moreover, the discreet and private aspect of using Google was highlighted as a key advantage, especially when discussing topics that might be difficult or taboo to bring up with parents or peers:
“That's when people start going on Google. You obviously can't talk to your parents, then with Google, you don't have to talk to anybody, just type until you get answers” (Shaw, M, 22, Thai, FG 7).
This point underscores the value of Google as an accessible, confidential, and user-friendly resource for MRY to obtain the SRH information they need independently and privately.
Social media platforms: The data showed that platforms like TikTok, Twitter, Facebook, and Instagram were commonly utilised by MRY to access SRH information. These platforms offer a wide range of content, including personal anecdotes and media articles, providing users with various perspectives on SRH issues. While participants recognised that these platforms are not always reliable sources of SRHR information due to the potential for misinformation, the influence of social media in this space is undeniable. One participant expressed concern about the reliability of these platforms, stating,
“I agree, young people do generally reach out to social media platforms, which is not ideal, because, again, there's false information, misleading” (Faith, F, 18, Australian, FG 10).
Despite these concerns, the role of social media in disseminating information about physiological functions and other SRH topics was highlighted by another participant, “I had to learn that (about SRH) via social media,” adding,
“There is so many things that we didn't know until social media came around and we had to discover on our own (Adebola, F, 16, Nigerian, FG 7).
This indicates that, for many, social media has been a significant source of discovery and learning in areas where traditional education may be lacking. Another participant echoed the sentiment, acknowledging the extensive influence of social media, particularly among the youth,
“I completely agree that social media is a huge, like it's huge influence. ...Social media has great potential for learning things and it's kind of more geared towards, especially towards the younger population. (Ron, M, 20, Chinese, FG 12).
This comment underscores the dual nature of social media as both a vast repository of knowledge and a platform that requires critical evaluation and verification to ensure the accuracy and reliability of the information consumed.
Other internet sites: The data also indicate the complex and varied online landscape navigated by participants seeking out a wide array of online sites to gather information related to SRHR, spanning health e-magazines to pornography sites despite credibility and misinformation concerns. One participant remarked,
“So the first line of defence, I would say, is that they would go online and look at some un-credible sources, sometimes they can do that, but they need to filter out through those sources what is reliable and credible, such as .com.au websites, government websites, and from those they can gain some information about treatment options or, yeah, things like that.” (Aylin, F, 18, Turkish, FG 10).
Other participants echoed similar sentiments about the educational gap, revealing how individuals often turn to the Internet for information and community experiences they feel are lacking in traditional educational settings. Furthermore, the personal nature of the information sought and shared online was highlighted in the comment, “A lot of the social media that I research on, is personal experience” (Monique, F, 21, Bosnian, FG 7), reflecting a trend towards seeking and valuing personal narratives and experiential knowledge in understanding and navigating SRHR.
The study also produced several participant-proffered solutions (Table 4), aligning with the identified themes and sub-themes which will be discussed in a supplementary paper. These solutions offer practical insights into enhancing SRHR education and support for MRY.
Table 4 Solutions proffered by MRY participants
留言 (0)