Trial design
PREMEDI was a randomized, parallel-group, controlled trial aimed at evaluating the effects of MD during pregnancy on the prevention of overweight/obesity at 24 months in the offspring.
Participants
All pregnant women in their first trimester of pregnancy consecutively observed at a Tertiary Center for Gynecology and Obstetrics were evaluated for the study. These subjects were evaluated by a Research Team (RT) composed of gynecologists and dietitians experienced in clinical trials. The RT evaluated the presence of inclusion and exclusion criteria, provided information regarding study design and outcomes, and collected written informed consent from the women.
Inclusion criteria were Caucasian ethnicity and age range of 20 to 35 years. Exclusion criteria were documented infections during pregnancy, twin pregnancy, malignancies, malformations, immunodeficiency, diabetes mellitus and other chronic diseases; chronic inflammatory bowel diseases; gastrointestinal functional disorders; celiac disease; a history of abdominal surgery; neurological and neuropsychiatric disorders; and the utilization of a vegan diet.
Intervention
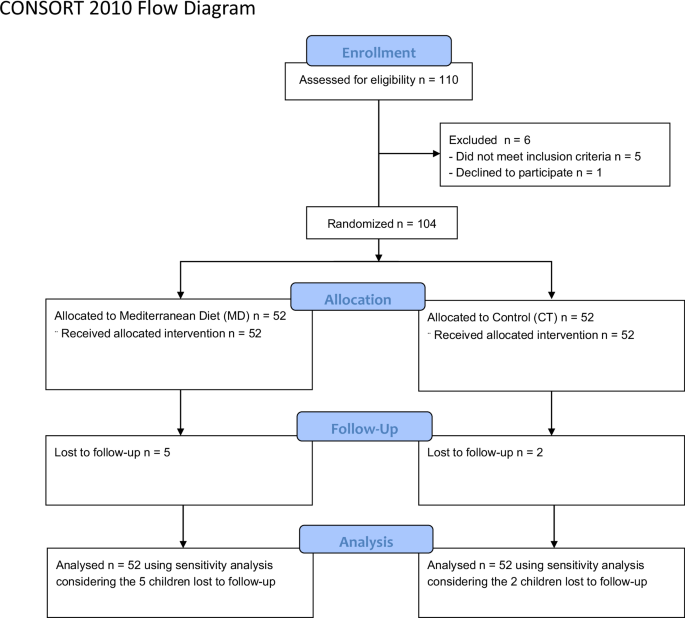
Soon after the collection of the written informed consent, the study subjects were randomly allocated in a 1:1 ratio to the CT or MD arms by the RT.
Women enrolled in the CT group were provided standard-of-care recommendations by the gynecologists operating at the Center. Such recommendations included energy intake, physical activity, optimal weight gain during pregnancy based on pre-pregnancy weight [12], and hygiene rules for food-related illnesses [13]. Whereas, women enrolled in the MD group, received standard obstetrical and gynecological care plus personalized MD nutritional counseling provided by certified dietitians operating at the Center. The MD nutritional counseling was performed in three face-to-face sessions at enrollment (8–13 gestational weeks), 3 months (14–28 gestational weeks) and 6 months after the enrollment (29–40 gestational weeks). MD nutritional counseling was based on the following recommendations: use of extra virgin olive oil as the main cooking fat (at least 4 tablespoons/day); intake of 2 servings/day of vegetables; intake of 3 servings/day of fruit, avoiding juices; intake of 3 servings/day of wholegrain cereals; intake of 3 servings/day of skimmed dairy products; intake of 3 servings/week of legumes; intake of 3 servings/week of fish; intake of 3 servings/week of nuts and seeds; intake of 2 liters/day of water; low consumption of red meat and processed meat; and avoidance of refined grains and ultraprocessed foods including processed baked goods, pre-sliced bread, soft drinks, fruit juices, and precooked meals [14].
Outcomes
The primary outcome was the proportion of children with overweight or obesity at 24 months of age in the MD vs. CT arm, as detected by the International Obesity Task Force (IOTF) growth charts [15]. The analysis of the primary outcome was prespecified as intention to treat (ITT). Other outcomes were maternal adherence to MD, as detected by the MedDiet Score [16], maternal weight gain, and epigenetic modulation of metabolic pathways in the offspring. These non-primary outcomes were analyzed using per-protocol analysis (PPA).
Sample size calculation
Sample size was calculated based on the primary outcome, i.e., the proportion of offspring with overweight or obesity at 24 months. Based on prior observational studies, we expected an incidence of overweight or obesity at 24 months of 25%. To detect an absolute difference of 20% in the proportion of overweight or obesity at 24 months at an alpha level of 0.05 and with a power of 80%, 49 mother-child pairs per group were necessary (Pearson Chi-square test). Assuming a dropout rate of up to 5% as in our previous studies, we enrolled 52 mother-child pairs per group, for a total of 104 pairs.
Randomization
A central randomization procedure was applied to allocate women in a 1:1 ratio into the MD and CT arms. The randomization list was generated by applying the ralloc command with block sizes of 2 in Stata version 14.2 (Stata Corporation, College Station, TX, USA) [17].
Allocation concealment
The treatments were consecutively numbered according to the randomization list, which was known only to the study coordinator [18, 19].
Blinding
Blinding the women was not possible because of the nature of the intervention. The collection of main study outcome data was performed by physicians and pediatric nurses unaware of the study outcome and group assignment.
Study monitoring and data management
Study monitoring was performed by an independent clinical trial monitor and included on-site visits and telephone interviews with the investigators. The monitor reviewed the study forms for completeness, clarity, and consistency and instructed the researchers to make any needed corrections or additions. The clinical researchers entered data in a case report form. Such data was anonymized and entered into an electronic database by the same researcher. The database underwent data cleaning according to standard procedures and was locked before statistical analysis, performed by a statistician.
Data collection
At enrollment, a multidisciplinary team composed of gynecologists and certified dietitians operating at the Center evaluated the following variables: anamnestic, clinical, and anthropometric features of all women enrolled in the study, socio-demographic factors, gestational age, allergies, number of cohabitants, pets, physical activities, use of drugs, smoking exposure, education level, family and living conditions. The MedDiet Score, a validated 14-item questionnaire assessing MD adherence, was administered by the dietitians involved in the multidisciplinary team [16]. Each item has a score of 0 or 1, with a total score ranging from 0 to 14. Adequate adherence to MD was determined as a MedDiet score ≥9. All data were collected anonymously in a dedicated clinical chart. The intake of dietary supplements, pre-, pro-, and symbiotics were recorded in the same chart. Follow-up visits were scheduled at gestational weeks 8 to 13, 14 to 28, and 29 to 40. During these visits, the multidisciplinary team performed a full anamnestic and physical examination and assessed the MedDiet Score. A cord blood sample (≥10 ml) was collected by the gynecologists at delivery in the first 11 women enrolled in each arm. For all babies after delivery, a follow-up visit was planned every 3 months for the first 12 months of life and then every 6 months until the age of 2 years. At each visit, a team composed of pediatricians, allergists and pediatric nurses, unaware of study aims and group assignment, collected data regarding anamnestic and clinical features, body growth, occurrence of allergic diseases and/or other chronic disease, and antibiotic use. The diagnosis of overweight or obesity in the offspring at 24 months of age was made using the International Obesity Task Force (IOTF) body mass index (BMI) cut-offs [15]. Anthropometric measurements (weight and length) were collected following standardized procedures. Briefly, subjects were weighed naked twice on calibrated electronic scales (Seca 834) or on mechanical scale (Seca 711). Supine length of infants was measured twice using a standard measuring board (Seca 210 Mobile Measuring mat). If the anthropometric measures deviated substantially (>100 g for weight and >5 mm for length), a third measurement was obtained.
DNA isolation from cord blood, methylome analyses and ultra-deep DNA methylation at leptin gene
Cord blood samples were collected at the time of delivery in EDTA tubes. Genomic DNA was extracted using the DNA Extraction Kit (GE Healthcare, Uppsala, Sweden) following the manufacturer’s protocol. Methylome analyses were performed by using Epic Array Illumina 850k. Bioinformatic analyses were performed on IDAT files by applying RnBeads R-based scripts [20, 21]. As a first step, the quality score was determined. According to sample annotations, batch effects and phenotype covariates were identified. DNA methylation distributions and intergroup as well as intragroup variability in methylation profiles were analyzed. Differential methylation between groups of samples was calculated. Differentially methylated CpG sites, promoters and CpG island were calculated among single samples and between groups using the Mann-Whitney U test. According to the dissimilarities in terms of DNA methylation at each of the 850k CpG sites, a Principal Component Analysis (PCA) was performed, and PCA plots were generated. To analyze DNA methylation at the Leptin gene, we generated an amplicon library for sequencing as previously described [22, 23]. Briefly, genomic DNA was submitted to bisulfite treatment and a double amplification strategy was adopted. The first PCR step was performed using bisulfite-specific Leptin primers with Hot Start Taq (Qiagen) and with the following temperature conditions: 95 °C for 15 min; 36 cycles of denaturation at 95 °C for 30 s; annealing at 53 °C for 40 s; and elongation at 72 °C for 1 min and 72 °C for 10 min. The second PCR protocol was performed to add multiplexing indices to the first amplicons (forward and reverse “Nextera XT” primers, Illumina, San Diego, CA, USA). The Master Mix KAPA Uracil plus (Roche, Basel, Switzerland) was used for the second amplification and the PCRs were performed with the following temperature conditions: 95 °C for 3 min; 12 cycles of denaturation at 98 °C for 20 s; annealing at 55 °C for 30 s: and elongation at 72 °C for 50 s and 72 °C for 5 min. Both PCR steps were followed by purification using magnetic Beads (Beckman-Coulter, Brea, CA, USA) according to the manufacturer’s instructions. All amplicons were quantified using a Qubit 2.0 fluorometer. An equimolar amplicon library was generated and then diluted to a final concentration of 8 pM. Phix control library (Illumina) [10% (v/v)] was added to increase diversity of base calling during sequencing. The library was subjected to sequencing using V2-nano reagent kits on the Illumina MiSeq system (Illumina).
Statistical analysis
Continuous variables were reported as median (50th percentile) and interquartile interval (IQI, 25th and 75th percentiles). Discrete variables were reported as the number and proportion of subjects with the characteristic of interest. The main outcome, i.e., the proportion of children with overweight or obesity at 24 months, was analyzed using the prespecified Pearson’s Chi-square test (see sample size calculation). We also calculated the risk difference and its 95% confidence using a binomial regression model (BRM) having the proportion of children with overweight or obesity as the response variable, and treatment (discrete: 0 = CT; 1 = MD) as the predictor variable (ITT and PPA). We evaluated the influence of baseline maternal weight or BMI on the risk difference by adding them as covariables to the BRM (PPA). Other outcomes, i.e., maternal adherence to treatment and weight gain during pregnancy were analyzed using random effect linear regression (RELR) models (PPA). To this aim, MedDiet Score (continuous, score) or maternal body weight (continuous, kg) was the response variable, treatment (discrete: 0 = CT; 1 = MD); trimester (discrete: 0 = 1st trimester; 1 = 2nd trimester; 2 = 3rd trimester), a treatmentXtime (discreteXdiscrete) interaction were the predictors (PPA), and the mother was the random effect [24]. We evaluated the influence of baseline maternal weight or baseline maternal BMI on weight gain by adding it as covariable to the RELR model (PPA). Three Bonferroni corrected between-group (MD vs. CT) within-time (1st, 2nd and 3rd trimester) contrasts were calculated. The between-group differences in the methylation of the leptin gene were analyzed using unpaired Student’s t-test. Statistical analysis was performed using Stata 18.5 (Stata Corporation, College Station, TX, USA) and GraphPad Prism 7.0 (GraphPad Software, San Diego, CA, USA).





留言 (0)