
記住我









Eighty-nine patients received TBI-based conditioning before 1st allo-HSCT. Table 1 summarizes transplant characteristics. Median patient age at TBI was 42.5 years (IQR, 32.5–51.2). The median follow-up time was 15.2 years (IQR, 13.0-18.2).
Table 1 Patients characteristics (n = 89)Most patients (n = 47) received a myeloablative conditioning (MAC) regimen containing 8 Gy TBI. Reduced-intensity conditioning (RIC) regimens comprising 4 Gy TBI were applied in 31 patients, while eleven patients received MAC with 12 Gy TBI (Table 2). The median age of patients receiving RIC (4 Gy) and MAC (8–12 Gy) was 50.7 years (IQR, 41.0–59.0) and 38.9 years (IQR, 29.7–45.1). This difference was statistically significant (P < 0.001). ELN genetic risk classification was similar between RIC and MAC groups (P = 0.443), while the distribution of disease status at allo-HSCT was different (P < 0.001). Fifteen patients receiving RIC were in > 2nd complete remission (including refractory AML), while 11 patients receiving MAC were in > 2nd complete remission (including refractory AML). Most patients receiving MAC were in first complete remission (n = 28), while only 3 patients receiving RIC were in first complete remission at allo-HSCT. PR1 and CR2 were present in 13 patients receiving RIC and 19 patients receiving MAC.
Table 2 Conditioning regimens before allo-HSCT (n = 89)Chronic graft-versus-host diseaseTwo-year and 5-year cumulative incidences of cGVHD requiring systemic immunosuppression were 33% (95%CI, 23–42) and 36% (95%CI, 26–46). Twenty-nine patients had a history of grade II-IV aGVHD without cGVHD (requiring systemic immunosuppression), while 26 patients had neither aGVHD nor cGVHD. Eighteen patients had a history of aGVHD and cGVHD, while 16 patients had a history of cGVHD without prior aGVHD. Severe cGVHD was the most frequent maximum grade of cGVHD (n = 17) while twelve patients had moderate cGVHD, and five patients had mild cGVHD. Most patients had three or more cGVHD organ sites (median 3, IQR, 2–4). The most common sites of cGVHD in patients suffering from cGVHD were the skin (n = 24), oral mucosa (n = 20), eyes (n = 14), and liver (n = 11). The cumulative incidences of cGVHD (requiring systemic immunosuppression) in patients receiving RIC and MAC were similar over the entire follow-up period (P = 0.91). Two-year and 5-year cumulative incidences of cGVHD were 35% (95%CI, 19–53) and 39% (95%CI, 21–56) in patients receiving RIC, while patients receiving MAC showed 2-year and 5-year cumulative incidences of cGVHD of 31% (95%CI, 20–43) and 34% (95%CI, 22–47), respectively.
Secondary malignanciesTable 3 shows details of all secondary solid malignancies and precancerous lesions in 89 patients. Patient no. 290 was diagnosed with a pleomorphic undifferentiated sarcoma which appeared within less than a year after TBI. It was assumed that the sarcoma was present at the time of allo-HSCT. Therefore, this patient was excluded from further analyses resulting in 88 patients.
Table 3 Secondary solid malignancies and precancerous lesions after total body irradiation-based conditioning (n = 89)The cumulative incidences of secondary solid malignancies and precancerous lesions were 8% (95%CI, 4–16), 14% (95%CI, 7–23) and 17% (95%CI, 9–27) at 10, 15 and 20 years, while the cumulative incidences of premature deaths were 59% (95%CI, 48–69), 59% (95%CI, 48–69), and 64% (95%CI, 49–76), respectively. Seven patients developed at least one non-SCC. The most common non-SCCs were cutaneous basal cell carcinomas of the face, while two male patients developed thyroid cancers. The mean time from allo-HSCT to the development of the first non-SCC was 10 years (95%CI, 7–14). Four secondary SCCs occurred in 3 patients. Cutaneous SCCs were the most frequent SCCs. The mean time from allo-HSCT to the first SCC was 10 years (95%CI, -7-27).
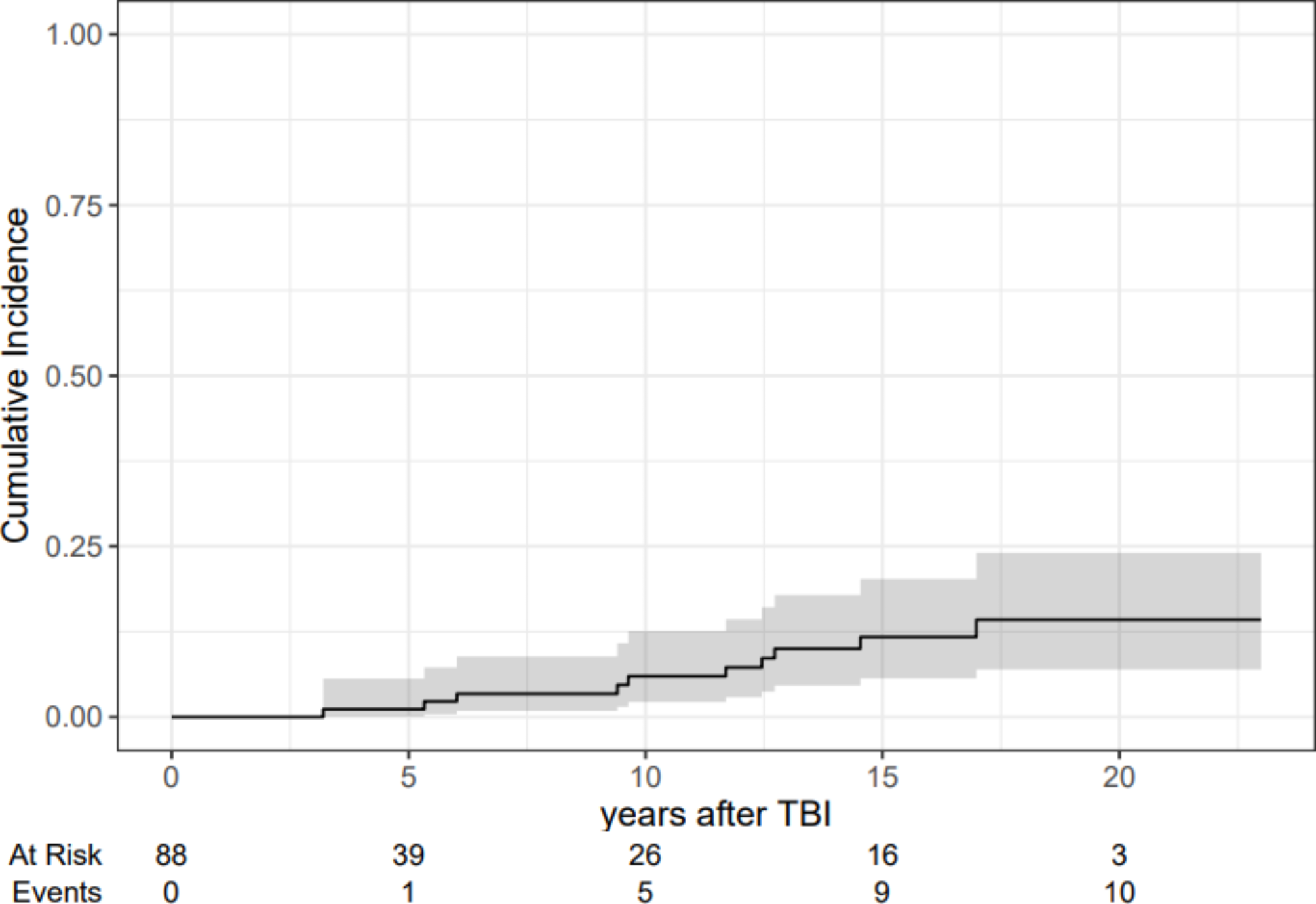
Figure 1 shows the estimates of the cumulative incidences of secondary solid malignancies with 95% confidence intervals treating premature deaths among patients who did not develop secondary solid malignancies as competing risks. The cumulative incidences of secondary solid malignancies were 6% (95%CI, 2–13), 12% (95%CI, 6–20), and 14% (95%CI, 7–24) at 10, 15 and 20 years.
Fig. 1
Estimates of the cumulative incidences of secondary solid malignancies with 95% confidence intervals (n = 88)
The cumulative incidences of invasive non-SCCs were 4% (95%CI, 1–9), 10% (95%CI, 4–18), and 9% (95%CI, 4–18) at 10, 15 and 20 years. The cumulative incidences of invasive SCCs were 2% (95%CI, 1–8), 2% (95%CI, 1–8), and 5% (95%CI, 1–14) at 10, 15 and 20 years, respectively.
The cumulative incidences of relapse at 5, 10 and 15 years were 43% (95%CI, 33–53), 44% (95%CI, 34–54) and 44% (95%CI, 34–54), while the cumulative incidences of non-relapse mortality (NRM) were 16% (95%CI, 9–24), 18% (95%CI, 11–27) and 18% (95%CI, 11–27), respectively.
Hazard models for secondary solid malignancies and precancerous lesions and the competing risks of premature deathsTable 4 shows the cause-specific hazards (HR CS) for secondary solid malignancies and precancerous lesions and the competing risks of premature deaths. In the multivariate regression models, older age at TBI translated into lower rates of secondary malignancies/precancerous lesions (HR cs 0.95, 95% CI, 0.90-1.00; P = 0.043). The analysis of competing events revealed that older patients showed a trend towards premature deaths (deaths before they could develop secondary malignancies/precancerous lesions, HR cs 1.02, 95%CI, 1.00-1.05; P = 0.069). Higher TBI doses (mainly applied in younger patients) translated into reduced rates of secondary malignancies/precancerous lesions (HR cs 0.76, 95% CI, 0.59–0.98; P = 0.035) while lacking associations with premature deaths. Chronic GVHD translated into increased rates of deaths before patients could develop secondary malignancies/precancerous lesions (HR cs 8.04, 95%CI, 3.97–16.3; P < 0.001).
Table 4 Cause-specific hazards (HR CS) for secondary malignancies/precancerous lesions and the competing risks of premature deaths (n = 88)
留言 (0)