
記住我







This retrospective study was institutional review board-approved and performed in a Health Insurance Portability and Accountability Act-compliant manner. The need for informed consent was waived.
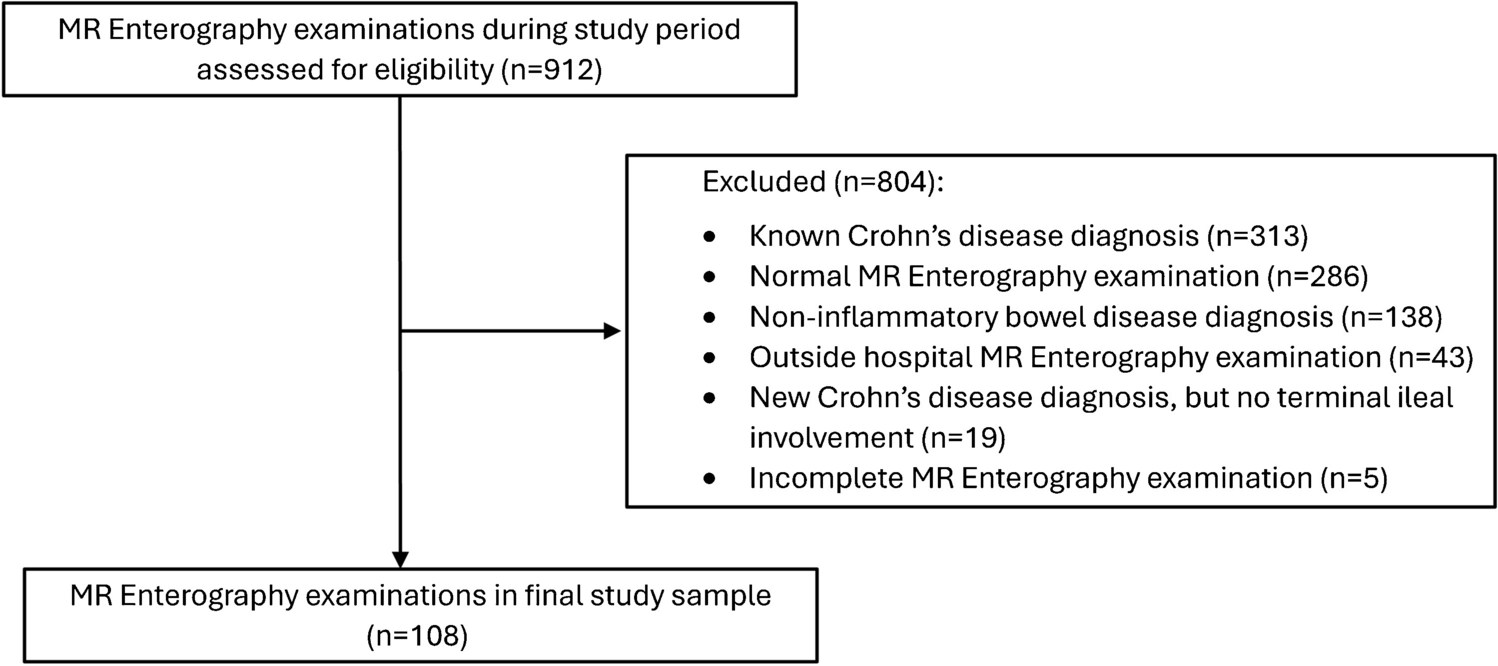
Using a review of institutional electronic health records, consecutive pediatric patients (ages 6 years to 18 years) with newly diagnosed ileal CD that underwent a clinical MRE examination prior to medical treatment initiation between January 1, 2021, and December 31, 2022, were identified. Patients without a clinical diagnosis of CD in the electronic health record, including endoscopic and histologic confirmation of ileal CD, were excluded as were patients with incomplete MRE examinations and MRE examinations performed at outside institutions. A participant flow diagram is presented in Fig. 1.
Fig. 1
For each participant included in the final study sample, demographic and anthropometric data were recorded. Clinical markers of intestinal active inflammation also were recorded from the time of ileal CD diagnosis, including C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), albumin, hematocrit, and fecal calprotectin. All laboratory data was obtained within 3 months of the MRE examination. In patients that underwent repeated laboratory testing, the values closest to the date of the MRE examination were documented. Clinical MRE and endoscopy reports were used to phenotype participants based on disease location and the presence of stricturing and internal penetrating disease. In addition, clinical endoscopy reports were used to document the diagnostic adequacy and the presence of ulcers (e.g., superficial, deep, linear) involving the terminal ileum; participants with erosions and aphthous lesions by endoscopy were considered to be negative for ulcers for the purposes of this study.
Pertinent clinical MRE examinations were independently reviewed by three fellowship-trained, board-certified pediatric radiologists (26 years, 16 years, and 4 years post-fellowship experience). Study radiologists were blinded to one another and were not provided any additional clinical (e.g., laboratory or endoscopic) data. All MRE examinations included a combination of axial and coronal single-shot fast spin-echo without and with fat suppression, axial diffusion-weighted, and axial and coronal contrast-enhanced T1-weighted sequences based on our institutional clinical MRE imaging protocol (which remained unchanged during the study period) (Supplemental Table). MRE images were acquired following the ingestion of oral contrast material (Breeza; Beekley Corporation, Bristol, CT) using weighted-based dosing (20 ml/kg, up to 1,000 ml).
Each study radiologist assessed the terminal ileum (defined as the distal 15 cm of the small bowel, including the ileocecal valve, for the purposes of this investigation) and documented the following MRI findings for each MRE examination:
Presence vs. absence of radiologic ulcers (yes/no), defined as a mucosa-based defect in the bowel wall filled with oral contrast material or enteric contents (Figs. 2 and 3);
Severity of radiologic ulcers – classified based on the most severe ulcer (none, depth < 50% bowel wall thickness, or depth > 50% bowel wall thickness, scored as 0–2);
Extent of radiologic ulcers (none, mild [1–2 ulcers], moderate [3–5 ulcers], or severe [6 or more ulcers], scored as 0–3);
Maximum single bowel wall thickness in mm; and
Length of disease in cm (maximum 15 cm).
Fig. 2
Examples of radiologic ulcers from two different children with newly diagnosed ileal Crohn disease. A Axial T2-weighted single-shot fast spin-echo MR image with fat suppression from a 12-year-old boy shows both deep (long arrow) and superficial (short arrow) radiologic ulcers. The terminal ileum appears thick-walled with mural edema. B Axial T2-weighted single-shot fast spin-echo image without fat suppression from a different 12-year-old boy shows multiple superficial radiologic ulcers (arrows). The terminal ileum appears thick-walled with mural edema. All three study radiologists indicated the presence of radiologic ulcers in these two children as well as agreed on severity (i.e., ulcer depth)
Fig. 3
A 15-year-old with a family history of Crohn disease and new perianal drainage. A Coronal T2-weighted single-shot fast spin-echo, (B) axial T2-weighted single-shot fast spin-echo, (C) axial T2-weighted single-shot fast spin-echo fat-saturated, and (D) axial postcontrast T1-weighted MR images show findings consistent with ileal Crohn disease, including multiple radiologic ulcers (arrows) of variable depth and severe in extent (6 or more visible ulcers)
Multiple unique examples of radiologic ulcers meeting the above study definitions on both noncontrast and contrast-enhanced MR sequences were assembled by a fourth radiologist (15 years post-fellowship experience) and shared with the study radiologists prior to their imaging review to serve as a training aid.
Statistical analysesContinuous data were summarized as means and standard deviations, while categorical data were summarized as counts and percentages. Student’s t-test (two-sided) was used to compare continuous variables between groups, while Fisher’s exact test was used to compare categorical variables between groups. Pearson’s and Spearman’s rank-order correlation coefficients were used to evaluate associations between variables, as appropriate. The consensus among the three study radiologists was used to categorize patients into two groups, patients without and patients with radiologic ulcers (with either all three or two of three study radiologists agreeing on their absence vs. presence). Mean maximum bowel wall thickness, mean length of disease, and mean extent of ulcers among the three study radiologists were used for correlation testing. The diagnostic performance (sensitivity, specificity, positive predictive value, and negative predictive value) of MRE for diagnosing ulcers (based on study radiologist consensus) was also determined using the presence of ulcers at clinical endoscopy as the reference standard.
Inter-radiologist agreement was assessed using Fleiss’ kappa (k) statistics, with weighted kappa statistics calculated for ordinal variables (e.g., extent of ulcers). Kappa statistics were interpreted as follows: < 0 = no agreement; 0–0.20 = slight agreement, 0.21–0.40 = fair agreement, 0.41–0.60 = moderate agreement, 0.61–0.80 = substantial agreement, and 0.81–1 = almost perfect agreement [7].
A P-value < 0.05 was considered significant for all inference testing. Statistical analyses were performed using MedCalc® Statistical Software version 20.111 (MedCalc Software Ltd, Ostend, Belgium).
留言 (0)