
記住我
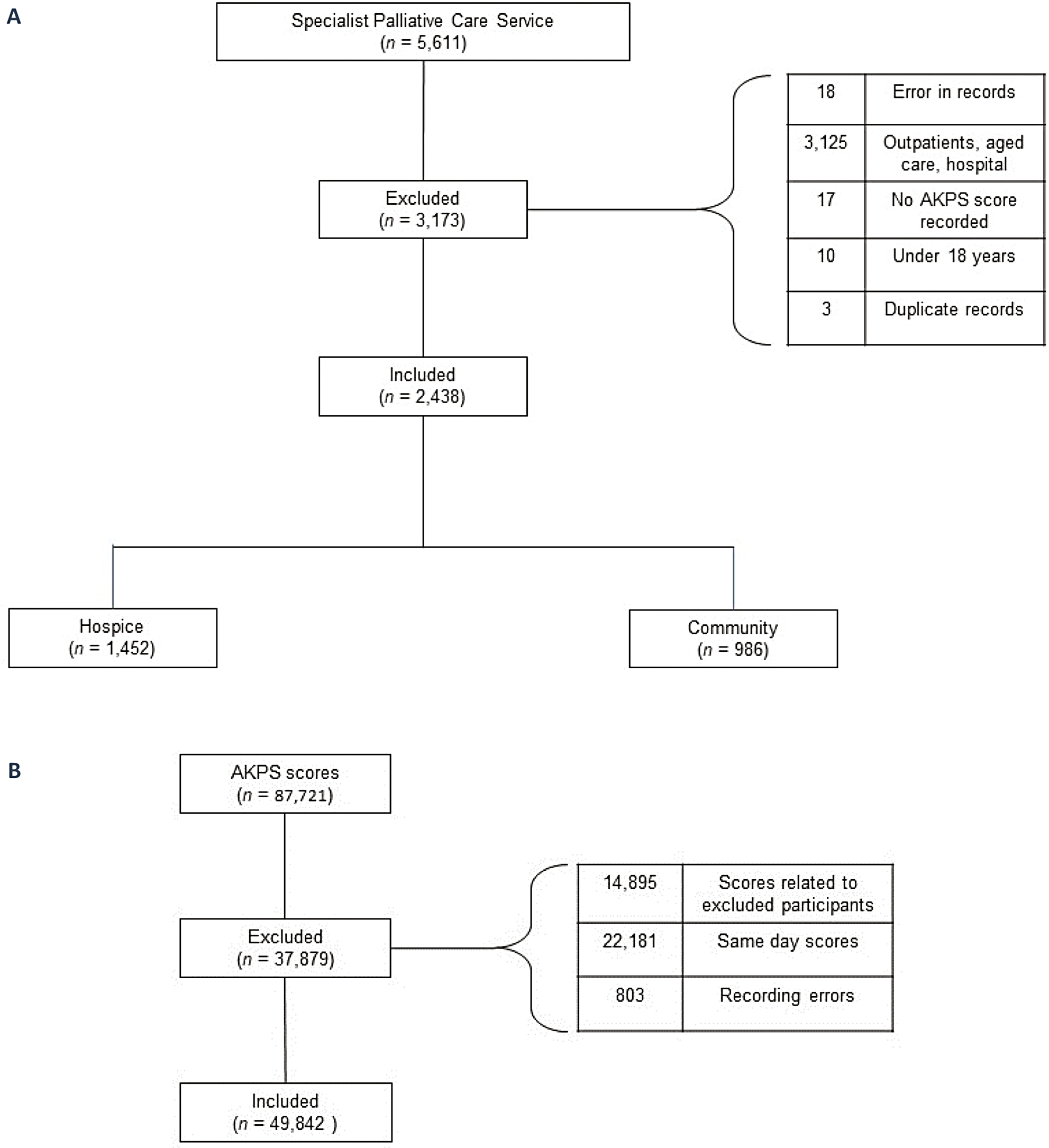
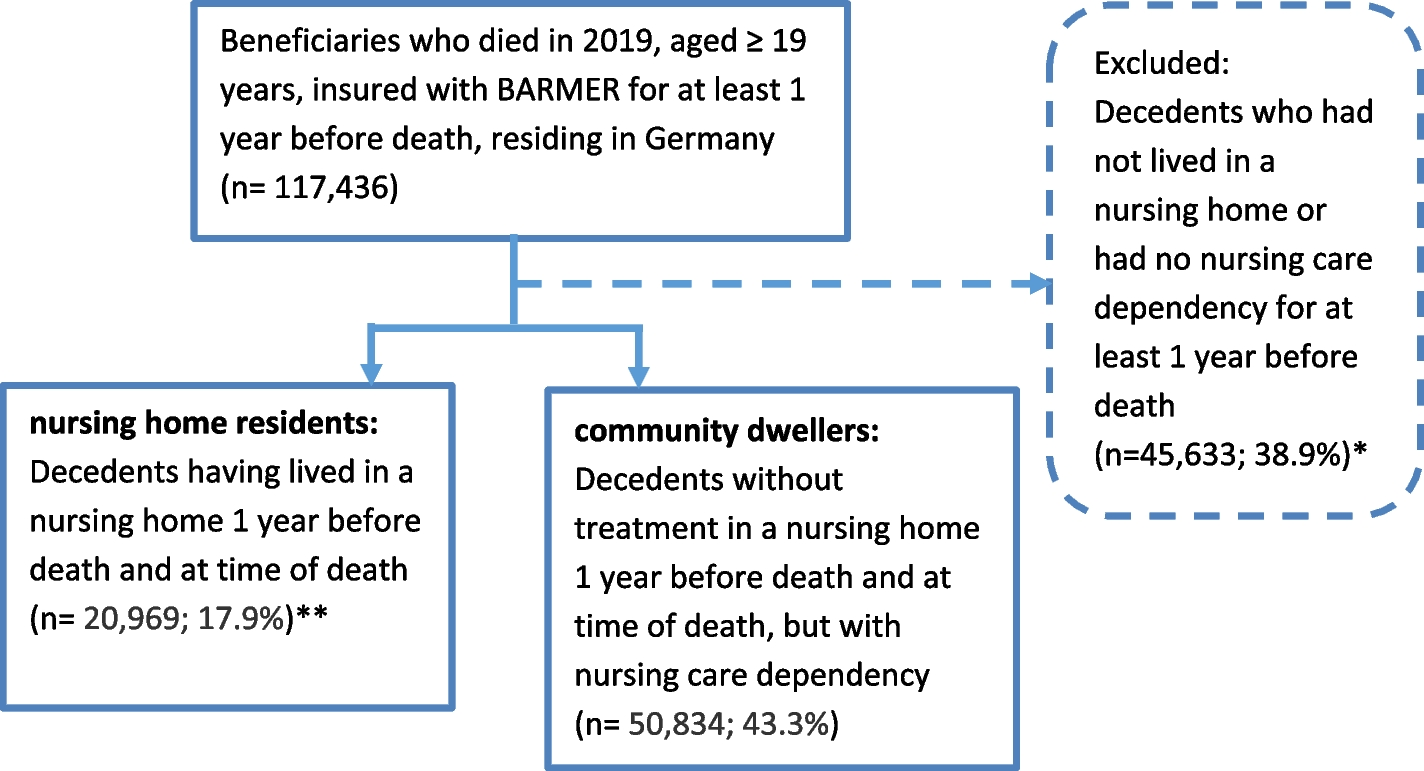




Initial database searches after de-duplication identified 2059 results. From these, 254 potentially eligible studies were identified and screened as full texts (Fig. 1). Eight papers were identified for inclusion. Thirteen additional sources were identified from reference and citation searches, and one from the grey literature search. Due to the additional papers identified we discussed with an information expert our search sensitivity; however, many of the additional papers were not indexed under the search terms used and would not have appeared in searches. Our search was very broad as seen in the Appendix. We discuss challenges of identifying relevant literature in the databases in the discussion. Updated searches identified 497 results, with 38 papers screened as full texts. From these, one paper was identified for inclusion. Twenty-three sources reporting on 20 different studies were included in the qualitative analysis.
Fig. 1
PRISMA flowchart of search process
The number of articles published on this topic has increased substantially over time – 18 of the 23 were published in the last 10 years, with years of publication ranging between 1995 and 2023. Nineteen papers used purely qualitative methods [11, 15, 16, 19, 20, 34,35,36,37,38,39,40,41,42,43,44,45,46,47] and four used mixed methods [48,49,50,51]. The mean number of participants recruited was 31 (range 1–100). The mean age of people receiving palliative or end of life care was 77 years. Characteristics of included papers are summarised in Table 1.
Table 1 Characteristics of included sourcesAs can be seen in the table, there were many different ways in which ethnicity was described, some of which represent the time in which the studies were undertaken. For example, CALD may now potentially viewed as outdated.
We grouped the findings across the included studies into seven overarching themes were: (1) Knowledge of hospice and palliative care, (2) societal and structural issues, (3) language and health literacy, (4) migratory experiences, (5) trust in healthcare services and professionals, (6) religion and hope, and (7) cultural values. Barriers and facilitators for accessing and utilising care were explored through each theme.
Knowledge of hospice and palliative careUnderstanding of palliative and end of life care was generally limited among Black and African-Caribbean carers, migrants, and CALD (culturally and linguistically diverse) patients [35, 36, 38, 47]. Part of this may be due to there being no equivalent term for ‘palliative care’ in many cultures and languages [36]. A lack of understanding and limited health literacy, especially where there was limited English skills among Hispanic and Latino participants, impaired their ability to seek help, navigate the healthcare system, and make informed decisions [34, 37, 39]. Many participants learned about hospice for the first time at the time of the referral [45, 46]. Participants often had a limited understanding of hospice and the changes in goals of care (i.e., from curative to comfort care) it represented, and were not well-aware of the connection between hospice referral and disease prognosis [11, 15, 36, 46, 49]. Some participants viewed hospice as a support if their health declines further in future, despite currently receiving hospice services [46]. Others viewed hospice as a break before returning to curative treatment [41, 45]. Positive past experiences with hospice, learning about hospice care through seeing older relatives go through it, or recommendations from friends helped carers access hospice [45, 49].
Understanding the potential risks associated with life-sustaining treatments were reported to be important for Hispanic carers making end of life decisions, with carers wanting healthcare professionals to explain end of life treatment options, including purpose, goals, and limitations. Despite the discomfort surrounding the topic of hospice care, carers emphasised the importance of talking about the benefits of hospice care [15]. This was supported by families’ concerns around medication use toward the end of life being dispelled through nurses providing explanations [44, 50].
Patients’ and carers’ insight into their own or their family member’s health status also enabled them to make end of life decisions. Patients who were aware about their declining health or their conditions being unlikely to respond to medical treatment were more likely to accept recommendations to enrol in hospice, despite having little to no previous knowledge of hospice [45, 49].
Societal and structural issuesHospice care and other end of life support held a stigma among Black African-Caribbean, African American, and Chinese American communities, seen as giving up on or not wanting to take care of someone [35, 39, 41, 43]. Stigma around dementia also resulted in later diagnosis and reluctance to seek additional support [16]. Talking about end of life, prognosis, palliative care, or hospice care was often suppressed among people from minority ethnic groups, and may cause feelings of discomfort or offence when mentioned [11, 15, 19, 20, 36, 38, 39, 50]. Healthcare professionals working with South Asian patients with kidney disease in the UK reported that not all of their colleagues agreed with discussing end of life and advance care planning with patients [37].
Institutional racism, and the risk of discrimination and mistreatment within healthcare systems was a concern for African American participants; some of whom felt that they were “second-class patients” due to experiences of differential treatment and stereotyping from healthcare professionals [43]. Structural barriers to accessing care included lack of health insurance or living in poverty [43].
Latino and Hispanic participants in the USA reported feeling uncertain about who was being billed for services received, and therefore hesitating to request more services despite needing them [46]. Carers suggested that healthcare professionals should recognise that many African American people experience substantial financial difficulties.11 Health insurance coverage of hospice care facilitated access for African American patients with low income [49].
African American patients and carers valued assistance from health and social care professionals, for instance, help from hospice staff when completing hospice enrolment paperwork [49]. Social workers also helped carers make end of life care decisions by explaining treatment options, arranging meetings with healthcare professionals, advocating for families, and supporting effective communication between family members and their dying relatives, as well as with each other.20
Language and health literacyLanguage barriers were reported across many papers. Latino and Hispanic patients and carers highlighted a need for more Spanish-speaking healthcare professionals and materials in Spanish [19, 34, 46]. Healthcare professionals reported that South Asian patients also experienced poorer access to care due to language barriers [37]. Particular language difficulties reported by nurses and patients included adequately assessing and managing pain without interpreters [36, 50], supporting patients and families coming to terms with dying [44], and processing information about prognosis and treatment in a foreign language while suffering from distressing symptoms [38]. This can be exacerbated for people with dementia who speak English as a second language, as they may lose their English ability as well as their ability to communicate as the disease progresses [16].
Latino and Hispanic participants faced health literacy difficulties that hindered their ability to communicate with medical providers; for example, using medical terms incorrectly [46]. CALD patients with cancer had difficulties communicating with clinicians about treatment expectations [36]. Black and Hispanic carers believed that the lack of end of life communication from healthcare professionals, such as about worsening prognosis, impeded end of life care planning and decision-making; [15, 47] for example, hospice referral happening too late because the physician did not discuss hospice with carers [43]. Black and African American carers also felt they could have been better informed concerning treatments and outcomes [20, 47].
Migratory experiencesA study with Hispanic and Latino participants who had migrated to the USA found many carers were previously not exposed to issues around ageing and dying as they did not have elderly relatives nearby, limiting opportunities to learn from family members. These experiences, as well as low education levels, resulted in participants feeling limited in their ability to seek out and understand health information and services. Terminally ill Latino and Hispanic people had limited access to healthcare in their countries of origin, and once in the USA, continued to have few interactions with healthcare prior to being diagnosed with their terminal illness. This limited interaction with medical providers led to participants rarely discussing their preferences with clinicians and instead following doctors’ orders [46].
Migrant patients in Germany experienced feelings of not belonging, which led to difficulties towards the end of life, such as experiencing less support from neighbours and the local community than in the country of origin, and regrets around moving.39 These feelings of interpersonal disconnect may discourage migrant patients from seeking or using palliative care services.
Trust in healthcare services and professionalsTrustworthy information was important and acted as a facilitator to accessing care, with recommendations from friends, neighbours, and spiritual leaders being the main influence on decision making [43, 47]. There was distrust of health and care systems and physicians among Black, African American and Hispanic carers [11, 47], including refusing support from services [34] and feeling misled by doctors due to not understanding medical terminology [39]. African American patients and carers were sceptical of advice offered by healthcare professionals due to previous reports of being treated badly [43]. Carers recommended that clinicians work to establish trust while understanding their distrust of care and the medical system, and recognising the historical and social reasons for this, including slavery, racism, medical experimentation and exploitation [11].
Black and African American patients and carers are more likely to trust staff members of their community [47] and found the lack of Black hospice care workers frustrating [11, 39]. Nurses working with immigrant patients reported that trust is particularly important, and that it can be easy to lose the trust of patients and their families. They suggested building a trusting relationship by getting to know the patient and their family, and not rushing conversations about dying. Nurses reported using qualified health interpreters and having a multicultural workforce were valuable for working with immigrants [44].
Latino and Hispanic carers reported trusting doctors perceived to be knowledgeable and adept. However, those with limited health literacy had no option other than to trust doctors [46, 51]. Healthcare professionals investing time in understanding patients’ beliefs about dementia resulted in a better understanding of cultural barriers and facilitators in accepting support, and promoted trust in the relationship [16].
Religion and hopeReligion was seen as a facilitator in end of life decision making. Many Black, African-Caribbean and African American carers indicated that their faith, religious beliefs, or pastoral counselling was an important resource in making end-of-life care decisions for their family member [20, 35, 47]. African American carers suggested that healthcare professionals invite their pastors to prognosis discussions and understand the role of religion and church in their lives [11]. Latino patients were similarly guided by God and religion, and end of life treatment discussions often involved a spiritual or religious leader [34, 51]. Religion also caused barriers to accessing care. For example, African American carers were reluctant to enrol their family member in hospice care because they felt that doing so reflected a lack of trust in God [43]. However, others felt that God was sending them hospice or healthcare professionals [41,
留言 (0)