
記住我

Pulse pressure (PP) amplification (PPA), also referred to solely as pulse amplification, means the phenomenon that PP amplifies (widens gradually) as the pulse wave travels from the central aorta to peripheral muscular arteries along the arterial tree [1]. PPA is virtually synonymous with systolic blood pressure (BP) amplification, because diastolic (and mean) BP remains constant between the central and peripheral arteries [2].
The phenomenon of PPA is attributable to non-uniformity of elastic wall properties in the arterial system. Normally, as going down from the elastic aorta to muscular arteries, the arterial wall not only becomes thinner but also gradually stiffens since the elastin/collagen fiber ratio decreases in the medial layer and the smooth muscle cell content increases accordingly. Arterial stiffness (S) is, by definition, a change in BP (ΔP) for a given change in blood volume (ΔV): S = ΔP/ΔV. Therefore, PP becomes wider as arterial wall is stiffer, if inflow and outflow are the same between different arterial sites. Central-to-peripheral PPA is thus accounted for by the stiffness difference (namely, a positive stiffness gradient) between the more elastic aorta and stiffer muscular arteries. PPA is also influenced by peripheral wave reflection that causes late-systolic BP augmentation [3], because the boosting effect on peak systolic BP is more pronounced in the central than peripheral arteries. There is indeed a reciprocal (inverse) relationship between PPA and the augmentation index (AIx).
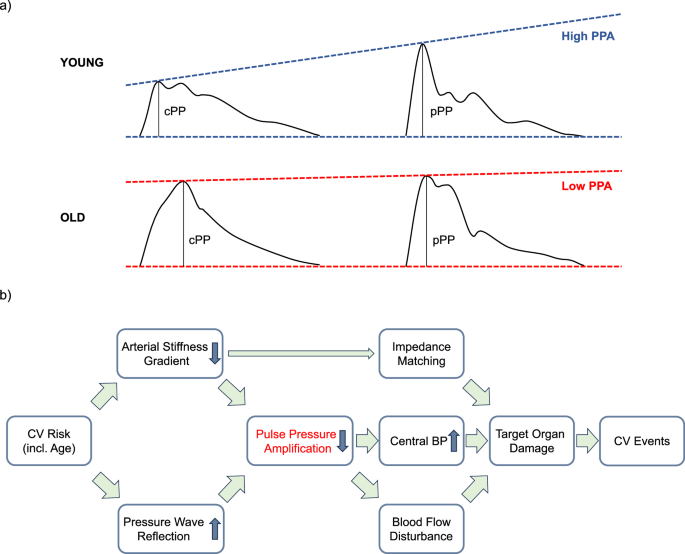
PPA decreases progressively with age (Fig. 1a). Brachial PP in young adults can be 50% greater than aortic PP, whereas in elderly people the brachial and aortic PP are nearly equal (in other words, PPA approaches 0%). The decreased PPA in the elderly is attributed both to a selective stiffening of the central aorta without accompanying elevation of peripheral artery stiffness, and to an increased pressure wave reflection from the periphery [4]. Previous studies demonstrated a marked increase in aortic pulse wave velocity (PWV) with age in contrast to a much more gradual change in brachial PWV [5], indicating that the brachial/aortic PWV ratio (namely, the central-to-peripheral stiffness gradient related to PPA) decreases or even becomes less than unity (<1) with aging. Such a close association with age suggests PPA as a potential biomarker of (early) vascular aging. PPA is also known to increase on physical exercise [6] and with increasing heart rate, in consequence of peripheral vasodilation and decreased late-systolic BP augmentation, respectively.
Fig. 1
a Comparison of PPA between young and old subjects. Note that, despite similar peripheral PP (pPP), the old subject has higher central PP (cPP) than the young subject because of lower PPA. b Potential mechanism linking PPA to cardiovascular (CV) disease
In the current issue of Hypertension Research, Huang et al. [7] reported the predictive ability of PPA for cardiovascular and coronary events in a prospective cohort of 3945 individuals based on the IDCARS database. Aortic pulse waveforms were generated from radial waveforms using a generalized transfer function, and PPA was quantified as the ratio of brachial to aortic (central) PP. The results showed a significant and independent predictability of the PPA ratio for both events with the best cut-off value (threshold) of 1.3. Of high-risk individuals (with PPA of <1.3) younger than 60 years, 67.7% were women, potentially reflecting a higher AIx in women than in men. They concluded PPA to be a forerunner of cardiovascular/coronary complications over and beyond traditional risk factors.
The study by Huang et al. [7] may have two important implications for optimal BP measurement. First, BP should preferably be evaluated at two different arterial sites (namely, central and peripheral), whenever available. The results of this study imply that an individual with a higher central BP is at higher risk of cardiovascular disease than an individual with a lower central BP, even if both individuals have an identical brachial BP. The prognostic significance of PPA as demonstrated by this study provides evidence in favor of clinical usefulness of central BP as routine measurement. Second, BP waveform recording can add useful information on cardiovascular risk assessment to usual BP measurement with a cuff sphygmomanometer. Of note, the radial/aortic PPA ratio can be readily estimated from the radial waveform alone using non-invasive applanation tonometry and a generalized transfer function, even without using brachial cuff sphygmomanometry [8].
It may be worthwhile here discussing the potential mechanisms responsible for the detrimental effect of reduced PPA on cardiovascular integrity (Fig. 1b). Previous studies have associated PPA not only with hard endpoints as shown in the current study but also with surrogate endpoints (such as left ventricular hypertrophy [8] and renal resistive index [9]), which are identical to target organ damage/dysfunction caused by hypertension. First, these significant associations are likely in some part because central BP (and PP) corresponds to the pressure exerted at the level of the heart, brain and kidney. The central PP cannot be assessed accurately by peripheral PP alone, but it is predictable precisely by considering PPA. Second, PPA is a potential measure of arterial stiffness gradient between central and peripheral arteries. Diminished stiffness gradient, which reduces PPA, leads to impedance matching, causes higher pulsatile stress to penetrate deeply into fragile microvasculature of peripheral vasodilated organs, and predisposes to microvascular damage [10]. Lastly, PPA is linked to pulsatile blood flow. PPA produces an instantaneous BP gradient between the proximal and distal arteries, as shown in an invasive study on simultaneous measurements of aortic and radial BP waveforms [6]. The BP gradient is known to generate instantaneous blood flow, and therefore PPA can contribute to the production of flow pulse waveform [4, 11]. Indeed, PPA is related to the magnitude of oscillatory flow fluctuation consisting of late-systolic reverse and early diastolic forward flows in peripheral arteries [11]. Previous studies have shown that decreased aortic-to-leg PPA in patients with stiffened aorta is associated with reduced reverse flow in the femoral artery [12], and the latter is linked to higher renal resistive index [9] and reduced glomerular filtration rate [13]. Taken together, these results indicate that PPA serves as a unique hemodynamic parameter containing integrated information on both pulsatile BP and flow as well as arterial stiffness gradient.
In agreement with previous relevant studies, the current investigation [7] demonstrated clinical usefulness of PPA measurement in a large population. In the future, PPA could be utilized not only as a prognostic marker for risk stratification but also as a therapeutic guide for treatment of hypertension. PPA can be normalized at least in part by effective antihypertensive vasodilator treatment [8, 14]. Normalization of PPA can potentially retard the progression (or even facilitate the regression [8]) of damage and dysfunction in target organs, and it may thereby help to improve cardiovascular outcome of hypertension [14]. Further investigation is required to verify this possibility.
留言 (0)