
記住我
Carbapenemase-producing Klebsiella pneumoniae strains (CP-Kps) have spread rapidly around the world (Guo et al., 2023). The European Antimicrobial Resistance Surveillance Network (EARS-Net) of the European Centre for Disease Prevention and Control (ECDC) have recently reported a rate of 24.9% for carbapenem-resistant Klebsiella pneumoniae (Kp) isolates in Italy (European Centre for Disease Prevention and Control, 2023). New Delhi metallo-β-lactamase (NDM) is able to hydrolyse almost all β-lactams, including carbapenems. Since its 2008 discovery from a Kp strain isolated from a patient repatriated to Sweden after hospitalization in New Delhi, NDM-positive strains have been causing healthcare-associated outbreaks worldwide (Wu et al., 2019).
In Italy, the first outbreak of NDM-producing Kp (November 2018-May 2019) was documented in the northwestern area of Tuscany. This outbreak, involving nine different hospitals and 350 patients, was mostly caused by an NDM-1-producing Kp clone of ST147 (European Center for Disease Prevention and Control, 2019; Di Pilato et al., 2022).
Here, we report the identification of a blaNDM-5 and blaOXA-232 producing Kp clone of ST437, isolated for the first time from a patient hospitalized in a healthcare setting in Abruzzo region, Southern Italy.
2 Case presentationIn April 2023, an 85-year-old Italian male patient was admitted to the hospital with a proximal femoral fracture, and underwent emergency surgery. The patient had comorbidities, particularly senile dementia associated with Parkinsonism, arterial hypertension, and a second stage sacral pressure ulcer due to reduced mobility.
On the 9th day after surgery, the patient developed fever and hypotension due to elevated lactate and procalcitonin levels (73 ng/ml). Blood and urine samples were collected, and empirical antibiotic treatment with meropenem 500 mg Q12H IV and vancomycin 1000 mg Q24H IV (renal impairment dosing) was initiated. On the 48th hour, a suspected Kp strain was detected in both blood and urinary cultures. The isolate (Kp1) was identified as Klebsiella pneumoniae by matrix assisted laser desorption ionization-time of flight (MALDI-TOF) mass spectrometry using Vitek MS (Biomérieux, Marcy l’Étoile, France). Carbapenemase genes were screened using the Amplex Eazyplex SuperBug CRE test (Amplex Diagnostics, Gars am Inn, Germany) based on the loop-mediated isothermal amplification (LAMP) method. The blaKPC and blaCTX-M1 genes were also detected).
The antimicrobial susceptibility test (AST) was performed using the MicroScan WalkAway system DxM 1096 (Beckman Coulter), and the results were interpreted according to the guidelines of the European Committee on Antimicrobial Susceptibility Testing (EUCAST, 2023, version 13.1). Since the breakpoint of tigecycline against Kp has not been made available by EUCAST, the EUCAST breakpoint for E. coli was used. Cefiderocol (FDC) susceptibility was tested using Minimum Inhibitory Concentration (MIC) Test Strip (Liofilchem, Roseto degli Abruzzi, Italy), and interpreted according to EUCAST clinical breakpoints. FDC is a novel injectable siderophore cephalosporin that is active against most carbapenem-resistant Enterobacteriaceae and is used for the treatment of complicated urinary tract infections, hospital-acquired bacterial pneumonia, and ventilator-associated bacterial pneumonia (Wu et al., 2020).
The results indicated that a modification to the antibiotic therapy may be required (Table 1). Hence, ceftazidime/avibactam (CZA) 2.5 g Q8H IV treatment was initiated against carbapenem-resistant Kp (Tumbarello et al., 2019). The patient’s clinical condition improved rapidly after microbiological eradication (negative blood and urine cultures).
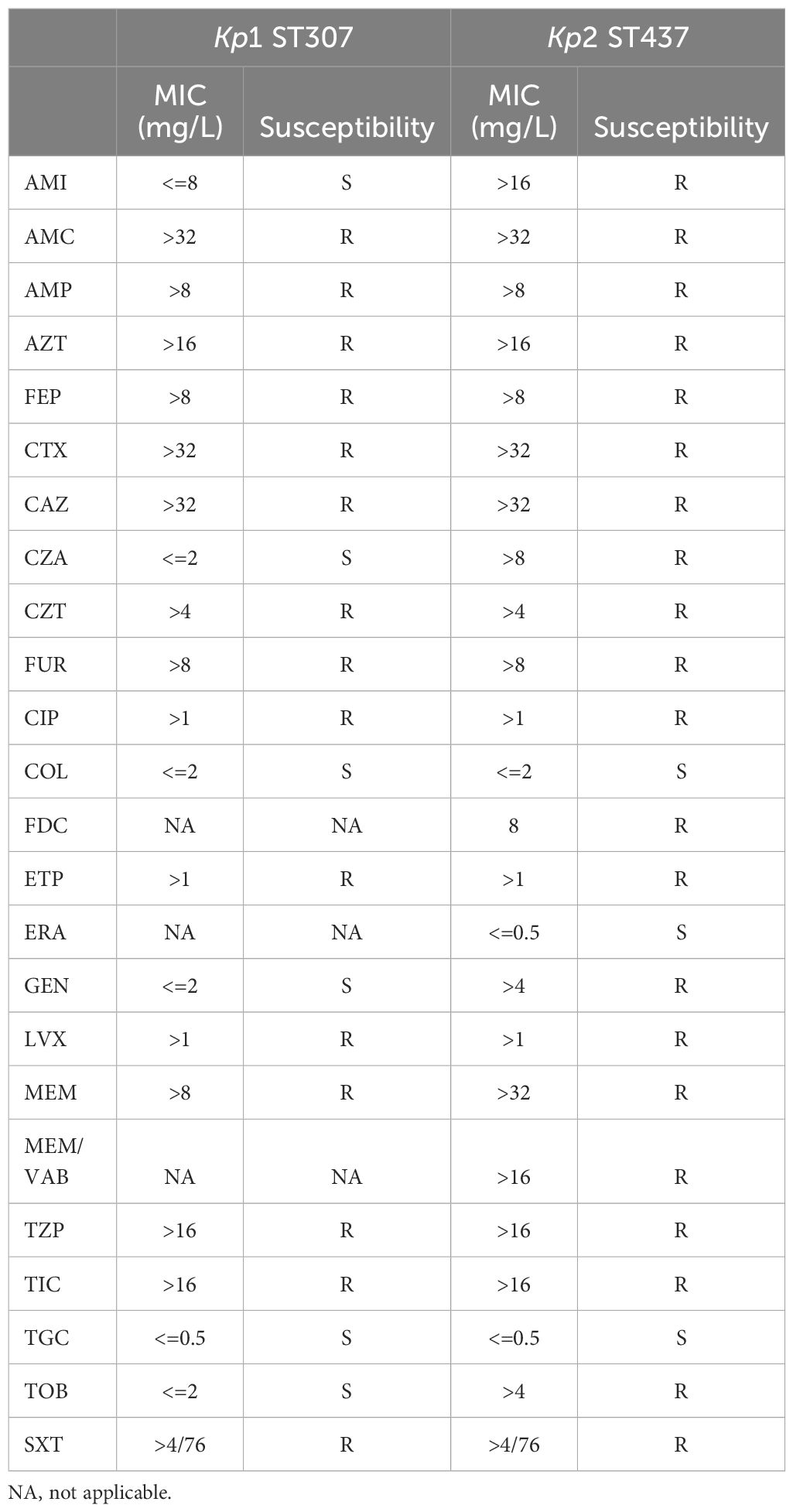
Table 1. Minimum inhibitory concentration (MIC) and susceptibility results of Kp1 and Kp2 strains.
On the 12th day of antibiotic therapy (2 days of meropenem and 10 days of CZA), the patient underwent surgical toileting due to clinical worsening of the sacral ulcer, and vacuum-assisted closure therapy was initiated with gradual improvement of the lesion. Tissue sampling for microbiological examination was performed, and a different Kp strain (Kp2) was isolated and identified from the culture (Table 1). Screening of carbapenemase genes in the Kp2 strain revealed the presence of blaNDM, blaOXA-181 and blaCTX-M1 genes. Considering the microbiological eradication of Kp1, CZA was interrupted and no indication for further antibiotic therapy was given, considering Kp2 to be a colonizing strain of the sacral ulcer. The medical histories of the patients and laboratory analyses of Kp strains are outlined in Figure 1.
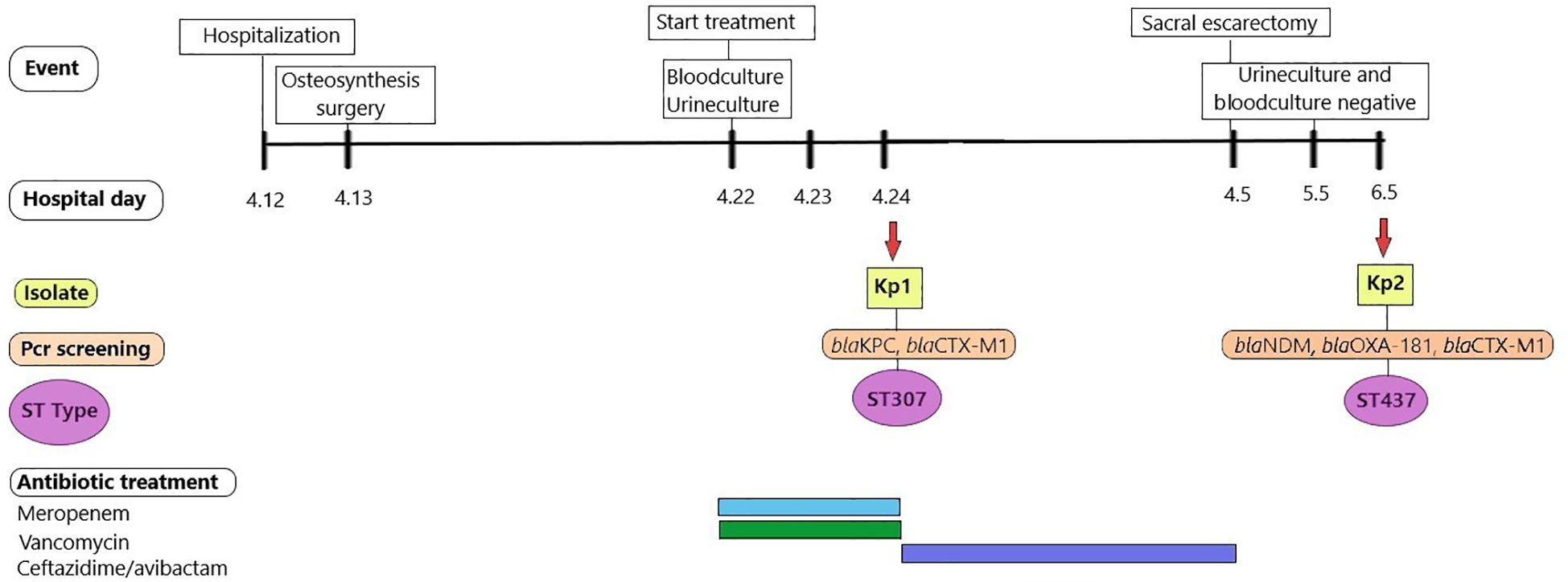
Figure 1. Medical history of the patient. Different colored bars in antibiotics treatment represent different antibiotics: light blue bar (Meropenem), green bar (Vancomycin), purple bar (Ceftazidime-avibactam).
Both Kp1 and Kp2 strains were subjected to whole-genome sequencing (WGS). DNA was extracted according to the protocol described by Cornacchia et al. (2022), and WGS was performed using the Illumina platform (Cornacchia et al., 2022). An in-house pipeline was used for the WGS data analysis. The genome assembly quality check was assessed according to Hennart et al. (2022) (n. contigs < 1,000, total length ranged from 4.5 to 6.5 Mbp, GC% < 59%). Species confirmation and K/O locus determination were performed in Kleborate (Lam et al., 2021) hosted on the PathogenWatch platform (Argimón et al., 2021); meanwhile, sequence type (ST) was calculated in silico according to the multilocus sequence typing (MLST) scheme hosted on the Pasteur sdb platform (Diancourt et al., 2005 and Brisse et al., 2009). Chromosomal and acquired resistance genes and outer membrane porin alterations were detected by querying the ResFinder 4.4.2 database (v. 12th December 2023) (Florensa et al., 2022).
3 ResultsWGS results confirmed that both strains belonged to species Klebsiella pneumoniae. MLST analysis revealed that Kp1 isolated from the blood and urine was a clone of ST307-CG307, and Kp2 from the sacral ulcer was a clone of ST437-CG10268. Capsular type (KL) and O locus (OL) analyses revealed that Kp1 belonged to KL102, OLO1/O2v2, and the capsular polysaccharide type was wzi173, while Kp2 belonged to KL52, OL101, and the capsular polysaccharide type was wzi50.
We focused on the Kp2 strain due to its phenotypic antimicrobial resistance and the presence of blaNDM gene, which had never been identified in the healthcare system of our province before. The AST (Table 1) showed that Kp2 was extensively resistant, in particular to the combinations of cephalosporins/β-lactamase inhibitors such as CZA or carbapenem/β-lactamase inhibitor meropenem/vaborbactam (MEM/VAB). Resistance was also observed for FDC. Kp2 was susceptible only to tetracyclines (eravacycline (MIC < 0.5 μg/ml) and tigecycline (MIC < 0.5 μg/ml)) and polymyxins (colistin (MIC <=2 μg/ml)). Based on the resistance phenotype, this strain is classified as extensively drug resistant (XDR) (Magiorakos et al., 2012).
Carbapenem resistance genes blaNDM-5 and blaOXA-232 and Extended Spectrum β-Lactamase (ESBL) blaCTX-M-15 genes were identified through querying the ResFinder 4.4.2 database. The other penicillin resistance genes identified were blaTEM-1D and blaSHV-11. Finally, trimethoprim (dfrA12), sulfonamide (sul1), and aminoglycoside (aac(6’)-Ib, aadA2, rmtB, rmtF) resistance genes were also identified. The GyrA-83I and ParC-80I mutations were also detected.
The presence of ompK36 with a glycine-aspartate (GD) L3 insertion was detected. The strain harbored several plasmid replicons (100% identity), including Inc-type (IncFII(K), IncFII, IncFIB(K), IncR) and Col-type (ColKP3, Col(BS512)) replicons. The ST437 strain was shown to have yersiniabactin ybt 14 located within the integrative conjugative element ICEKp5 to specifically overcome host-mediated iron limitation.
4 DiscussionTo the best of our knowledge, this is the first report of the identification of an ST437 blaNDM-5 producing Kp in the Abruzzo region of Italy. The ST437 Kp is a global epidemic clone, previously reported in North and South America (Wang et al., 2013; Tijet et al., 2014; Aires et al., 2020), Europe (Emeraud et al., 2022; Benulič et al., 2020; Palmieri et al., 2020; Fuster et al., 2020; Marti et al., 2017) and Asia (Zhu et al., 2018; Weng et al., 2020; Sahoo et al., 2023).
The ST437 clone is often associated with β-lactamase-producing genes, mainly blaKPC-2 and blaCTX-M-15, and more recently with blaOXA-like (blaOXA-48 and blaOXA-245) or blaNDM-like (specifically blaNDM-1, blaNDM-7 and blaNDM-23) genes. ST437 blaKPC-2 and blaCTX-M-15 expression was previously reported in isolates from Brazil (Andrade et al., 2011; Palmeiro et al., 2019) and blaKPC-2 and blaOXA-1 in Ontario, Canada (Tijet et al., 2014).
In Europe, several studies have reported the presence of ST437 clones as well. For instance, blaOXA-245 producing Kp (Oteo et al., 2013), blaNDM-7 producing Kp (Seara et al., 2015) and blaOXA-48 and blaNDM-1Kp were identified in Spain (Fuster et al., 2020).
Benulič et al. described the population of carbapenem-resistant Kp detected during an outbreak occurred in Slovenia between 2014–2017, including blaOXA-48 and/or blaNDM-1 ST437 strains. Palmieri et al. (2020) reported the presence of ST437, blaOXA-48 and blaNDM-1 in clinical Kp isolates from Serbia. In the same year, Weng et al. described for the first time a blaOXA-232 producing ST437 Kp strain in China. The blaOXA-232 producing strains are frequently associated with travel to India.
In 2023, blaNDM-5 ST437 Kp was isolated from a river in eastern India (Sahoo et al., 2023).
In Italy, the ST437 Kp clone is rarely detected, with previous reports in two hospitals in Padua between June 2009 and December 2011, which highlighted the presence of blaKPC-2 gene.
The ST437 Kp2 clone detected in our hospital was susceptible to colistin and tigecycline, and showed elevated MIC values of all carbapenems, cephalosporins and also novel β-lactamase inhibitor combinations (BLICs) tested. The blaNDM-5 carbapenemase identified in the ST437 Kp explains all β-lactam resistance observed, with the exception of that to aztreonam, which is not hydrolyzed by metallo-β-lactamases. However, this strain also carries blaCTX-M-15 as well as another class D carbapenemase, blaOXA-232, which may contribute to aztreonam resistance (de Man and Limbago, 2016). In this context, the use of avibactam protects aztreonam from hydrolysis, making it effective against NDM (Tamma et al., 2023).
High MICs for tobramycin, amikacin, and gentamicin were also observed, most likely due to the presence of rmtF. Fluoroquinolone resistance is also likely affected by the presence of GyrA-83I and ParC-80I mutations. The ST437 Kp isolate, in addition to blaNDM-5 and blaOXA-232, carried several mutated porin genes in ompK36 and ompK37 which are linked to resistance to cephalosporins and carbapenems. The presence of carbapenems and the co-occurrence of other resistance determinants (blaNDM-5, blaCTX-M, blaSHV, and blaTEM), virulence factors (ybt14), and the capsular serotype (KL52) further highlights its high pathogenic potential.
Among the blaNDM variants, blaNDM-5 was first reported in the UK in 2011 and has gained significant attention owing to its enhanced resistance to carbapenems and broad-spectrum cephalosporins (Li et al., 2018).
Infections caused by blaNDM-5-carrying CP-Kps are associated with high rates of morbidity, mortality, and transmission due to the dissemination ability of NDM-producing Kp strains (Paczosa and Mecsas, 2016; Jia et al., 2022).
In this study, the acquisition of blaNDM-5-producing Kp by the patient could not be explained by direct contact with a colonized patient. However, the potential involvement of undetected and asymptomatically-colonized patients in transmission routes cannot be excluded. The selective pressure of CZA treatment may have also favored the emergence of this NDM-producing Kp strain.
The case described here had no proven connection with India, Pakistan, the Middle East, the Balkans, Spain in Europe, Brazil, or North America. Therefore, the route through which NDM-producing Kp was introduced into the hospital is unknown. According to European Centre for Disease Prevention and Control (2011), patients with no direct link to countries where this clone is circulating are defined as autochthonous cases, indicating an unknown reservoir of NDM.
Two STs clones with similar virulence potentials and resistance profiles were also identified. Hence, a single dominant clone is not the only one responsible for severe infections, causing repercussions on prognosis and therapeutic treatment (Venturini et al., 2022). Although the number of bacterial isolates belonging to the same species analyzed per sample is determined by response times, increases in testing capacity and improved diagnostic protocols are needed to improve preciseness in the identification procedure. The ST437 Kp2 clone was considered by the infectious disease clinician to be a colonizing strain, in fact after surgical toilet and vacuum-assisted suture therapy the lesion gradually improved and no local or systemic signs of active infection occurred. For these reasons the patient did not receive further antibiotic treatment. Nevertheless, antibiotic pressure plays a decisive role in modifying the susceptibility of microorganisms to various antibiotics (Shields et al., 2017).
Approximately one-third of deaths caused by AMR in Europe occur in Italy (https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistance-surveillance-europe-2022-2020-data). Italy is one of the countries with a high rate of antibiotic resistance, and where antibiotics are used excessively and often inappropriately, although there are signs of improvement, as reported in the last Ears-NET report (carbapenem-resistant isolates percentage from 26.7% to 24.9%).
Southern regions of Italy have critically higher levels of carbapenem-resistant Kp strains than the northern parts. In Southern Italy, Abruzzo, Apulia and Campania are the regions with the highest levels of prevalence of antimicrobial use (around 45%) (Medicines use in Italy National Report Year 2022 Published on: 01 December 2023).
Pérez-Galera et al. (2023) described several risk factors, which may contribute favoring Carbapenem-resistant Enterobacteriaceae (CRE) infections. These factors include hospitalization in the last three months, previous colonization/infection by CRE, chronic heart failure, dementia, chronic renal failure, central venous and urinary catheters, dialysis, and previous use of antibiotics. Moreover, significant comorbidities and invasive surgeries play a key role in the deterioration of the immune status conditions of hospitalized patients (European Centre for Disease Prevention and Control, 2011; Zuo et al., 2021). Most of the previously described risk factors were identified in the present case.
After the first case of NDM-producing ST437 Kp, several infection control measures were implemented in our healthcare setting, including contact precautions in individual rooms, reinforcement of standard cross-transmission control measures, cleaning procedures, and active surveillance cultures, together with retraining courses for operators. All these measures were adopted to raise awareness of this issue and avoid the spread of this strain associated with high mobility and mortality in our patients (World Health Organization, 2016 and 2017). All control measures activated and surveillance activities (culture swabs combined with molecular methods) were successful, indeed only one positive patient was identified. The patient positive for the presence of the ST437 Kp strain was a 92 years old woman, bedridden, with a long hospital stay and a bladder catheter, therefore with many risk factors for colonization. After the first detection of this strain in the hospital, other rare and sporadic findings of ST437 Kp strain were recorded (6 cases of urinary infections) in the following 7 months. In all cases, infection control measures effectively prevented the spread of the strain among patients. Heterogeneity in coverage across the wards in the hospital and the use of culture and not molecular methods for the identification of carbapenem resistant strains in screening practice, limits the knowledge of the real spread of the ST437 Kp strain in our healthcare setting.
The effectiveness of infection control interventions for the early detection and/or control of the transmission of NDM-producing Enterobacteriaceae has not been proven yet. However, an ECDC risk assessment report demonstrated the effectiveness of active surveillance and control measures, including a dedicated team for all suspected and CPE-positive patients (European Centre for Disease Prevention and Control, 2011). The emergence of clones carrying new genetic determinants, especially in local areas and small regions such as the Abruzzo region, requires prompt diagnosis and therapeutic protocols, as well as further investigations to better understand the potential transmission routes and evolution of these clones. This case report is the snapshot of a restricted geographic area in a limited period of time and its origin is still unknown. For this reason, a more active AMR surveillance involving other hospitals in Abruzzo and the other Italian regions combined with next generation methods could potentially improve Kp infection treatment and patient outcomes. It is time for a more effective and widespread antimicrobial stewardship with a multidisciplinary approach to be implemented in hospitals and outpatients. These strategies should involve local, regional, and central government monitoring, auditing, and feedback.
Data availability statementThe datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://www.ncbi.nlm.nih.gov/genbank/, SAMN40624209 https://www.ncbi.nlm.nih.gov/genbank/, SAMN40624210.
Ethics statementEthical approval was not required for the studies involving humans because The retrospective analysis of the clinical data did not involve procedures that normally require written consent outside of the research context. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements because The retrospective analysis of the clinical data did not involve procedures that normally require written consent outside of the research context. Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article because The retrospective analysis of the clinical data did not involve procedures that normally require written consent outside of the research context.
Author contributionsSR: Conceptualization, Formal Analysis, Methodology, Writing – original draft, Writing – review & editing. VF: Methodology, Writing – review & editing. AD’: Methodology, Writing – review & editing. MF: Methodology, Writing – review & editing. VD: Investigation, Methodology, Writing – review & editing. CD: Investigation, Methodology, Writing – review & editing. SD: Methodology, Writing – review & editing. LD: Methodology, Writing – review & editing. MD: Investigation, Methodology, Writing – review & editing. MP: Methodology, Writing – review & editing. ACH: Formal Analysis, Methodology, Writing – original draft, Writing – review & editing. GC: Methodology, Writing – review & editing. CC: Methodology, Writing – review & editing. FP: Funding acquisition, Writing – review & editing. ACO: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing.
FundingThe author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by EU funding within the NextGenerationEU-MUR PNRR Extended Partnership initiative on Emerging Infectious Diseases (Project no. PE00000007, INF-ACT).
Conflict of interestThe authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ReferencesAires, C. A. M., Pereira, P. S., Rocha-de-Souza, C. M., Silveira, M. C., Carvalho-Assef, A. P. D., Asensi, M. D. (2020). Population structure of KPC-2-producing klebsiella pneumoniae isolated from surveillance rectal swabs in Brazil. Microb. Drug Resist. 26, 652–660. doi: 10.1089/mdr.2019.0166
PubMed Abstract | Crossref Full Text | Google Scholar
Andrade, L. N., Curiao, T., Ferreira, J. C., Longo, J. M., Clímaco, E. C., Martinez, R., et al. (2011). Dissemination of blaKPC-2 by the spread of Klebsiella pneumoniae clonal complex 258 clones (ST258, ST11, ST437) and plasmids (IncFII, IncN, IncL/M) among Enterobacteriaceae species in Brazil. Antimicrob. Agents Chemother. 55, 3579–3583. doi: 10.1128/AAC.01783-10
PubMed Abstract | Crossref Full Text | Google Scholar
Argimón, S., David, S., Underwood, A., Abrudan, M., Wheeler, N. E., Kekre, M., et al. (2021). NIHR global health research unit on genomic surveillance of antimicrobial resistance. Rapid genomic characterization and global surveillance of klebsiella using pathogenwatch. Clin. Infect. Dis. 73, S325–S335. doi: 10.1093/cid/ciab784
PubMed Abstract | Crossref Full Text | Google Scholar
Benulič, K., Pirš, M., Couto, N., Chlebowicz, M., Rossen, J. W. A., Zorec, T. M., et al. (2020). Whole genome sequencing characterization of Slovenian carbapenem-resistant Klebsiella pneumoniae, including OXA-48 and NDM-1 producing outbreak isolates. PloS One 15, e0231503. doi: 10.1371/journal.pone.0231503
PubMed Abstract | Crossref Full Text | Google Scholar
Brisse, S., Fevre, C., Passet, V., Issenhuth-Jeanjean, S., Tournebize, R., Diancourt, L., et al. (2009). Virulent clones of Klebsiella pneumoniae: identification and evolutionary scenario based on genomic and phenotypic characterization. PloS One 4, e4982. doi: 10.1371/journal.pone.0004982
PubMed Abstract | Crossref Full Text | Google Scholar
Cornacchia, A., Chiaverini, A., Centorotola, G., Di Domenico, M., Cocco, A., Ancora, M., et al. (2022). Whole-genome sequences of two klebsiella pneumoniae strains (Sequence types 23 and 35) from wildlife. Microbiol. Resour Announc. 11, e0014022. doi: 10.1128/mra.00140-22
PubMed Abstract | Crossref Full Text | Google Scholar
Diancourt, L., Passet, V., Verhoef, J., Grimont, P. A., Brisse, S. (2005). Multilocus Sequence Typing of Klebsiella pneumoniae nosocomial isolates. J. Clin. Microbiol. 43, 4178–4182. doi: 10.1128/JCM.43.8.4178-4182.2005
PubMed Abstract | Crossref Full Text | Google Scholar
Di Pilato, V., Henrici De Angelis, L., Aiezza, N., Baccani, I., Niccolai, C., Parisio, E. M., et al. (2022). Resistome and virulome accretion in an NDM-1-producing ST147 sublineage of Klebsiella pneumoniae associated with an outbreak in Tuscany, Italy: a genotypic and phenotypic characterisation. Lancet Microbe 3, e224–e234. doi: 10.1016/S2666-5247(21)00268-8
PubMed Abstract | Crossref Full Text | Google Scholar
Emeraud, C., Birer, A., Girlich, D., Jousset, A. B., Creton, E., Naas, T., et al. (2022). Polyclonal dissemination of OXA-232 carbapenemase-producing klebsiella pneumoniae, France 2013-2021. Emerg. Infect. Dis. 28, 2304–2307. doi: 10.3201/eid2811.221040
PubMed Abstract | Crossref Full Text | Google Scholar
European Centre for Disease Prevention and Control (2011). Updated risk assessment on the spread of NDM and its variants within Europe (Stockholm: ECDC).
European Centre for Disease Prevention and Control (2023). Antimicrobial resistance in the EU/EEA (EARS-Net) - Annual Epidemiological Report 2022 (Stockholm: ECDC).
Florensa, A. F., Kaas, R. S., Clausen, P. T. L. C., Aytan-Aktug, D., Aarestrup, F. M. (2022). ResFinder - an open online resource for identification of antimicrobial resistance genes in next-generation sequencing data and prediction of phenotypes from genotypes. Microb. Genom. 8, 748. doi: 10.1099/mgen.0.000748
Crossref Full Text | Google Scholar
Fuster, B., Salvador, C., Tormo, N., García-González, N., Gimeno, C., González-Candelas, F. (2020). Molecular epidemiology and drug-resistance mechanisms in carbapenem-resistant Klebsiella pneumoniae isolated in patients from a tertiary hospital in Valencia, Spain. J. Glob Antimicrob. Resist. 22, 718–725. doi: 10.1016/j.jgar.2020.05.002
PubMed Abstract | Crossref Full Text | Google Scholar
Guo, H., Wu, Y., Li, L., Wang, J., Xu, J., He, F. (2023). Global emergence of carbapenem-resistant Klebsiella pneumonia co-carrying multiple carbapenemases. Comput. Struct. Biotechnol. J. 21, 3557–3563. doi: 10.1016/j.csbj.2023.07.013
PubMed Abstract | Crossref Full Text | Google Scholar
Hennart, M., Guglielmini, J., Bridel, S., Maiden, M. C. J., Jolley, K. A., Criscuolo, A., et al. (2022). A dual barcoding approach to bacterial strain nomenclature: genomic taxonomy of klebsiella pneumoniae strains. Mol. Biol. Evol. 39, msac135. doi: 10.1093/molbev/msac135
PubMed Abstract | Crossref Full Text | Google Scholar
Jia, P., Jia, X., Zhu, Y., Liu, X., Yu, W., Li, R., et al. (2022). Emergence of a novel NDM-5-producing sequence type 4523 klebsiella pneumoniae strain causing bloodstream infection in China. Microbiol. Spectr. 10, e0084222. doi: 10.1128/spectrum.00842-22
PubMed Abstract | Crossref Full Text | Google Scholar
Lam, M. M. C., Wick, R. R., Watts, S. C., Cerdeira, L. T., Wyres, K. L., Holt, K. E. (2021). A genomic surveillance framework and genotyping tool for Klebsiella pneumoniae and its related species complex. Nat. Commun. 12, 4188. doi: 10.1038/s41467-021-24448-3
PubMed Abstract | Crossref Full Text | Google Scholar
Li, X., Fu, Y., Shen, M., Huang, D., Du, X., Hu, Q., et al. (2018). Dissemination of blaNDM-5 gene via an IncX3-type plasmid among non-clonal Escherichia coli in China. Antimicrob. Resist. Infect. Control 7, 59. doi: 10.1186/s13756-018-0349-6
PubMed Abstract | Crossref Full Text | Google Scholar
Magiorakos, A. P., Srinivasan, A., Carey, R. B., Carmeli, Y., Falagas, M. E., Giske, C. G., et al. (2012). Multidrugresistant, extensively drug-resistant and pan drug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 18 (3), 268–281. doi: 10.1111/j.1469-0691.2011.03570.x
PubMed Abstract | Crossref Full Text | Google Scholar
Marti, R., Stephan, R., Klumpp, J., Nüesch-Inderbinen, M., Hummerjohann, J., Bagutti, C., et al. (2017). Draft genome sequence of klebsiella pneumoniae 704SK6, an OXA-48- and CTX-M-15-encoding wastewater isolate. Genome Announc 5 (33), e00831–17. doi: 10.1128/genomea.00831-17
PubMed Abstract | Crossref Full Text | Google Scholar
Oteo, J., Hernández, J. M., Espasa, M., Fleites, A., Sáez, D., Bautista, V., et al. (2013). Emergence of OXA-48-producing Klebsiella pneumoniae and the novel carbapenemases OXA-244 and OXA-245 in Spain. J. Antimicrob. Chemother. 68, 317–321. doi: 10.1093/jac/dks383
PubMed Abstract | Crossref Full Text | Google Scholar
Paczosa, M. K., Mecsas, J. (2016). Klebsiella pneumoniae: going on the offense with a strong defense. Microbiol. Mol. Biol. Rev. 80, 629661. doi: 10.1128/mmbr.00078-15
Crossref Full Text | Google Scholar
Palmeiro, J. K., de Souza, R. F., Schörner, M. A., Passarelli-Araujo, H., Grazziotin, A. L., Vidal, N. M., et al. (2019). Molecular epidemiology of multidrug-resistant klebsiella pneumoniae isolates in a Brazilian tertiary hospital. Front. Microbiol. 10. doi: 10.3389/fmicb.2019.01669
Crossref Full Text | Google Scholar
Palmieri, M., D’Andrea, M. M., Pelegrin, A. C., Mirande, C., Brkic, S., Cirkovic, I., et al. (2020). Genomic epidemiology of carbapenem- and colistin-resistant klebsiella pneumonia isolates from Serbia: predominance of ST101 strains carrying a novel OXA-48 plasmid. Front. Microbiol. 11. doi: 10.3389/fmicb.2020.00294
Crossref Full Text | Google Scholar
Pérez-Galera, S., Bravo-Ferrer, J. M., Paniagua, M., Kostyanev, T., de Kraker, M. E. A., Feifel, J., et al. (2023). Risk factors for infections caused by carbapenem-resistant Enterobacterales: an international matched case-control-control study (EURECA). EClinicalMedicine 57, 101871. doi: 10.1016/j.eclinm.2023.101871
PubMed Abstract | Crossref Full Text | Google Scholar
Sahoo, S., Sahoo, R. K., Dixit, S., Behera, D. U., Subudhi, E. (2023). NDM-5-carrying Klebsiella pneumoniae ST437 belonging to high-risk clonal complex (CC11) from an urban river in eastern India. 3 Biotech. 13, 139. doi: 10.1007/s13205-023-03556-5
PubMed Abstract | Crossref Full Text | Google Scholar
Seara, N., Oteo, J., Carrillo, R., Pérez-Blanco, V., Mingorance, J., Gómez-Gil, R., et al. (2015). Interhospital spread of NDM-7-producing Klebsiella pneumoniae belonging to ST437 in Spain. Int. J. Antimicrob. Agents 46, 169–173. doi: 10.1016/j.ijantimicag.2015.04.001
PubMed Abstract | Crossref Full Text | Google Scholar
Shields, R. K., Chen, L., Cheng, S., Chavda, K. D., Press, E. G., Snyder, A., et al. (2017). Emergence of Ceftazidime-Avibactam Resistance Due to Plasmid-Borne blaKPC-3 Mutations during Treatment of Carbapenem-Resistant Klebsiella pneumoniae Infections. Antimicrob. Agents Chemother. 61 (3), e02097–16. doi: 10.1128/aac.02097-16
PubMed Abstract | Crossref Full Text | Google Scholar
Tamma, P. D., Aitken, S. L., Bonomo, R. A., Mathers, A. J., Duin, D. v., Clancy, C. J. (2023). Infectious diseases society of America 2023 guidance on the treatment of antimicrobial resistant gram-negative infections. Clin. Infect. Dis., ciad428. doi: 10.1093/cid/ciad428
PubMed Abstract | Crossref Full Text | Google Scholar
Tijet, N., Sheth, P. M., Lastovetska, O., Chung, C., Patel, S. N., Melano, R. G. (2014). Molecular characterization of klebsiella pneumoniae carbapenemase (KPC)-producing enterobacteriaceae in ontario, Canada 2008-2011. PloS One 9, e116421. doi: 10.1371/journal.pone.0116421
PubMed Abstract | Crossref Full Text | Google Scholar
Tumbarello, M., Trecarichi, E. M., Corona, A., De Rosa, F. G., Bassetti, M., Mussini, C., et al. (2019). Efficacy of ceftazidime-avibactam salvage therapy in patients with infections caused by klebsiella pneumoniae carbapenemase-producing K. Pneumoniae. Clin. Infect. Dis. 68, 355–364. doi: 10.1093/cid/ciy492
PubMed Abstract | Crossref Full Text | Google Scholar
Venturini, C., Bowring, B., Partridge, S. R., Ben Zakour, N. L., Fajardo-Lubian, A., Lopez Ayala, A., et al. (2022). Co-occurrence of multidrug resistant klebsiella pneumoniae pathogenic clones of human relevance in an equine pneumonia case. Microbiol. Spectr. 10, e0215821. doi: 10.1128/spectrum.02158-21
PubMed Abstract | Crossref Full Text | Google Scholar
Wang, G., Huang, T., Surendraiah, P., Wang, K., Komal, R., Zhuge, J., et al. (2013). CTX-M β-lactamase–producing klebsiella pneumoniae in Suburban New York City, New York, USA. Emerg. Infect. Dis. 19, 1803–1810. doi: 10.3201/eid1911.121470
PubMed Abstract | Crossref Full Text | Google Scholar
Weng, X., Shi, Q., Wang, S., Shi, Y., Sun, D., Yu, Y. (2020). The characterization of OXA-232 carbapenemase-producing ST437 klebsiella pneumoniae in China. Can. J. Infect. Dis. Med. Microbiol. 2020, 5626503. doi: 10.1155/2020/5626503
PubMed Abstract | Crossref Full Text | Google Scholar
World Health Organization (2016). Guidelines on core components of infection prevention and control programmes at the national and acute health care facility level (Geneva: IGO). Licence: CC BY-NC-SA 3.0.
World Health Organization (2017). Guidelines for the prevention and control of carbapenem-resistant Enterobacteriaceae, Acinetobacter baumannii and Pseudomonas aeruginosa in health care facilities (Geneva: IGO). Licence: CC BY-NC-SA 3.0.
留言 (0)