Overcoming diagnostic challenges in constrictive pericarditis: why volume is important?
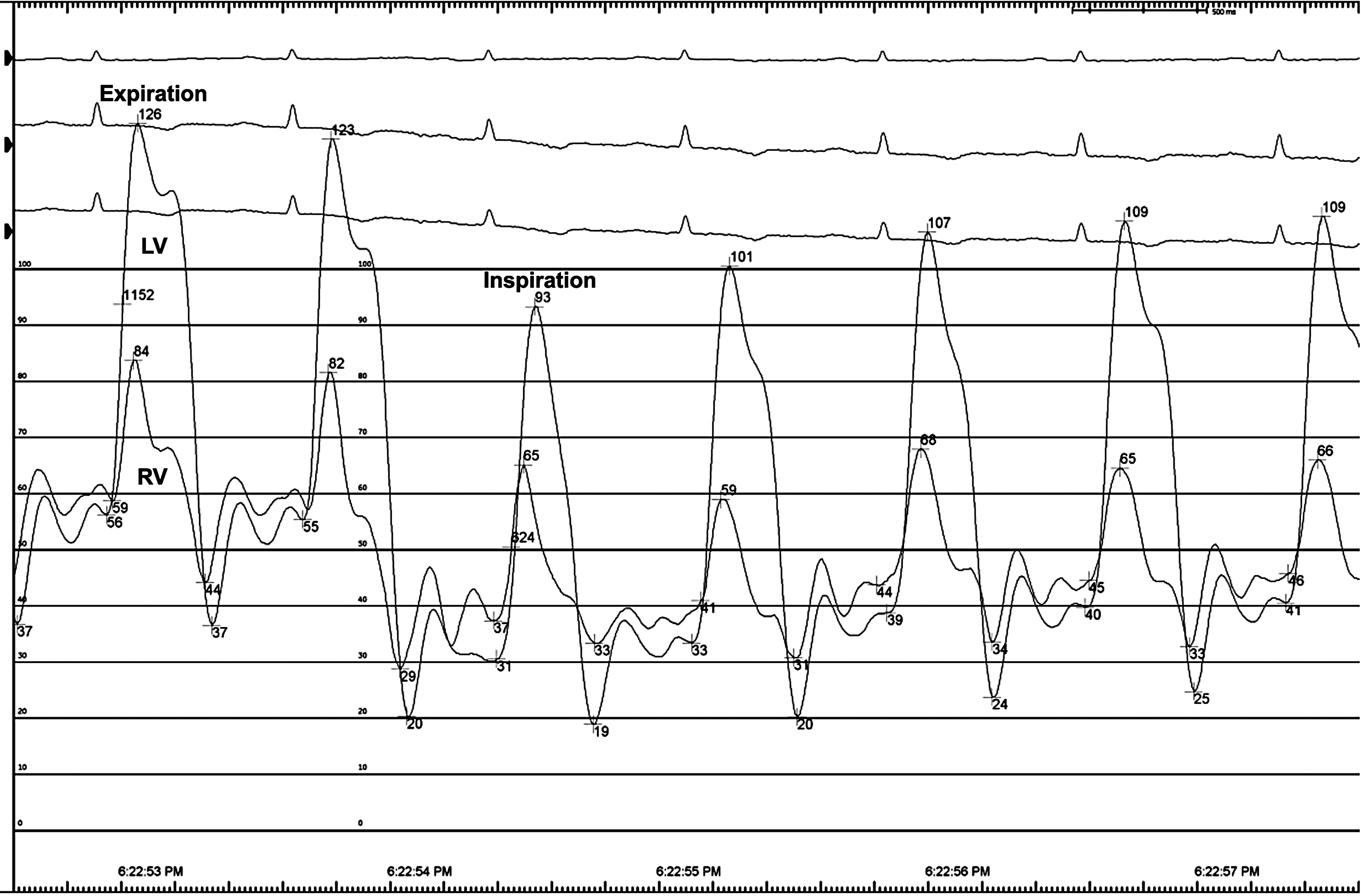
A 65-year-old male with chronic liver disease and cirrhosis under evaluation for liver transplant, with a presumptive diagnosis of cirrhosis secondary to nonalcoholic steatohepatitis, had ascites refractory to increasing doses of diuretics. Liver biopsy, liver Doppler ultrasound and magnetic resonance imaging were not consistent with etiology. Transthoracic echocardiogram showed annulus reversus and marked respiratory variation of the pulsed wave Doppler of mitral and tricuspid inflow velocities suggesting constrictive pericarditis (CP), and the patient was referred to our cardiology outpatient clinic. Further work-up with right heart catheterization (RHC) showed very elevated right atrium pressure (35 mmHg), near equalisation of right and left ventricles end-diastolic pressures (36 and 41 mmHg, respectively), with square-root sign. However, it wasn’t able to show dissociation between pulmonary capillary wedge pressure and left ventricle end-diastolic pressure with respiration nor exaggerated ventricular interdependence (Fig. 1), which couldn’t confirm the diagnosis of CP. An initial cardiac magnetic resonance (CMR) demonstrated thickened pericardium, without pericardial effusion, but was also inconclusive for exaggerated ventricular interdependence. Although the RHC and CMR were carried out after fluid challenge, the patient was taking high doses of diuretics and our cardiology team believed the overdiuresis masked the constrictive physiology. Due to the rapid deterioration of liver function tests and the urgent need to decide on the patient’s eligibility for a liver transplant, it was decided to discontinue diuretics and repeat CMR. After one week of interruption of diuretics, a second CMR demonstrating pericardial thickening, exaggerated ventricular interdependence with ventricular septal shift and diastolic interventricular septal bounce (Fig. 2), gave the answers to our dilemma. The patient underwent pericardiectomy, which resolved his symptoms of fluid overload, and the liver function tests slowly returned to normal. Two years later, the patient remains asymptomatic and off the liver transplant list.







留言 (0)