
記住我

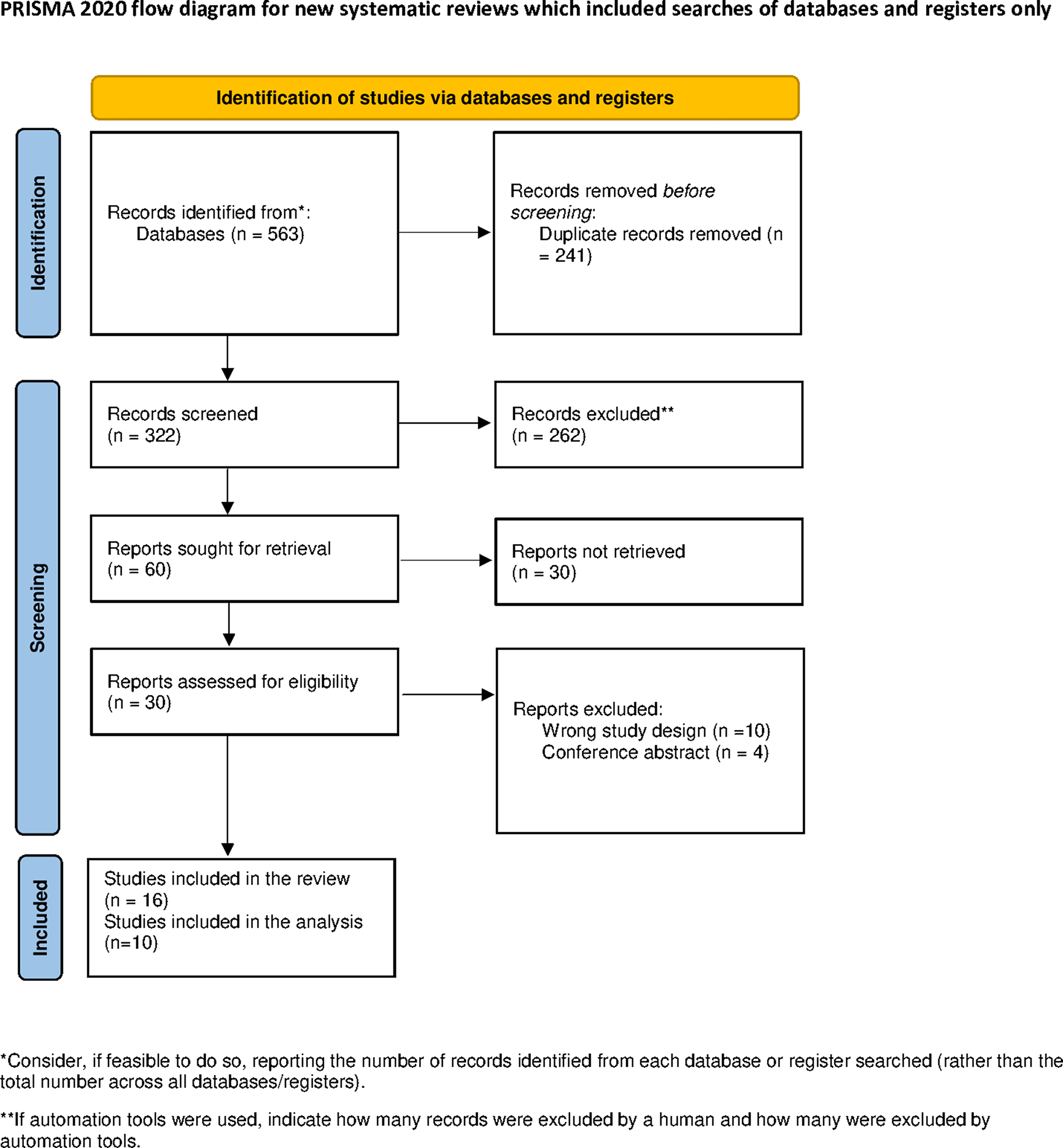



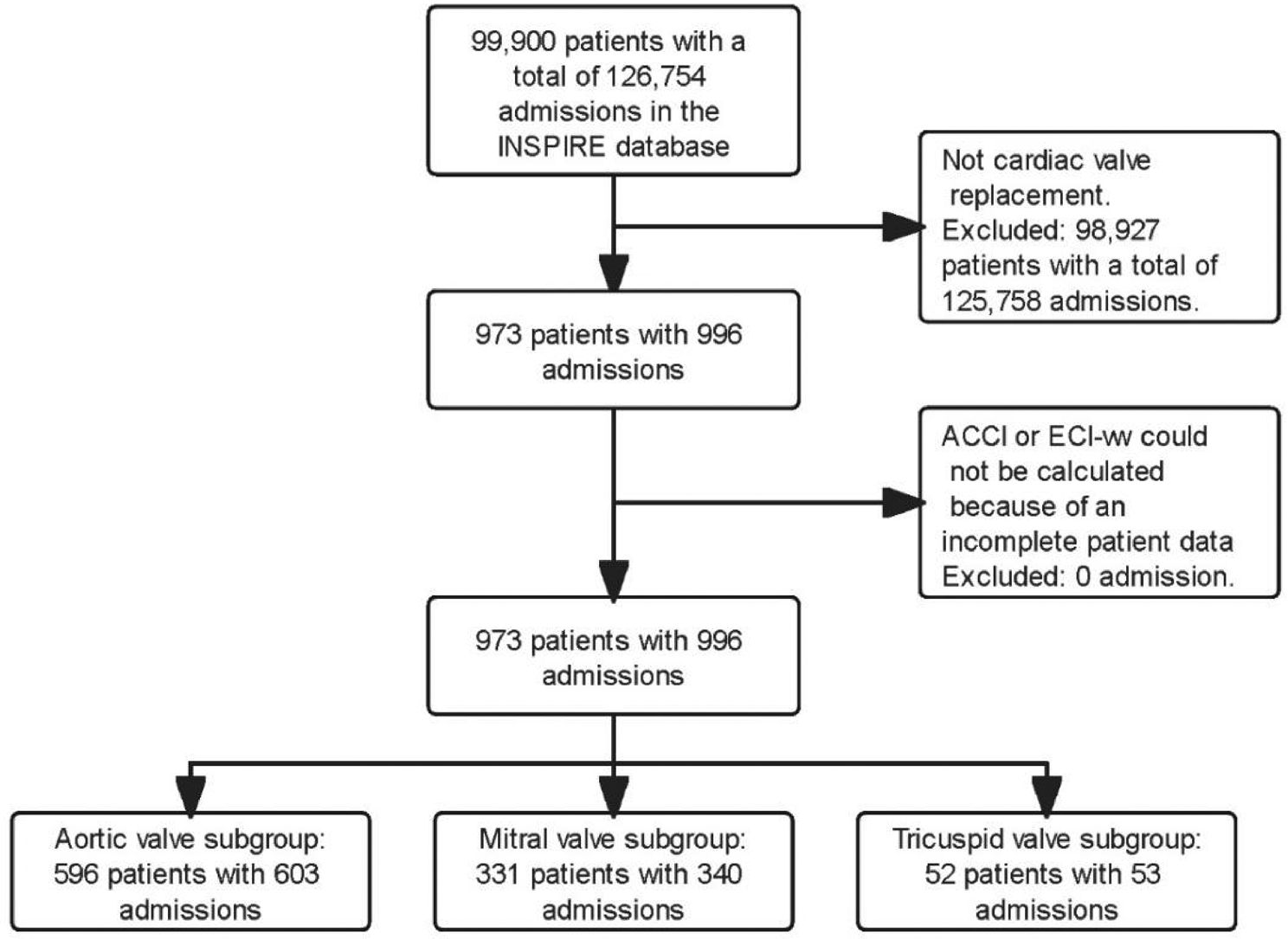
Data were retrospectively harvested from the Shandong Cancer Hospital and Institute’s database for the period 2021 to 2023, focusing on non-small cell lung cancer patients who underwent induction therapy, encompassing both immunochemotherapy and chemotherapy. A total of 135 patients achieved complete (R0) resection post-induction therapy. This cohort included 20 (14.8%) sleeve lobectomy cases, 70 (51.9%) instances of isolated lobectomy, 18 (13.3%) patients receiving combined lobectomy (excluding pneumonectomy), and 27 (20.0%) undergoing pneumonectomy. Subsequent categorization based on induction therapy divided these patients into two groups: 15 patients in the ICI with chemo group, and 12 patients in the chemotherapy-only (Chemo) group, as illustrated in Fig. 1. The Institutional Review Board /Ethics Committee granted approval for this study. Due to the retrospective nature of the research and pre-existing consent for data usage at the time of surgery, the requirement for individual data consent was exempted.
Fig. 1
Patient selection flowchart. chemo chemotherapy; ICI immune checkpoint inhibitor
Treatment and follow-upAll patient treatment plans are discussed through multidisciplinary consultations.Between two to four cycles of induction therapy were administered to patients, which included the use of programmed cell death protein 1 (PD-1) inhibitors alongside a dual chemotherapy regimen incorporating platinum in ICI group, while only a dual chemotherapy regimen incorporating platinum in chemo group as per established guidelines, with treatments occurring tri-weekly. Patients with squamous cell carcinoma received albumin paclitaxel combined with carboplatin regimen, while patients with adenocarcinoma received pemetrexed combined with carboplatin regimen. In the ICI group, 13 patients received 3 cycles of treatment, 1 patient received surgical treatment in advance due to unclear remission of the lesions in 2 cycles, and 1 patient did not undergo the third cycle of treatment due to severe bone marrow suppression.
In the chemotherapy group, 11 patient received 3 cycles of treatment, and 1 patient received one more cycle treatment due to the large lesion.Subsequent to the completion of the induction phase, surgical interventions were scheduled to occur between three to six weeks later. Across the treatment continuum, patients were subjected to a total of four chemotherapy cycles, both preceding and following surgery, with an additional recommendation for the continued application of the same PD-1 inhibitor over a span of one year as part of adjuvant therapy. Diagnostic and preparatory evaluations prior to surgery encompassed comprehensive computed tomography (CT) scans of the chest, abdomen, and brain, supplemented by bone scans for all patients. In instances of ambiguous brain CT outcomes, magnetic resonance imaging (MRI) was employed to ascertain clarity. Bronchoscopies were systematically conducted to facilitate tissue diagnosis and to aid in the meticulous planning of surgical procedures. In scenarios where CT scans proved insufficient for the definitive determination of lymph node metastasis, positron emission tomography (PET) scans, along with endobronchial ultrasound, were predominantly utilized. A complete removal of the mediastinal lymph nodes was carried out in a methodical manner. The histological grading of tumors was done according to the latest criteria given by the WHO and staging of the tumors was decided carefully as per the eighth edition of TNM classification system by International Association for the Study of Lung Cancer. Postoperative follow-up was strictly organized, with regular scheduled outpatient consultations at 1, 3, 6, and 12 months after the surgery, and biannual thereafter during three or five years in case of stage III patients, and then annual afterwards. Chest-CT scan was ordered for each visit to track progress of the patient. The follow-up of patients who were not able to come for these consultations was also done through telephone in which comprehensive data on the patients’ current status, the recurrence patterns and mortality was closely extracted from these telephone calls as well as the records of the clinic.
Outcome measuresSurgical complications were meticulously classified according to the Clavien-Dindo system, identifying those of grade III or above as significant [1]. Documented pulmonary issues encompassed a range of conditions from pneumonia and empyema to acute respiratory distress syndrome, necessitating reintubation for respiratory failure, as well as pleural effusion and pulmonary embolism. Cardiac-related complications included arrhythmias, demand ischemia, and heart attacks. Challenges related to anastomosis featured leaks, separation, and the formation of fistulas. Other notable complications covered chyle leaks, deep vein thrombosis, infections at the surgical site, and injuries to the recurrent laryngeal nerve. The period from the completion of neoadjuvant therapy to the surgical procedure was precisely measured, as was the duration of the surgery itself, from the initial cut to the final suture. The main focus was on identifying major complications occurring within 30 days following the operation. Secondary outcomes concentrated on the pathological responses, including complete pathologic response (PCR) and major pathologic response (MPR), using the TNM staging from the eighth edition of the American Joint Committee on Cancer’s staging manual for cancer, and the mediastinal lymph node mapping adhered to the 2009 guidelines set by the International Association for the Study of Lung Cancer. The effectiveness of the therapeutic interventions was evaluated based on the percentage of tumor cells that remained viable, utilizing routine hematoxylin and eosin staining techniques, in accordance with the methodology proposed by Hellmann et al. [11].
Statistical analysisFor the analysis of discrete data, the utilization of percentage metrics was standard, while the assessment of continuous data relied on the calculation of mean values and their standard deviations, employing one-way analysis of variance with the application of Scheffe’s method for post-hoc adjustment when required. The evaluation of binary outcomes such as OS, DFS, post-surgical mortality, and incidences of complications was conducted through the computation of hazard ratios (HRs). To chart the progression of OS and DFS, the Kaplan–Meier method was employed, facilitating the generation and comparison of survival curves via the log-rank test. Estimations of HRs were refined using Cox proportional hazards models. The comprehensive statistical analysis was carried out using the SPSS software, version 24.0, developed by IBM-SPSS Inc., Armonk, NY, and the GraphPad Prism software, version 7.0d, from GraphPad Software, San Diego, California. The approach to hypothesis testing was bidirectional, ensuring a comprehensive assessment of the data.
留言 (0)