
記住我
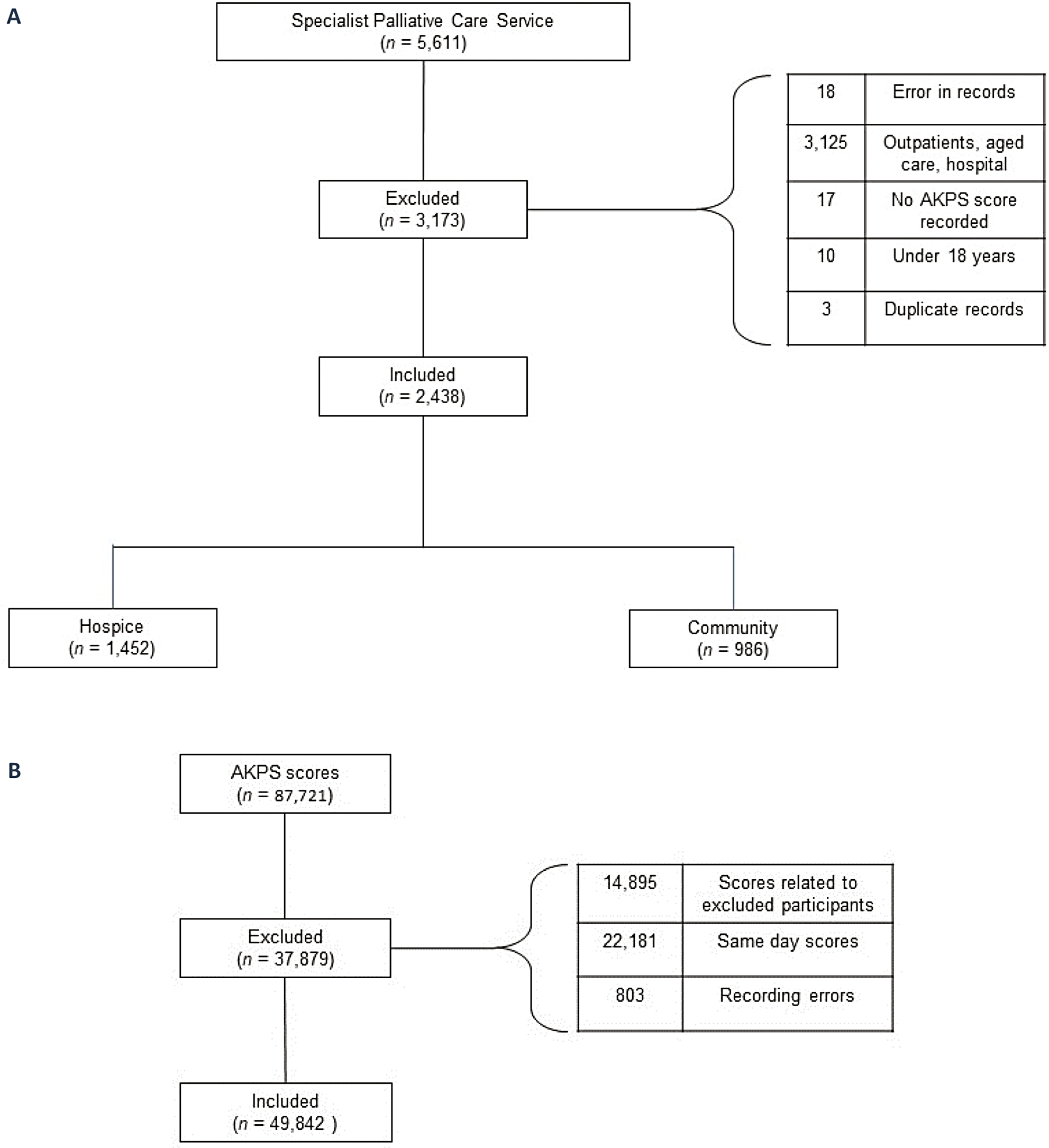




The literature search produced 5,572 records from electronic database searches including an additional 9 documents from grey literature sources (Fig. 1 PRISMA-ScR flowchart). Following the removal of duplicates (n = 1,994), 3,578 titles and abstracts were reviewed and 3,402 were deemed to be irrelevant. 176 full-text studies were assessed for eligibility. Overall, 51 met the inclusion criteria for this scoping review. Reasons for exclusion included studies that were not directly addressing the review objectives (n = 87), insufficient detail on key concepts (n = 11), wrong context (n = 8), unable to source at this time (n = 7), adult population only (n = 3), unable to disaggregate data for children (n = 3), and study more recently described (n = 6).
Fig. 1 Study characteristics
Study characteristicsTable 3 presents descriptive information on the study characteristics. Of the 51 included papers, the majority (n = 47, 92%) were published between 2013 and 2023. Thirteen studies adopted a multi-country, European or global perspective [1,2,3,4, 6, 14, 25,26,27,28,29,30,31], 10 studies were conducted in either Canada, the USA, or South America [32,33,34,35,36,37,38,39,40,41], 22 studies were undertaken in Europe, of which 14 were UK-based [7, 8, 11, 12, 42,43,44,45,46,47,48,49,50,51], and other European countries included Belgium, France, Germany, Ireland, and Italy [9, 52,53,54,55,56,57,58]. Six papers focused on population cohorts in Asia (China, Malaysia, South Korea), Australia, and Africa (Uganda, South Africa) [10, 21, 59,60,61,62].
Table 3 Study characteristics (n = 51)Of the 51 included papers, 13 articles defined or discussed population-level need for CPC from an international policy, planning, or conceptual discussion perspective (category 1). Thirty-eight articles were applied studies, defining CPC need as well as describing the data and methods used to quantify population-level need for CPC (category 2).
The majority of articles focused on children and young people (n = 37). A small number of articles focused on the perinatal/neonatal population (n = 5). In this paper, the term ‘child’ refers to infants, children and young people unless otherwise specified.
The extracted material from each article (i.e., study descriptives, study focus, applied methodological characteristics, etc.) is presented in Table 4.
Table 4 Summary of extract data from included papers (n = 51)Category (1) defining CPC need - policy/conceptsThe review included 13 international policy statements/standards and general conceptual discussions on CPC need, of which two referred to both adults and children [6, 26], 11 focused specifically on children [1,2,3,4, 9, 14, 27, 29, 35, 36, 39].
Policy statements/standardsThe ‘Global Atlas of Palliative Care’ defined need for palliative care for adults and children in terms of the concept of ‘serious health-related suffering’. The concept was introduced by the Lancet Commission on Global Access to Palliative Care and Pain Relief [63] which outlined 20 diagnostic groups and a range of symptoms needing palliative care [6]. A review of standards and norms for palliative care by the European Association of Palliative Care (EAPC) stated that palliative care should be available to all adults and children with life-threatening diseases (not defined) and highlighted concerns about the use of the emerging concept of serious health-related suffering to describe the objectives of palliative care [26].
The five international palliative care standards and policy statements that were focused on children all drew on key concepts outlined in A Guide to Children’s Palliative Care, by the UK-based charity, Together for Short Lives (TfSL) [1]. In the Guide, CPC need was defined in terms of having a life-threatening condition (for which curative treatment may be feasible but may fail) or life-limiting condition (for which there is no reasonable hope of cure). These conditions were categorised into four groups describing disease progression (Table 5). The groups were first proposed by the Association for Children with Life-threatening or Terminal Conditions and their Families, and the Royal College of Paediatrics and Child Health (ACT/RCPCH) in the first edition of the Guide in 1997. This review included the 2018 (4th edition) Guide which noted that aside from diagnosis, other factors (e.g., spectrum of disease, severity of disease, complications, needs of the individual child and family) should be accounted for when determining CPC need [1].
Table 5 Defining CPC need – policy statements/standardsThe WHO outlined groups of populations and conditions that generate a CPC need [3]. Population groups were defined in terms of disease progression categories which overlap with the ACT/RCPCH groups (Table 5), and condition groups including malignancies, conditions discovered in the perinatal period, injuries, serious infections, genetic conditions, malnutrition, and pain.
The International Standards for Paediatric Palliative Care (Global Overview – PPC Standards 2021, GO-PPaCS) set out general and specific factors in defining CPC need [2]. At the general level, it was agreed that children with life-threatening, life-limiting, or terminal illness may need CPC. Life-threatening/life-limiting were defined as per the TfSL guide and terminal was defined as a condition where death becomes inevitable in children with life-limiting or life-threatening illnesses. Specifically, conditions eligible for CPC were classified into five categories describing disease progression, the first four of which were adopted from the ‘ACT/RCPCH’ groups (Table 5) and the fifth referred to perinatal/neonatal conditions. These standards also stated that diagnosis is not the only important factor and that the complexity of each child and family’s needs are important to consider. The standards further stated that ‘complex chronic conditions’ (CCCs) should also be considered, a concept developed by Feudtner et al. (discussed below) [32]. The need for standardisation of eligibility criteria was emphasised and a list of ‘red flag’ eligibility criteria were described including diagnosis of a life-limiting/life-threatening condition, serious episodes of hospitalisations, use of invasive medical devices, conditions that cause difficulties in pain/symptom management, complex psychosocial and spiritual needs, and difficulties in making significant decisions. The GO-PPaCS were endorsed in the 2022 European Charter on Palliative Care for Children and Young People ([29] pg.2). A recent blueprint for CPC also described CPC need in terms of the ACT/RCPCH groups [27].
Conceptual discussionsSix review papers discussed key CPC concepts including how CPC need is defined [4, 9, 14, 35, 36, 39]. Spicer et al. [36] outlined an agreed set/lexicon of CPC terminology for use in Canada where CPC need was defined in terms of ‘Life-threatening conditions’ [36]. Life-threatening conditions were defined as encompassing life-limiting or life-shortening conditions, and were described in terms of the ACT/RCPCH groups. It was further explained that life-threatening conditions (as per this lexicon) are frequently complex chronic conditions with significant impact on the child/family [36]. Similarly, an overview of core issues in CPC for medical practitioners described CPC need both in terms of complex chronic conditions and the ACT/RCPCH groups [39].
The remaining four of these papers were published within the last 5 years and provide recent perspective on developments in CPC eligibility discussions [4, 9, 35]. Macauley [35] discussed the origins, and drawbacks, of the term ‘life-limiting’, highlighting its disproportionate use in children’s, compared with adults’, palliative care literature. Macauley [35] noted that the term life-limiting could expand the reach of palliative care by encompassing both shortened life and/or burden of disease but pointed out several problems with the term, including its lack of specificity. Jankovic et al. [9] undertook consensus discussions with experts in the field to identify well-defined CPC eligibility criteria that could be implemented in both clinical and organisational/healthcare planning contexts. The authors provided general guidelines for defining incurability in paediatric cancer and non-cancer patients, and outlined other parameters that should be accounted for (i.e., child and family personal and social factors), subsequently cited in the GO-PPaCS [2, 9]. Fraser et al. [4] and Downing et al. [14] discussed advances and challenges in CPC access and research, including challenges associated with defining the eligible population. Fraser et al. [4] highlighted drawbacks of recent approaches that combine adult and children’s palliative care, citing the difference of opinion at the international level about the new definition of palliative care developed by the International Association of Hospice and Palliative Care that draws on the Lancet Commission concept of serious health-related suffering [64].
Category (2) defining & quantifying CPC need – appliedThe review included 38 articles undertaking applied research estimating population-level CPC need. The following sections describe the core definitions of population-level CPC need adopted, noting if/where complexity of need was addressed, and the estimation methods and data sources applied in the studies. (Core methodological characteristics of the applied articles are summarised in Additional File 1.)
Definitions of CPC need in applied literatureThree articles focused on developing a detailed list of diagnoses/conditions that would be considered eligible for CPC, on the understanding that proper planning of services requires detailed information on the population of children who need the services, which in turn requires detailed diagnostic criteria [7, 32, 42]. In each case, the list of diagnoses were coded according to the International Classification of Diseases (ICD10), although different versions were used [65]. A further 16 papers applied or modified these lists to estimate population-level need for CPC to inform service planning [12, 33, 34, 41, 43, 45,
留言 (0)