
記住我
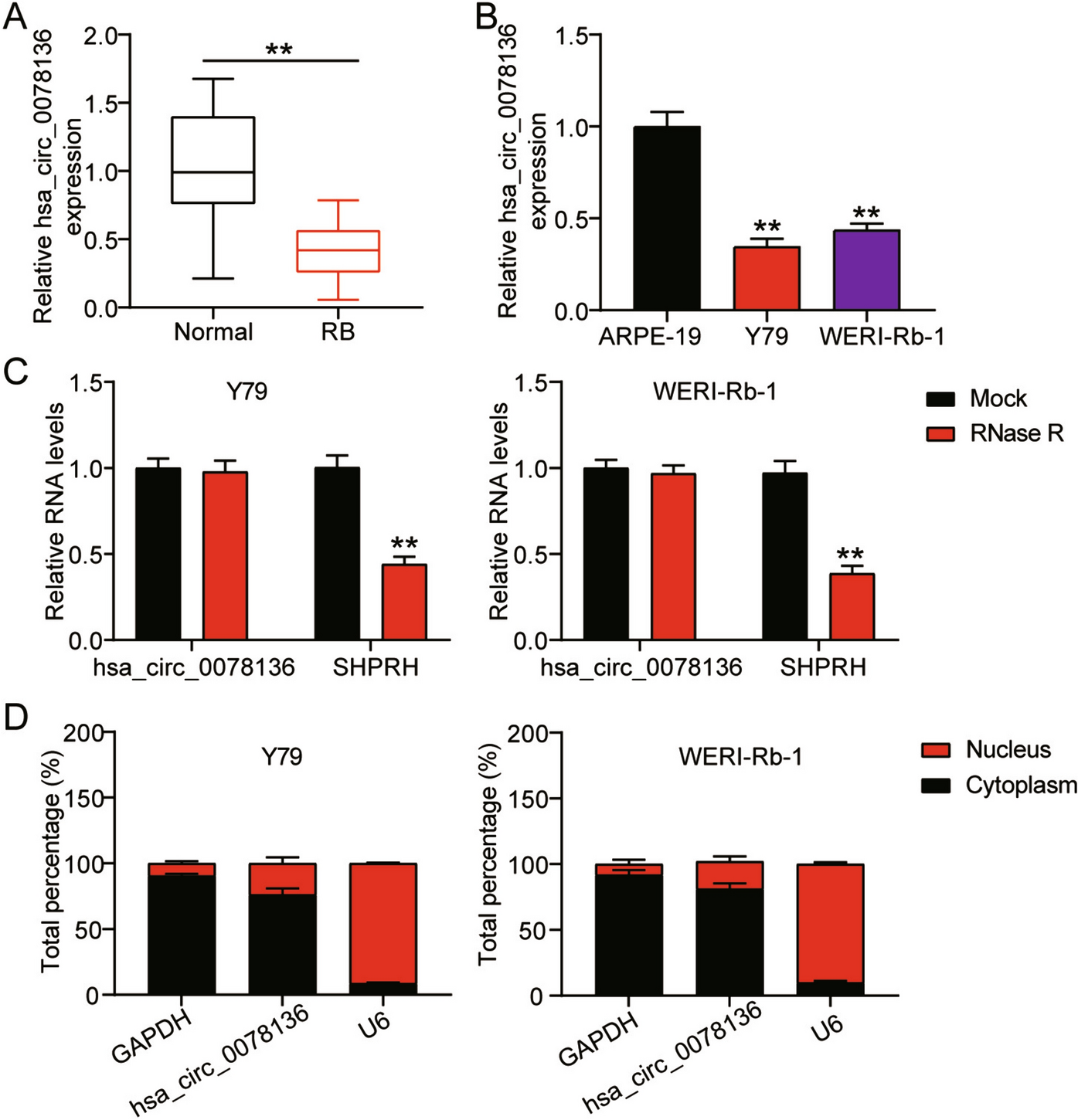





Our database search yielded 1001 records. After removing duplicates, we assessed the titles and abstracts of 727 records. We then conducted a full-text examination of 19 articles, ultimately identifying 15 studies that met our inclusion criteria for systematic review (Fig. 1).
Fig. 1
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) study flow diagram
Design and samplesAmong the 15 studies in our analysis, 11 of these [12,13,14,15,16,17,18,19,20,21,22] explored the impact of a single exercise session. The four remaining studies comprised two randomised controlled trials (RCTs) [23, 24], a comparative study [25], and a single group study [26] that implemented an exercise programme.
Together, these studies encompassed a total of 728 participants. The smallest study featured a sample of six participants [26], while the largest included 145 participants [16]. Except for one study [20], all studies reported the sex of participants, which accounted for 387 males and 329 females. Participants’ ages across the studies ranged from 13 to 78 years.
The Goldmann-Applanation Tonometer emerged as the primary measurement tool utilised in the selected studies [12,13,14, 16,17,18,19,20,21,22,23,24,25]. Furthermore, one study [21] employed a non-contact pneumatonometer (NCT, Canon HY9-RK-F1 Japan, automatic mode), another study [15] used the Perkins hand-held applanation tonometer, and Lipkova et al. [25] utilised Schiotz’s tonometer. However, Lipková & Kyselovičová [26] did not disclose the measurement tool used in their study.
Interventions characteristicsSpecifics about the interventions’ characteristics are provided in Tables 1 and 2. Out of the studies proposing a singular exercise session, aerobic activity was the most prevalent intervention (n = 10). Notably, resistance training was only evaluated in one study [18], and another study [22] analysed the effects of the isometric training. Regarding exercise programmes, three proposed aerobic exercises [23, 25, 26], while a solitary study analysed a programme based on resistance exercises [24].
Table 1 Overview of the studies proposing a training programmeTable 2 Characteristics of studies involving a single exercise sessionFour studies introduced training programmes of variable durations, from a concise 4-week programme [24] to an extended 3-month programme [23, 26]. These studies entailed 2–5 exercise sessions per week, with individual session durations ranging from 30 minutes [23] to 60 minutes [26]. Exercise intensity was typically regulated by maximal heart rate [25, 26] or by one repetition maximum, as in the case of Ibrahim & Elbeltagi [24]. However, Ma et al. [23] omitted details regarding exercise intensity.
Dropouts and adverse eventsFrom the six studies providing information about dropouts, a total of 44 were reported [22,23,24]. Dropout reasons were diverse, encompassing illness, study withdrawal, failure to meet reproducibility criteria, unavailability for follow-up, and subpar exercise performance. Nevertheless, none of the studies notified adverse effects ensuing from the interventions.
Main outcomesSingle session studiesTen out of the 11 studies that employed a single exercise session reported significant effects. Five of these studies displayed a significant intra-group reduction in IOP immediately following the aerobic exercise session [12,13,14,15,16]. In contrast, the study by Gracitelli et al. [19] demonstrated an elevated IOP after the intervention, which persisted for at least 30 minutes. Gillmann et al. [18] found an IOP increase during aerobic activity, lasting from the activity commencement to 120 minutes post-resistance exercise. Notably, IOP was higher 30 minutes after aerobic exercise than immediately post-exercise in three studies [12, 13, 19]. However, others documented a reduction in IOP at 24 minutes [20] and 60 minutes [15] after the intervention. No significant differences in IOP values were found in the sole study implementing isometric exercise [22].
Two out of the 11 studies revealed significant results in inter-group analysis [14, 15, 21]. Yuan et al. [14] showed a more substantial IOP decrease in glaucoma participants compared to healthy participants post-aerobic exercise. Additionally, Umoh et al. [15] reported consistently higher IOP levels in participants with glaucoma across all time points compared to healthy participants. In another study, participants with glaucoma and high myopia exhibited a more significant IOP reduction after aerobic exercise compared to both healthy participants and those with moderate myopia [21].
Meta-analysis of the 12 studies (comprising 388 participants) comparing pre- versus post-intervention IOP mean values from single exercise sessions [12,13,14,15,16,17,18,19,20,21,22] indicated a moderately significant reduction in this outcome (Hedges’ g -0.81 (− 1.58; − 0.03) p = 0.022, albeit with high heterogeneity (I2 = 96.7%) (Fig. 2). Our results further suggested a strong dependence of exercise effects on baseline IOP: higher baseline IOP corresponded to more substantial exercise-induced reductions (Beta = − 0.20; p < 0.001; R2 = 0.626) (Fig. 3). Subsequent analysis of 24 subgroups (n = 701) showed that the IOP-lowering impact of exercise was independent of exercise intensity (Beta = 0.02; p = 0.889; R2 = 0.0003).
Fig. 2
Meta-analysis of single exercise session impact on intraocular pressure
Fig. 3
Regression of basal intraocular pressure (IOP) on effect size
Exercise programme studiesRegarding the effects of exercise programmes, three of the four studies that implemented an intervention programme reported significant effects [23,24,25]. In all three studies, significant intra-group differences were observed. Ma et al. [23] reported a significant reduction in IOP values immediately after the aerobic intervention, but at 3 months post-intervention, IOP increased significantly in the aerobic group compared with irregular exercises group. In addition, Ibrahim and Elbeltagi [24] found significant improvements in IOP results following a resistance exercise-based intervention combined with standard medication. However, Lipkova et al. [25] only detected a significant increase of IOP in one session during the intervention.
Furthermore, only two of the four studies showed significant results in inter-group analysis [23, 24]. According to their findings, IOP tended to be higher in exercise protocols compared to the control group after the interventions.
Quality appraisalOverall, all 15 studies fulfilled most of the criteria outlined by the MMAT for each study design. The two quantitative randomised controlled studies [23, 24] had a MMAT score of 100% and the 13 quantitative non-randomised studies had a mean score of 84.62% (see Table 3).
Table 3 Methodological quality of the included studies according to the Mixed Methods Appraisal Tool (MMAT)
留言 (0)