Study design and setting
This is a sub-study conducted during screening for eligibility of a pilot randomised controlled trial (RCT) (Australian New Zealand clinical trials registry (ANZCTR) ACTRN12619001530112), approved by South Western Sydney Local health district (SWSLHD) human research and ethics committee on June 12th, 2019 (Project identifier 2019/ETH00283), commenced in September 2019 and completed recruitment in January 2023. The current protocol version 3.1 was approved on 11th Nov 2022. All participants provided informed consent. The RCT assessed the feasibility of completing a trial assessing early intervention using continuous positive airway pressure (CPAP) or positional therapy (PT) in pregnant women with an apnoea hypopnoea index (AHI) or respiratory disturbance index (RDI) ≥ 5, by the 16th week of gestation. Secondary outcomes of interest in the RCT include the development of gestational diabetes mellitus (GDM) by 28 weeks gestation, the development of hypertensive disorders of pregnancy, maternal weight gain, uterine artery blood flow, glycemic control during pregnancy (in participants who develop gestational diabetes), changes in maternal circulating biomarkers and neonatal birthweight and complications.
Initially pregnant women were invited to undertake self-applied Level III tests in the home environment and attended Level I (Grael 4 K PSG: EEG, Grael Acquisition system, Compumedics, Abbotsford, Australia) at the sleep investigations unit (SIU) at Liverpool hospital (Liverpool, NSW, Australia) by the 24th week of gestation.
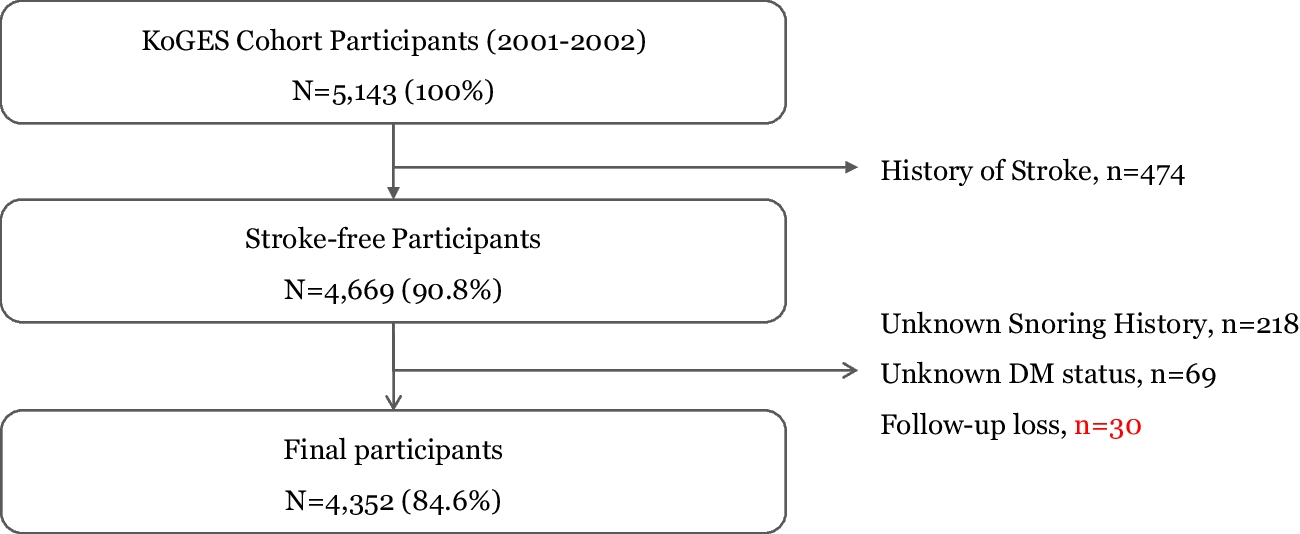
The addition of questionnaires and self-applied at-home Level II were approved by SWSLHD in January 2021, and implemented in March 2021. The thirty-two participants that had already been recruited at that date are not included in this analysis. Participants were screened for eligibility, invited to undertake Level I, level II, level III sleep studies and questionnaires. Participants were recruited from antenatal clinics at Campbelltown and Liverpool hospitals in South Western Sydney, NSW, Australia. Sub studies that we have analysed from this dataset assess the agreement of apnoea hypopnoea index (AHI) scores of Level I and Apnealink Air (level III) (n = 49) [8], and the agreement of AHI and respiratory disturbance index (RDI) of Level I and Somte (level II) (n = 24) [9].
Participants
At or prior to scheduled hospital obstetric bookings, participants were approached in person or by phone by study staff who completed screening eligibility using a research electronic data capture (REDCap) hosted electronic case report form [14]. Eligible participants were provided a participant information sheet by email or hard copy and provided informed written consent. Baseline data that were collected included STOP BANG [15], Epworth Sleepiness Scale (ESS) [16] and Facco’s pregnancy-related tool questionnaire [17]. A fetomaternal physician dated gestation based on the dating scan performed in the first trimester. The study coordinator determined order of testing, based on physical availability of the test devices within a scheduled window of 7 days.
Inclusion criteria for the RCT were defined as (1) women aged 18 years of age and above; (2) In early to mid-pregnancy (up 24 weeks gestation); (3) at increased risk of metabolic complications defined as one or more of: (a) body mass index (BMI) greater than or equal to 35 kg/m2 at screening; (b) previous gestational diabetes mellitus (GDM) [18]; (c) previous personal history of pre-eclampsia (or in mother or sister); (d) underlying renal disease; (e) maternal type 2 diabetes (pre-gestational); (f) symptoms of sleep disordered breathing (SDB) including snoring, witnessed apnoea, mild excessive daytime sleepiness (EDS) (which does not meet the criteria for severe EDS defined by Epworth Sleepiness Scale (ESS) (> 15) or a fall asleep accident or near-miss accident in the previous 12 months) or tiredness. Participants were excluded if they have (1) previous diagnosis of OSA on active treatment; (2) confirmed current GDM or preeclampsia; (3) maternal type 1 diabetes; (4) multifetal gestation, (5) known fetal chromosomal abnormality; (6) inability to provide informed consent; (7) severe EDS based on clinical assessment (e.g. including a fall asleep motor vehicle accident or near miss, transient sleepiness while driving/at lights or needing to pull over due to sleepiness while driving, or transient sleepiness in any other dangerous situation i.e. cooking, carrying baby) or ESS of greater than 15.
Additional inclusion criteria for this sub-study were completion of any questionnaire. Participants who failed to complete any questionnaire were excluded from this analysis. Participants self-applied Level II and III sleep studies in the home environment. Assistance by family member, spouse, or other was allowed but not encouraged. The study coordinator was available on-call for technical phone support during the study set-up and data collection.
Level I (attended PSG) (gold standard)
Participants were set up by experienced sleep technicians in the sleep investigations unit (SIU) at Liverpool Hospital. Level I data were collected between 21:00–06:00 approximately. Level I collection followed American Academy of Sleep Medicine (AASM) guidelines [19] and included EEG (C1/C2 C3/C4, O1/O2, F3/F4, M1/M2), EOG (E1/E2), EMG (chin, diaphragm and anterior tibialis (left and right)), snore (microphone), ECG (modified Lead II), airflow (pressure transducer, thermistor), respiratory effort (abdomen and thoracic), pulse oximeter (SpO2), sound level (decibel meter (dB meter)), digital video (audio and visual) and position sensor. SpO2 was collected using Compumedics adult silicone soft tip probe oximeter 3 m. EEG used gold cup electrodes (Falcon HST Snap Lead (Compumedics, Abbotsford, Australia)), EMG and ECG channels used Falcon HST Snap Leads. At times, gold cup electrodes and snap leads were used interchangeably for EEG (ground / reference), EMG (submentalis).
Level II (unattended PSG) (Somte)
The study coordinator encouraged participants to watch a manufacturer produced YouTube instructional video prior to undertaking the test [20] and educated participants at device collection the application technique and device operation. Level II data collection followed a modified American Academy of Sleep Medicine (AASM) set-up protocol. Collection included EEG (F3/F4, M1/M2), EOG (E1/E2), EMG (submentalis, anterior tibialis (left and right leg)), ECG (modified Lead II), airflow (pressure transducer), snore, airflow (thermistor), respiratory effort (abdomen and thoracic), oximeter (SpO2) and position sensor. F3/4 leads were placed on the forehead for ease of application. SpO2 was collected using Compumedics adult silicone soft tip probe oximeter 1 m. EEG, EMG and ECG channels used Falcon HST Snap Lead.
Level III (unattended) (Apnealink Air)
The study coordinator encouraged participants to read the manufacturer supplied instruction sheet prior to undertaking the test and educated participants at device collection the application technique and device operation. The Level III test data collection included respiratory effort, pulse, oxygen saturation (SpO2), nasal flow and snoring. Micropore tape (3 M™ Micropore™ Surgical Tape 1530–1, 3 M, North Ryde, Sydney, Australia) was issued and participants were instructed to secure air cannula and oximetry probe, using the tape, to the cheek and hand respectively to reduce the chance of lost signals.
Questionnaires
Four questionnaires (one preferred test device questionnaire and three test device questionnaires (PSG (level I), Somte (Level II), Apnealink (Level III)) were developed in English [Online supplement 1a. PSG, 1b. Somte, 1c. Apnealink, 1d. Preferred test]. The questionnaires were beta tested prior to implementation. Beta testing was conducted on hospital staff and feedback was implemented prior to the initiation of the questionnaires. The preferred test questionnaire used a ranking scale (1st, 2nd, 3rd preferred test). Test device questionnaires used a combination of yes/no, 5-point Likert scale responses, and optional linked text fields. Level I, Level II and Level III questionnaires assessed ease of use, convenience, and repeatability on a 5-point Likert scale and used yes/no responses and linked text fields. Additionally, Level II and Level III questionnaires assessed test difficulty and phone support requirements using yes/no responses and linked test fields. Participants who required phone support during Level II and Level III sleep studies were asked to report the helpfulness of the phone support using a 5-point Likert scale.
The study coordinator scheduled questionnaires to be sent via REDcap email to participants on the morning following each scheduled test date, and following the final test, in the case of the preferred test questionnaire. Incomplete questionnaires were reissued at an interval of three days, until completion, up to a total of three times. A hard copy of each questionnaire was included with each test for all participants, and questionnaires could be completed by either hard copy or online method. Participants self-completed questionnaires, but assistance to complete questionnaires was available from the study coordinator if requested by the participant. Questionnaires completed in hard-copy form were entered into REDCap by the study coordinator.
Linked text field responses were not collected for Ease of use, convenience, and repeatability questions for Level II questionnaire due to a coding error in Redcap during questionnaire development.
Statistical methods
Analyses were performed using Statistical Package for the Social Sciences (SPSS), Version 29.0 (IBM Corp., Chicago, Illinois, USA). Descriptive data are presented (based on distribution as assessed by a Shapiro–Wilk test) either as a mean ± standard deviation (SD), median (interquartile range (IQR) / range), or count (n (%)). Rank and Likert-scale questions were scored using Summative scale scores (sum of rank). Linked optional text fields were thematically analysed by the study coordinator and were batched according to theme. Friedman’s tests were used to calculate significance for test preference, ease of use, convenience, and repeatability. Only questionnaires completed are included in this analysis (Complete case analysis).









留言 (0)