
記住我










Candida spp. are commensals colonizing skin and mucosal membranes of oropharyngeal, gastrointestinal and genitourinary tracts of humans1. Based on the host’s immune status, these opportunistic pathogens can cause localized and systemic infections. Invasive candidiasis is a significant cause of mortality and morbidity in immunocompromised and immunocompetent individuals. Some of the major risk factors for Candida infections are prolonged use of antibiotics and hospitalization, diabetes, cancer, HIV/AIDS and immunosuppression associated with transplant recipients2. A recent systematic review estimated that ⁓4.1 per cent of the Indian population, i.e., ∼60 million people, suffer from a serious fungal disease, including candidiasis3.
While Candida albicans (C. albicans) is the most commonly identified infectious species of Candida worldwide, there has been a rise in infections caused by non-albicans Candida species (NACs). Single and multi-species infections by Candida pose a serious public health challenge. Treatment options for managing these infections are limited to a few antifungal drug classes: azoles, polyenes, echinocandins and pyrimidine analogues. The high cost of echinocandins hinders their widespread use in low- and middle- income countries such as India4,5. Amphotericin B causes nephrotoxicity; hence, its use is limited mainly to severe cases of invasive candidiasis6. This has led to an increased use of fluconazole for candidiasis treatment. This dependence on a limited repertoire of antifungal drugs has led to the emergence of multidrug-resistant species such as C. glabrata, C. krusei and C. auris7.
The geographical distribution of infection-causing species of Candida varies. C. tropicalis and C. parapsilosis are the most common NACs in Latin America, whereas C. glabrata is the most common NAC in North America and in some European countries8. C. auris infection, which was first reported in Japan, has been subsequently reported in 47 different countries, including India9. Age can also influence the type of Candida infection. C. parapsilosis is more commonly isolated from neonates and infants as compared to adults10. Depending on the microenvironment and comorbidities, Candida spp. can infect most human body organs, leading to conditions like oropharyngeal candidiasis, vulvovaginal candidiasis or candidemia. Oropharyngeal candidiasis is the most common fungal infection reported in people suffering from HIV/AIDS11, whereas diabetic females are more likely to suffer from vulvovaginal candidiasis12.
Candida spp. is a leading cause of nosocomial infections worldwide. Numerous clinical reports related to candidiasis diagnosis, management and outcomes have been published in India. However, this information has not been systematically curated for further analysis. The Centers for Disease Control and Prevention website provides data on Candida epidemiology in the American population. ClinEpiDB, an open-access database to explore and visualize epidemiology studies around the world13, does not contain any information on Candida or candidiasis. Other resources for Candida include non-epidemiological databases like the Candida Genome Database (CGD) and CandidaDB. CGD is an open online resource containing gene, protein and sequence-related information about multiple species of Candida, such as C. albicans, C. auris, C. glabrata14. CandidaDB, a database for genomic data on C. albicans and other related yeasts, has been discontinued15. Currently, no web resources showcase the epidemiology of Candida infections in India. To address this gap, we have developed EpiCandIn, an online curated compilation of Indian clinical reports of Candida infections.
EpiCandIn was created by manually curating scientific publications from 1972 to 2022 that report the prevalence of Candida infections, pathogenic species, organs affected, mode of treatment, mortality and antifungal susceptibility profiles of Candida isolates in different geographical locations of India. This resource will be useful for clinicians and policymakers to understand the changing trends of Candida infections and design appropriate management strategies.
Material & MethodsThe study was undertaken at the Biomedical Informatics Centre, ICMR-National Institute for Research in Reproductive and Child Health, Mumbai, India.
Screening publications for data extractionPubMed and ScienceDirect databases were searched to obtain articles pertaining to Candida research in India published till December 31, 2022. The search query used for PubMed was ‘((Candida [Title]) OR (Candidemia [Title]) OR (Candidiasis [Title]) OR (Candiduria [Title])) AND ((India [Title/Abstract]) OR (Indian [Title/Abstract]) OR (India [Affiliation]))’. The search query used for ScienceDirect was ‘Title: Candida OR Candidemia OR Candidiasis OR Candiduria, Author Affiliation: India’.
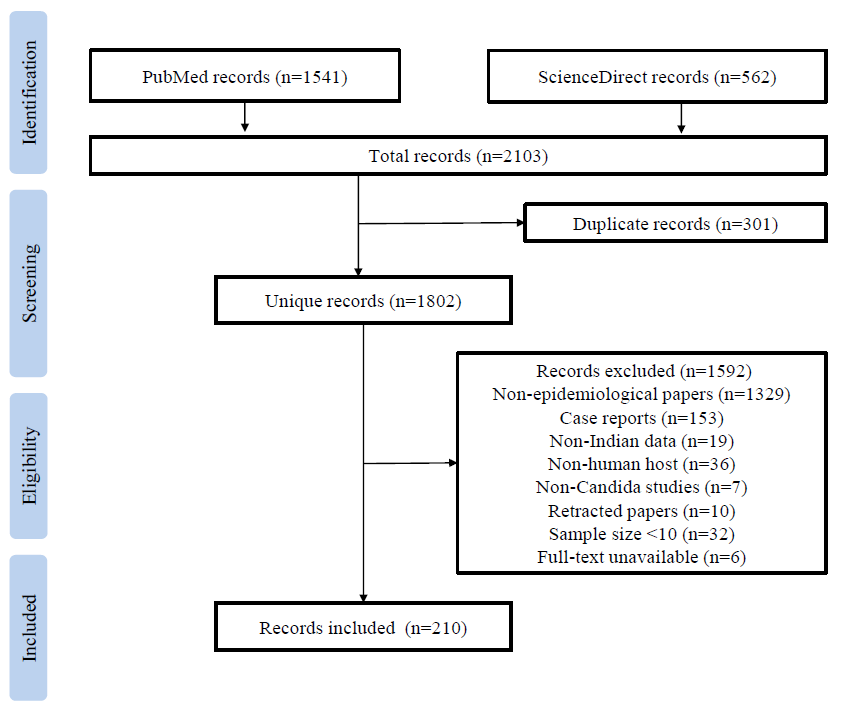
The abstracts of all articles were manually curated to include original scientific reports of Candida infections in the Indian population. Publications on Candida infections for which full text was not accessible were rejected. Publications with inconsistencies in the data reported in different article sections were rejected. Publications reporting non-epidemiology data, epidemiology data from non-Indian patients, data obtained from in silico, in vitro or in vivo models were excluded. The workflow adopted for this study is shown in Figure.
Export to PPT
Manual curation and data extractionAll the eligible publications were manually curated to extract the following information: author names, publication year, study duration, study design, clinical setup, geographical location, comorbidities, risk factors, species, type of candidiasis, niche infected, symptoms, antifungal drugs prescribed, age and sex of participants, number of patients, number of Candida isolates, identification methods, antifungal susceptibility profiles, methods of antifungal susceptibility testing, prevalence, and mortality.
Rules adopted for redundancy elimination in the database are listed in Supplementary Table I. The organs infected with Candida spp. and the type of candidiasis was determined as per the collected culture-positive biological samples (Supplementary Table II). The spellings of species names have been corrected as per NCBI Taxonomy database16. If a species name was not available in NCBI Taxonomy database, the most frequently used spelling was selected (Supplementary Table III).
Data analysisDue to a lack of uniformity in the sample collection and reporting methodology, statistical analysis could not be performed on the collated data. Data visualization packages such as ggplot2 library in R software (cran.r-project.org/web/packages/ggplot2/index.html) were employed to gain insights from the database.
Database architectureEpiCandIn is built on Apache HTTP Server 2.4.51 with MySQL Server 5.7.36 as the back-end and PHP 7.4.26, HTML and JavaScript as the front-end. D3.js JavaScript library was used for data visualization.
Results & DiscussionCandidiasis is among the most common nosocomial infections observed in India and globally. The clinical presentation and aetiology of candidiasis are dependent on the medical history, age, organs affected and the geographical area of the individuals2. Hence, it is important to assess and comprehend the evolving landscape of Candida infections in India. We have compiled clinical data from pan-India reports of Candida infections and presented it in a user-friendly online format through EpiCandIn.
EpiCandIn has a simple, user-friendly interface that facilitates navigation through the database. EpiCandIn can be accessed freely at epicandin.bicnirrh.res.in. The interface includes search, browse and visualization options for geographical location, species, affected niches and antifungal drugs.
HomepageThe Homepage of EpiCandIn contains an interactive map of India. The geographical sites contributing the data in EpiCandIn are highlighted on the map. Clicking on these sites will provide a tabular view of epidemiology studies and associated details from the selected locations. Quick links to access studies related to individual species, niches and antifungal drugs are also available here.
Search & downloadUsers can avail the simple or advanced search options to query the database. Simple search is through keyword check on all fields and advanced search functions through query builder wherein keywords are searched based on the specific fields defined by the user. Users can also download the data in a tabular format.
SubmitThrough this portal, clinicians and researchers can submit epidemiological data on Candida infections from India along with the associated publications. This data will be manually curated and verified for inclusion and subsequent data extraction for EpiCandIn updates.
The literature search yielded 2103 results, comprising 1541 articles from PubMed and 562 articles from ScienceDirect. After removing 301 duplicate articles, the remaining 1802 publications were manually reviewed, and 210 eligible papers were included in the EpiCandIn database. It contains data from 51 sites in 16 States and four Union Territories of India. These studies provide information on 38 unique Candida species isolated from 25 different host niches (Supplementary Table II) reported over a span of five decades.
The major challenge during data curation and extraction was the incomplete or missing information in the retrieved publications. The data on geographical location, gender, treatment modalities and outcome were missing in several papers. In the case of studies spanning multiple years, the observations were not segregated year-wise. With respect to age as a parameter, several articles used terms such as ‘neonates’, and ‘reproductive-aged women’ without indicating the exact age. A few reports mentioned a broad range of 1–88 yr17, 0–80 yr18 and 0–70 yr19 for the study participants. Notably, we did not find any published clinical reports on candidiasis from Himachal Pradesh, Bihar, Jharkhand and the northeastern States (except Assam).
A limitation of this study is the absence of statistical analysis because of the lack of uniformity in sample collection and data reporting across the publications. These issues have restricted the analytical scope of the data present in EpiCandIn. Therefore, a simple analysis of the data was performed, which revealed the following: (a) C. albicans is the most reported species for candidiasis followed by C. tropicalis, C. glabrata and C. parapsilosis (Supplementary Fig. 1 and 2); (b) clinical reports on C. auris and other NACs increased since 2011 (Supplementary Fig. 1); (c) blood was the most well-studied niche followed by the oropharynx and genitourinary tract (Supplementary Fig. 3 and 4); and (d) fluconazole was the most widely prescribed antifungal drug, followed by amphotericin B (Supplementary Fig. 5).
We observed a shift from simple microscopic and culture-based methods to more sophisticated molecular techniques such as polymerase chain reaction (PCR), DNA sequencing and matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometry for the detection of Candida species over the last two decades. This may have contributed to improved species-level identification, leading to a rise in reports on NACs such as C. auris since 201120. These species were identified mostly from the blood, oral cavity and genitourinary tracts (Supplementary Fig. 4), probably due to the ease of sample collection. Candidiasis management heavily depended on fluconazole and amphotericin B (Supplementary Fig. 5). Despite the rise in azole-resistant Candida isolates, fluconazole has remained the most widely prescribed antifungal drug for candidiasis in India over the years (Supplementary Fig. 5). This indicates the urgent need for expanding the antifungal therapeutic options through new drugs and targets. The World Health Organization has stressed upon the need for reports and evidence to understand the burden of infections with regard to the prevalence and antifungal resistance to strengthen global health policies21.
This study is the first step towards developing a unified platform for studying the epidemiological landscape of candidiasis in India. EpiCandIn will enable researchers, clinicians and policymakers to browse the data on Indian clinical reports and draw insights on the increasing burden of Candida infections. Periodic updates of this database with clinical data will enable us to strengthen the candidiasis management strategies in India.
留言 (0)