Study protocol
For this cross-sectional observational study, participants (n = 226) were recruited from patients attending a dedicated BP clinic after referral from their general practitioner from Hobart, Tasmania, Australia. Referred patients typically had known or suspected hypertension and were referred for a detailed BP assessment and recommendations for management by specialist doctors. Provision of the BP values recorded by the referring doctor was a requirement and these BP values were used as the clinic BP. On attendance at the dedicated BP clinic, unobserved AOBP measurement was undertaken using an established protocol [12], and the same BP measurement device was used for 24-h ABPM at the end of the same clinic visit. Cholesterol levels were obtained from blood test reports from accredited pathology services. Additional CVD risk factors and medications were assessed via self-report questionnaire. Separate absolute CVD risk scores were calculated using the systolic BP from each measurement method (clinic BP, unobserved AOBP and ABPM). The proportion of participants classified as high risk in accordance with the 2012 Australian guidelines [1], and compared across the BP measurement methods. As a dedicated clinic for patients with suspected hypertension or suspected uncontrolled hypertension, many participants were taking anti-hypertensive medications on presentation to the BP clinic. All patients maintained their usual medication schedule between referral to the BP clinic and the clinic visit where AOBP and ABPM measures were obtained. All participants provided written informed consent and ethical approval was obtained from the Tasmania Health and Medical Human Research Ethics Committee.
Clinic BP
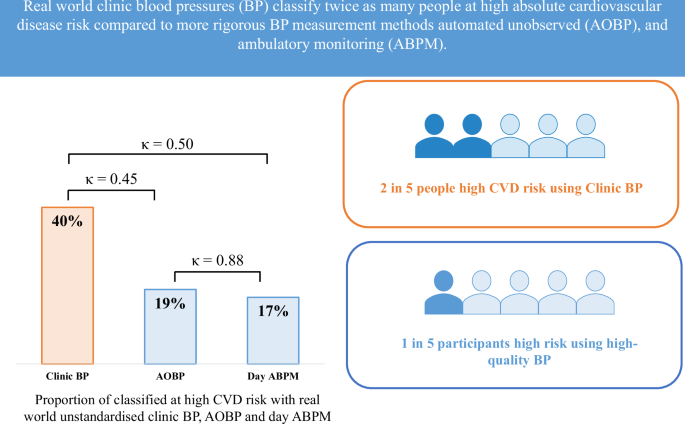
Clinic BP was recorded as part of the referral process and measured in the clinic environment according to the usual practice of each referring doctor from general practice. Thus, clinic BP was not standardised and represents a real-world clinic BP measurement, instead of a standardised research-grade clinic BP as recommended to be performed by hypertension guidelines [13]. No information was available on the rest period before or between clinic BP measurements, nor the device used for clinic BP measurement. Typically, one clinic BP reading was provided, in some instances a second or third BP measurement was available. Where more than one clinic BP measurement was available the average was used for analyses.
Unobserved AOBP
A validated automated BP device was used to obtain three unobserved AOBP measurements after 5-min of seated rest, with one-minute rest between each measurement (Mobil-O-Graph, IEM, GmbH) [12]. Participants were fitted with an appropriately sized BP cuff (based on arm circumference measurements) in a private room and advised to sit quietly with both feet on the floor, back supported and arm at heart level while the BP device automatically measured and recorded unobserved AOBP. The average of the second and third unobserved AOBP measurement was used for absolute CVD risk calculation [14].
ABPM
The same BP device used for the unobserved AOBP protocol was also used to record ABPM (Mobil-O-Graph, IEM, GmbH) [12]. Before leaving the clinic, participants were fitted with the BP device and advised to avoid removing the cuff for the 24-h ABPM period. ABPM measurements were recorded every 20 min during the day (6am–10pm) and every 30 min at night (10pm–6am). As per guideline recommendations, participants were advised to avoid talking or moving during each BP measurement and to avoid strenuous activities during the 24-h monitoring period [15]. The average of the daytime and 24-h ABPM were used for absolute CVD risk calculation.
White coat hypertension
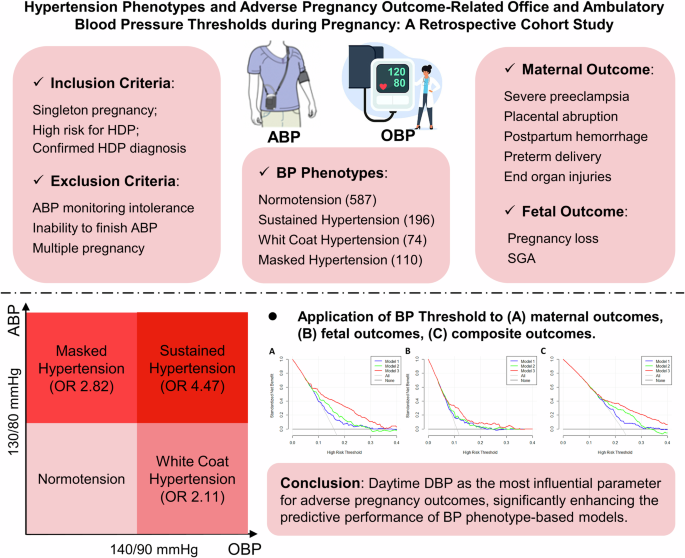
Participants were classified with white coat hypertension if clinic BP was ≥140/90 mmHg and 24-h ABPM was <130/80 mmHg [16]. Sustained hypertension was classified as both clinic-BP ≥ 140/90 mmHg and 24-h ABPM ≥ 130/80 mmHg. Normotension was defined as both clinic BP and 24-h ABPM < 140/90 mmHg and <130/80 mmHg, respectively.
Absolute CVD risk factor variables
Absolute CVD risk scores were calculated using the adjusted 5-year Framingham Risk Equation according to Australian CVD primary prevention guidelines [1, 3]. In addition to systolic BP, calculation of absolute CVD risk using the Framingham equation requires age, sex, smoking status, diabetes status, and total- and high-density-lipoprotein cholesterol.
Fasting cholesterol results were obtained from previous pathology test results on referral. For participants that did not have a recent cholesterol result (within 2 years) a sample of blood was drawn for analysis via an accredited pathology laboratory.
A health questionnaire was completed for all self-reported risk variables. Diabetes status was defined as being previously diagnosed by a medical practitioner and smoking status was defined as a current smoker or a participant who had quit smoking within the last 12 months. Height and weight were also recorded at the clinic visit.
Absolute CVD risk calculation
Age, systolic BP, and cholesterol values were input as continuous variables. Sex, diabetes status and smoking status were entered as dichotomous variables. Four risk scores were produced for each participant with the systolic BP from each measurement method: clinic BP, unobserved AOBP, and ABPM (24-h and daytime). Participants were classified as low, moderate or high absolute CVD risk according to guideline thresholds (<10%, 10–15% and >15%, 5 year risk, respectively) [1]. In addition, participants were classified as high-risk if they reported any of the clinical criteria that denote high-risk without the need for absolute CVD risk calculation as per guideline recommendations [1]. These clinical criteria included: diabetes and aged 60 years or older, BP ≥ 180/110 mmHg, total cholesterol >7.5 mmol/L. Thresholds for hypertension for out-of-office BP measures are typically lower compared to office measures. As such, an additional analysis was conducted with AOBP and ABPM adjusted with an increase of 5 mmHg and absolute CVD risk calculation and classification undertaken as per the above steps. In addition, a lower BP threshold of ≥160/100 mmHg for AOBP and ABPM was used to classify participants at high CVD risk but the BP threshold of ≥180/110 mmHg was maintained for clinic BP to determine differences in risk classification and agreement.
Statistical analyses
Analyses were performed in Stata version 16.1 (StataCorp, USA). Data are presented as mean (±SD) for continuous variables and as number and percentage for categorical variables. The absolute difference in absolute CVD risk scores calculated with each systolic BP were summarised and compared using the non-parametric Wilcoxon signed-rank test. Clinical significance was determined using the Cohen’s Kappa statistic (κ) to test agreement in high-risk classification according to BP, AOBP and ABPM. A κ of 0–0.20, 0.21–0.39, 0.40–0.59, 0.60–0.79, 0.80–0.90 and >0.90 was considered none, minimal, weak, moderate, strong and almost perfect level of agreement [17]. This equates to 0–4%, 5–15%, 16–35%, 36–63%, 64–81% and 82–100% of data that are reliable for none, minimal, weak, moderate, strong and almost perfect level of agreement, respectively. A sensitivity analysis was undertaken using only first clinic BP measurement for all participants compared with using the average clinic BP when more than one measurement was available. In addition, due to the relationship between advancing age and both systolic BP and absolute CVD risk a sub-analysis was undertaken to determine the effect of age on changes in CVD risk classification. T tests were used to compare continuous variables and Chi-squared tests were used to compare categorical variables.

留言 (0)