Pouch vaginal fistulae, which are highly symptomatic and distressing for patients, are difficult to treat and often an indication for pouch revision or excision. We found that CPA was a viable option for patients who had failed previous interventions for PVF repair, with 44% of patients living stoma-free and fistula-free at the time of follow up. In a meta-analysis of PVF by Machin et al., a total of 577 PVFs from 13 studies were reviewed, with an PVF incidence rate of 2.1–17.1% [1]. They observed an overall success rate for abdominal vs. local repairs of 60.2% and 44.9%, respectively.
Despite the limited success rate of transanal repairs compared with transabdominal repairs observed in this meta-analysis, transanal sphincter-preserving options are attractive to surgeons and patients alike to avoid the increased morbidity invariably associated with transabdominal repair. As with any handsewn anastomosis, patients undergoing CPA should be counseled regarding the possibility of nocturnal seepage, particularly when deeply asleep. The success rate of CPA is likely improved with the protection of a diverting loop ileostomy, as prior studies have demonstrated its effectiveness in aiding the healing process, especially if initial treatment attempts have failed. While stoma utilization was very high in our study (77.8%), our data are limited in number to definitively state that the CPA success rate is significantly impacted by the presence of a defunctioning ostomy. The two un-diverted patients in our study eventually required temporary DLI or pouch excision, suggesting that diversion at the time of CPA may have been beneficial. Both diversion and seton placement prior to CPA were left to surgeon discretion. Notably, 55% of our patients had draining setons in place at the time of CPA, but it is unclear if this is required prior to CPA; of those with setons prior to CPA, the healing rate was 40%.
To date, few studies have been published on full thickness transanal CPA for PVF, other fistulae, or anal canal strictures. Fazio and Tjandra first described transanal mucosectomy with pouch advancement for dysplasia or cuffitis in 1993 in two patients [6]. In terms of outcomes, both patients had intact continence with nocturnal minor seepage of liquid stool, and neither developed a stricture. In 2001, Zmora et al. described eight patients who underwent CPA, four of whom required transabdominal mobilization as well, with a success rate of 62% which is slightly higher than our rate of 44.4% [7]. Similar to Fazio et al., they reported good functional results in 63%. Mallick et al. also described a 50% success rate with utilization of pouch advancement flaps [9]. Anal canal strictures may also be treated with CPA, as reported by Prudhomme et al. in 2003, who reported on five patients who required transanal excision of the stricture and mucosal advancement in which the strictured segment was excised and a flap of ileal mucosa advanced [8]. CPA may not only have a place in the management of PVF but may also serve as a viable option for additional perianal pathologies, especially recalcitrant strictures in this high-risk population of patients with inflammatory bowel disease.
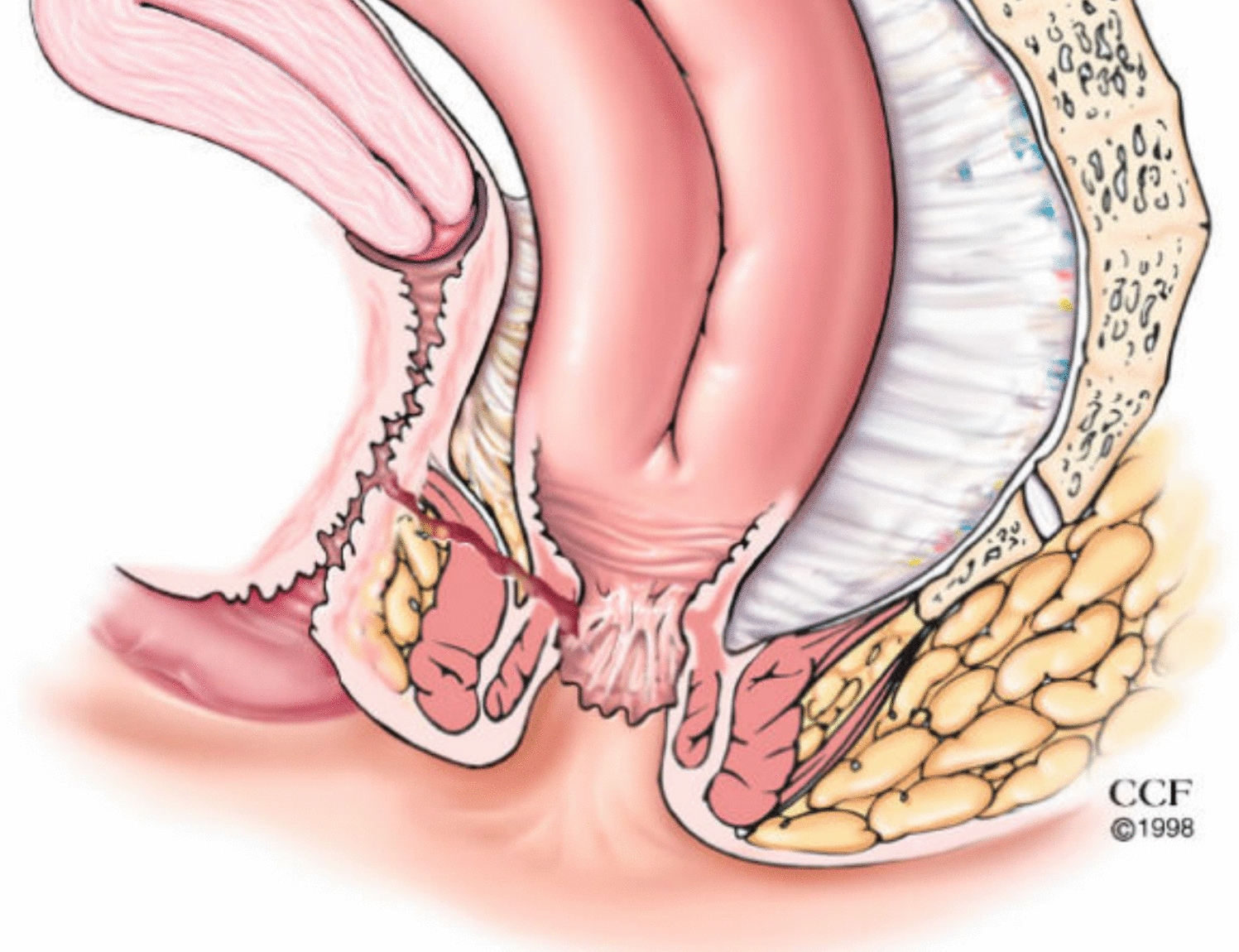
The etiology and timing of the development of a PVF may impact the success of CPA. PVF may occur because of inadvertent incorporation of the posterior vagina wall into the pouch-anal anastomosis during firing of the circular stapler (Fig. 2) [1, 2]. An early PVF at the level of the anastomosis would be the expected result of this technical complication, although paradoxically all the anastomotic PVF in our study presented late suggesting this was not the case. All these patients were ultimately diagnosed with CD, which may account for this delayed presentation. The late development of these fistulae (32 months) suggests CD was the etiology for the majority. More distal manifestations of vaginal fistulas may be a result of inflammation and fistulization related to cuffitis or CD of the anal canal. If present, such inflammation mandates systemic treatment with biologic or small-molecule medications prior to the attempted repair. While patients with anastomotic PVF and those with fistulae distal to the anastomosis both had clinical success in our study, it remains unclear if CPA success is dependent on the location of the fistula [3].
Our study has several limitations. As a result of its retrospective nature, the technical aspects of the CPA were derived from operative reports which may have been limited in detail. The long study period and number of operating surgeons may have resulted in variation in techniques and outcomes. Technical issues, such as inadvertent stapling of the vagina during IPAA creation, were unable to be determined retrospectively. Patients’ follow-up was also limited to our own medical records, and functional outcomes and long-term follow-up (> 1 year) were limited.


留言 (0)