
記住我








A 57-year-old female patient had previously undergone a laparotomy for an ovarian cyst in her 20s. At 46 years, due to adhesive small bowel obstruction (SBO), adhesiolysis without bowel resection was performed. However, her symptoms did not improve. Eighteen days postoperatively, a reoperation was performed for SBO; nonetheless, she only underwent a jejunostomy, due to the severe adhesions. Subsequently, 31 days after the primary surgery, leakage of intestinal fluid was observed from the laparotomy wound; and an ECF developed (Fig. 1A). Three months thereafter, resection of the ECF with stoma closure was planned. However, due to the severe adhesions, only stoma closure was performed, based on intraoperative assessments. Post-stoma closure, festering and ulceration of the peristomal skin worsened, resulting from leakage of the intestinal fluid from the ECF.
Fig. 1
Enterocutaneous fistula (ECF) is depicted. A State of the ECF at the time of referral to our hospital is shown. B State of the ECF after skin care is shown
Consequently, as a result of difficult management, the patient was referred to our hospital. First, skin care around the fistula was performed, during an outpatient visit; the stoma pouch was appropriately sized with the use of skin protectants, to prevent contamination around the ECF and to improve skin erosions and ulcers (Fig. 1B). No other treatments such as negative pressure wound therapy were applied. Eighteen-month post-stoma closure, debridement of the perifistula skin and simple closure of the ECF outlet were attempted. Nevertheless, the ECF recurred shortly postoperatively. For the subsequent 8 years, the ECF remained stable with regular skin care. Regarding nutritional status upon referral, the albumin level was 3.5 g/dL, lymphocyte count was 1.0 × 103/μL, hemoglobin level was 9.5 g/dL, and cholinesterase level was 189 U/L. Using magnesium oxide and kampo, such as Daikenchuto, and by encouraging oral intake, primarily of soft foods, these parameters improved to normal ranges approximately 4 months after referral to our hospital. The output of intestinal fluid from the ECF was controlled and did not exceed 600 mL/day. The patient experienced symptoms of SBO approximately four times a year. However, she persistently refused to undergo surgery.
Ten-year post-stoma closure, the patient underwent radical surgery. Enteroclysis revealed a strong flexure near the ligament of Treitz (Fig. 2A), and computed tomography (CT) confirmed the presence of a mass of dilated bowel, inferior to the fistula (Fig. 2B). Using a tube guide, a long tube was inserted into the upper jejunum preoperatively for intraoperative evaluation of the bowel passage. After careful preoperative simulation, we planned to perform laparoscopic adhesiolysis around the abdominal wall and mobilization of the pelvic small intestine, thereafter, to convert to an open surgery and evaluated the bowel passage, and subsequently to perform adhesiolysis, resection and anastomosis of the intestines.
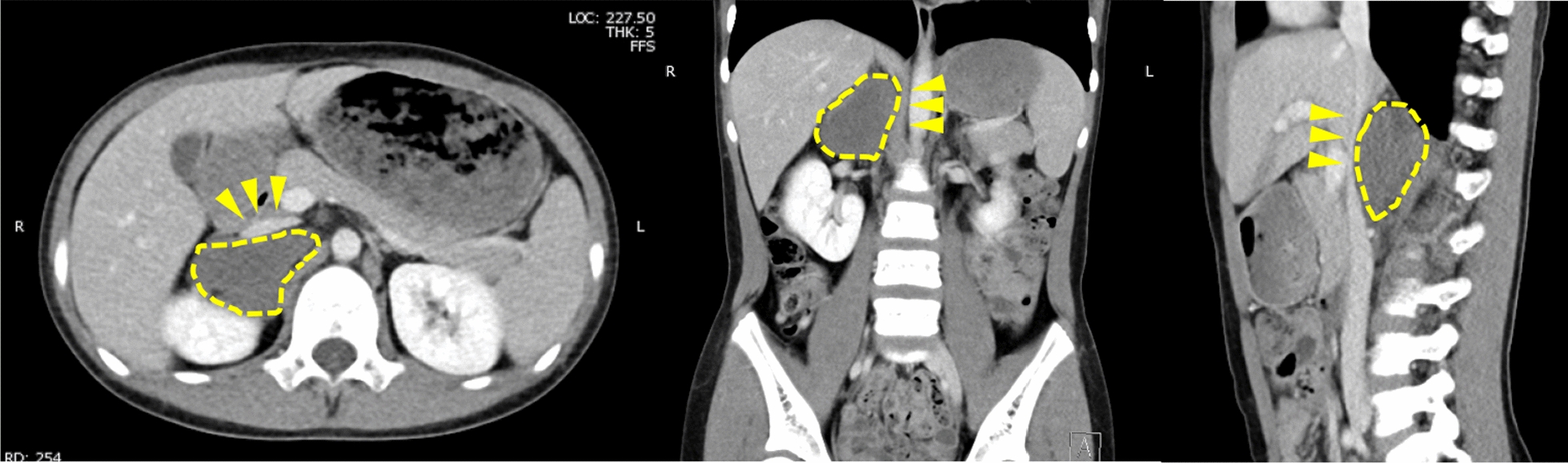
Fig. 2
Preoperative imaging examinations are depicted. A Enteroclysis revealed stagnation of contrast medium in the jejunum near the ligament of Treitz due to strong flexion. (D: dorsal position V: vertical position). B Computed tomography revealing a mass in the dilated bowel, inferior to the fistula. The yellow arrows indicate the presence of an enterocutaneous fistula
The patient underwent adhesiolysis and a partial resection of the small intestine at four locations, including the fistula site. The operative time was 634 min, and blood loss was 710 mL. An initial incision was made in the upper abdomen, which was far from the previous wound, and fewer adhesions were anticipated (Fig. 3A). The adhesions in the upper abdomen were not severe (Fig. 3B). Conversely, as postulated, extensive, severe adhesions were found in the lower abdomen (Fig. 3C). The patient underwent laparoscopic dissection of the strong adhesions surrounding the fistula site; dissection of the adhesions, between the abdominal wall and intestine; and mobilization of the pelvic small intestine. Post-open conversion, the adhesions between the intestines were dissected (Fig. 3D). By careful assessment of the entire small intestine inferior to the ligament of Treitz, the ECF was located, 35 cm from the anal aspect of this ligament. The balloon of the long tube was dilated to 15 mm-in-diameter and passed through the terminal ileum, to evaluate for the presence of stenoses and obstructions. The small intestine with difficulty passing through the balloon (four sites in total) were resected and anastomosed (Fig. 3E). A long tube was placed near the anal aspect of the anastomosis. The remaining part of the small intestine was 285 cm-in-length. After confirming blood flow within the remnant bowel, using indocyanine green fluorescence, a skin defect was formed at the fistula site; and the wound was closed.
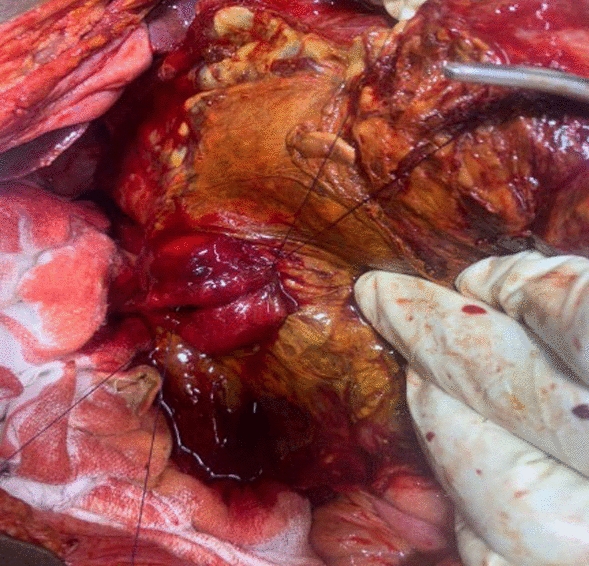
Fig. 3
Intraoperative findings are presented. A Diagram depicting the skin incision. B Upper abdomen has fewer adhesions to the abdominal wall. C Lower abdomen has severe adhesions. D Dissection between the intestines has been performed under an open conversion. E Diagram illustrating the surgical procedure. Four sites of the small intestine have been resected and anastomosed
After confirming the presence of flatus, the long tube was removed. However, repeated episodes of vomiting were observed. The enteroclysis confirmed the absence of organic obstruction of the bowel passage; nonetheless, inadequate peristalsis of the jejunum near the ligament of Treitz and dilatation of the oral aspect of the intestine were revealed. A CT image showed narrowing of the superior mesenteric artery (SMA) with dissociation and intestinal edema (Fig. 4A, left). After a discussion with the interventional radiologists, conservative treatment was continued, because intestinal blood flow was preserved.
Fig. 4
Postoperative course is depicted. A Computed tomography (CT) indicating narrowing of the superior mesenteric artery (SMA) with dissociation (left). At 7 months postoperatively, CT reveals that the narrowing of the SMA has resolved (right). B Surgical scar is depicted
However, the patient’s symptoms did not improve, and percutaneous endoscopic gastrostomy (PEG) was performed, to drain fluid in the dilated intestine. Her symptoms gradually resolved with regular drainage and with the use of acotiamide hydrochloride hydrate, mosapride citrate hydrate, and kampo medicines, such as Saireito and Daikenchuto. She could tolerate oral intake 2 months postoperatively and was discharged from the hospital 3 months postoperatively. Seven months postoperatively, the PEG was removed after several days of non-use and in the absence of a recurrence. Moreover, a CT image showed resolution of the SMA narrowing (Fig. 4A, right). Three years postoperatively, the patient progressed without recurrence of the ECF or SBO (Fig. 4B).
留言 (0)