
記住我



Managing Atelectasis otitis media poses significant challenges for otologists. The progression of retraction in this condition often leads to adherence of the atrophic membrane to the incus and stapes, increasing the risk of ossicle necrosis. Additionally, the TM may adhere to various parts of the middle ear, extending into the sinus tympani, superiorly into the attic, and inferiorly into the hypotympanum. Besides, retraction pockets in the tympanic membrane hold clinical significance as they contribute to the pathophysiology of middle ear cholesteatoma formation. Therefore, accurate diagnosis and proper management of these retraction pockets are crucial to prevent complete ossicle erosion and the formation of cholesteatoma [1,2,3,4,5,6,7,8,9,10].
Several authors advocate for conservative treatment in patients classified as Sadè Grade I and II or those with limited conductive hearing loss. Surgical intervention is often considered in Grade III or IV cases or in situations involving recurrent otorrhea or signs of progressive cholesteatoma [7,8,9].
Traditionally, atelectasis otitis has been managed through microscopic tympanoplasty using retro-auricular or trans-meatal approaches. However, in recent years, the endoscope has gained prominence in middle ear surgery [26,27,28]. The enhanced visualization provided by the endoscope, particularly the ability to view areas 'around the corner,' makes ESS an excellent approach for treating various middle ear disorders. Structures like the retrotympanum, anterior epitympanum, and middle ear folds, which are typically challenging to access, become more visible and accessible with endoscopic assistance [14,15,16,17,18]. While advantages and disadvantages of EES in chronic otitis media and cholesteatoma have been discussed in various papers, scientific evidence regarding the application of EES in atelectasis otitis media remains limited [22,23,24].
Marchioni et al. [24] conducted a preliminary study focusing on exclusive endoscopic tympanoplasty in patients with attic retraction pockets. They reported successful endoscopic dissection of the retraction pocket in all 27 subjects, removing the disease from the epi-tympanic region while preserving the mastoid bone and epitympanic-mastoid mucosa. Follow-up visits revealed a well-ventilated attic space in 21 of 27 (77.7%) subjects, with no retraction pockets found. In 5 of 27 (18.5%) subjects, a moderate retraction on the isthmus region was observed, maintaining good attic ventilation.
Guo et al. [23] presented a retrospective analysis of 17 patients with adhesive otitis media treated by EES. They reported excellent surgical outcomes, with all patients showing good tympanic membrane graft attachment, no retraction, or perforations observed at follow-up. The mean postoperative air-conduction hearing threshold (49.06 ± 22.15 dB hearing level) and mean air–bone gap (19.94 ± 10.00 dB HL) were significantly improved compared to preoperative values (65.29 ± 21.53 and 32.53 ± 8.21 dB HL, respectively; p < 0.05). No recurrences, secondary cholesteatomas, or secondary surgeries were reported at follow-up.
Parab et al. [22] described the treatment of 41 patients with retractions pockets surgically treated using two handed trans-canal endoscopic cartilage tympanoplasty with endoscope holders. At the 3-year clinical follow-up, no recurrence of retraction was observed. The preoperative air–bone gap was 24.53 ± 4.326 dB, improving to 14.57 ± 3.88 dB at the same follow-up period.
Despite these limited studies, there remains a lack of comprehensive investigations with larger sample sizes evaluating the surgical effectiveness of oto-endoscopic tympanoplasty for adhesive otitis media. Our study aims to contribute to the current understanding and effectiveness of ESS in managing atelectasis otitis media [29, 30].
In our study, ESS achieved an estimated graft success rate of 95.5% for treating atelectasis otitis media. At clinical follow-up, 2 patients experienced TM perforation (at 6 and 12 months post-surgery), and 1 patient had a recurrence of atelectasis TM (16 months after surgery), resulting in an 88.8% success rate at final follow-up. The average preoperative air-conduction thresholds decreased from 51.1 ± 21.5 to 34.6 ± 22.1 (p = 0.04) at follow-up, while the preoperative air–bone gap reduced from 28 ± 7.2 to 11.8 ± 10 (p = 0.002). These data closely align with the findings described by Parab et al. [22] and Guo et al. [23] reported above. The analysis of the postoperative pain showed as 36 (80%) of the patients reported ‘no pain’ after surgery, a quite high percentage.
In contemporary literature, authors have documented a lack of recurrence in 67–74% of patients with grade III and IV retraction pockets who undergo tympanoplasty using a microscopic approach. Interestingly, these statistics closely resemble those previously reported regarding the use of Endoscopic Ear Surgery (EES) for adhesive otitis media (AtOM).
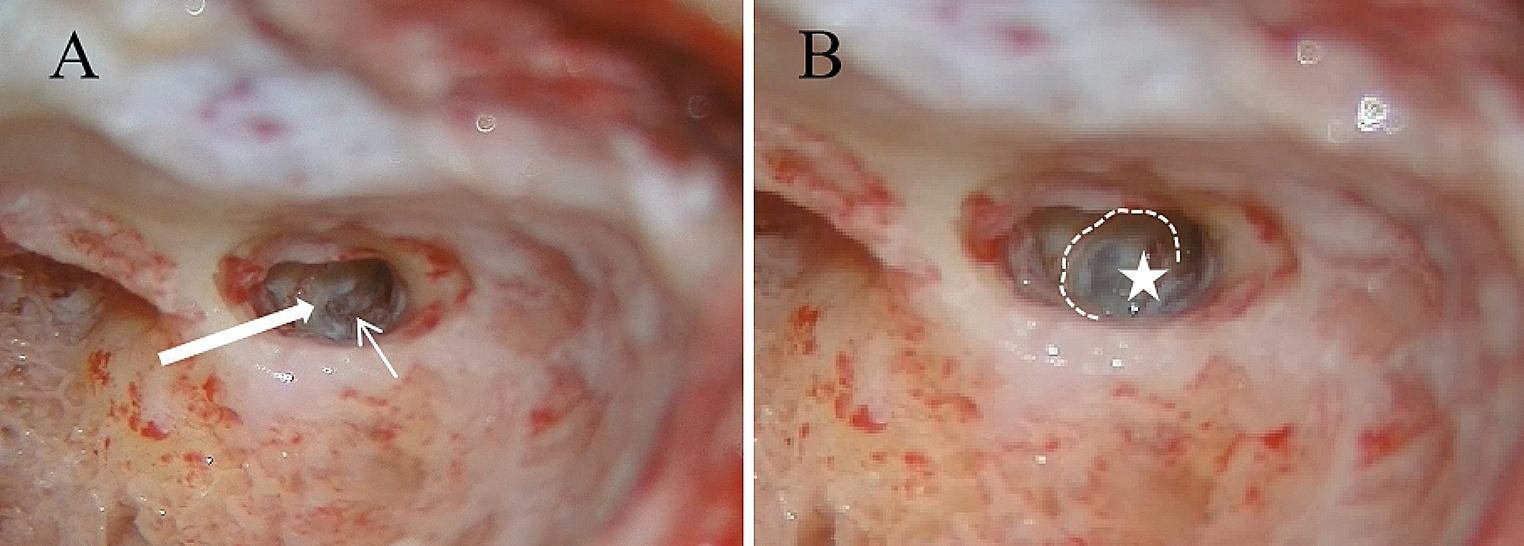
In patients with tympanic membrane atelectasis where we remove the eroded incus or stapes superstructures, ossiculoplasty was not performed at the same time of the tympanoplasty surgery. In these patients an ossicular chain reconstruction using a TORP or PORP through endoscopic ossiculoplasty was scheduled 1 year after surgery (Fig. 4).
Fig. 4
Ossicular chain reconstruction using PORP. Ossiculoplasty with PORP in secondary planned surgery. The patient previously underwent tympanoplasty for chronic otitis media with atelectasis, during which the eroded incus was removed. Stapes superstructures were intact, and the footplate was present and mobile. The prosthesis is first placed with the hollow portion on the stapes head and then positioned under the TM in the correct position
The primary advantages of EES lie in its excellent visualization of middle ear structures and its ability to explore structures around corners. Several anatomical and physiological concepts related to the development of Adhesive Otitis Media (AtOM) due to middle ear dysventilation align with the advantages offered by ESS. The blockage of ventilation routes by middle ear folds can contribute to epitympanic dysventilation and tympanic membrane retraction [12,13,14,15,16,17,18]. Therefore, it's crucial during surgery to ensure proper intraoperative visualization and the removal of these folds that obstruct airflow (Fig. 3). According to Marchioni et al. [24], the endoscopic procedure facilitates improved visualization and removal of blockages in the isthmus and the complete sectioning of the tensor fold, thereby creating a well-ventilated epitympanic cavity. The authors advocate that these endoscopic interventions, focusing on opening blocked airways while preserving the mastoid, could play a vital role in preventing a recurrence of attic retraction.
Despite offering excellent visualization of middle ear structures and recesses, the endoscopic approach has some potential limitations. These include the challenge of single-handed work, the absence of a stereoscopic view, and a potentially steep surgical learning curve. Additionally, the need for frequent endoscope cleaning due to blood or bone dust in the surgical field poses risks, including potential injury to middle ear structures during manipulation of the tympanic membrane adhered to the ossicular chain [14,15,16,17,18,19].
Furthermore, when compared to microscopic surgery, EES demonstrates less effective management of surgical complications, such as trauma to vital structures [15,16,17,18]. These factors collectively contribute to the relatively limited role played by exclusive Endoscopic Ear Surgery (EES) in comparison to conventional Microscopic Ear Surgery (MES).
留言 (0)