
記住我








A community-based cross-sectional study was conducted from May 30 to July 29, 2022, in Kena District, Konso Zone, Southern Ethiopia. The administrative town of Kena Woreda is Fasha, which is located 605 km south of Addis Ababa, the capital city of Ethiopia, and 15 km west of Karat, the town of Konso Zone. In Kena Woreda, there were 11 kebeles, 4 health centres, and 11 health posts. According to Kena Woreda Health Office statistics, the total population of Kena District was estimated to be 82,019, of which 40,189 (49%) are males, 41,830 (51%) are females, and 41% are reproductive-age women [23].
Source populationAll husbands who had resided in Kena woreda for a minimum of six months prior to the study.
Study populationAll husbands who had infants less than 12 months old and who were residents of the chosen kebeles in Kena woreda.
Inclusion and exclusion criteriaInclusion criteriaAll husbands who had infants less than 12 months old were included.
Exclusion criteriaAll husbands who had infants less than 12 months old but who did not stay together with their wives during pregnancy or the birth of their child and were critically ill during the data collection period were excluded.
Sample size calculationThe sample size for the first objective was determined using the single population proportion formula by considering the following assumptions: 95% confidence interval, a 5% margin of error (d), and the proportion of males who participated in BPCRP in Debre Berhan town, Ethiopia, was 51.4% [20], considering a 10% non-response rate. The final sample size was 422.
The sample size for the second objective was calculated using Epi Info version 7.2, with a 95% confidence interval and 80% power. A variable that measures knowledge of at least one danger sign during puerperium (P = 25.8% and OR = 1.8) [18] would give a larger sample size. Considering a non-response rate of 10%, the final sample size was determined to be 499 participants (Table 1). Based on this, the objective with the largest sample size was taken.
Table 1 Sample size calculation for the second objective in BPCR, Kena District, South EthiopiaSampling procedureThere are eleven kebeles in Kena District. A lottery method was used to select five kebeles. The Woreda Health Bureau estimated the number of mothers with children under 12 months old. The calculated sample size for each selected kebeles was distributed proportionally based on its population size, as determined from available information.
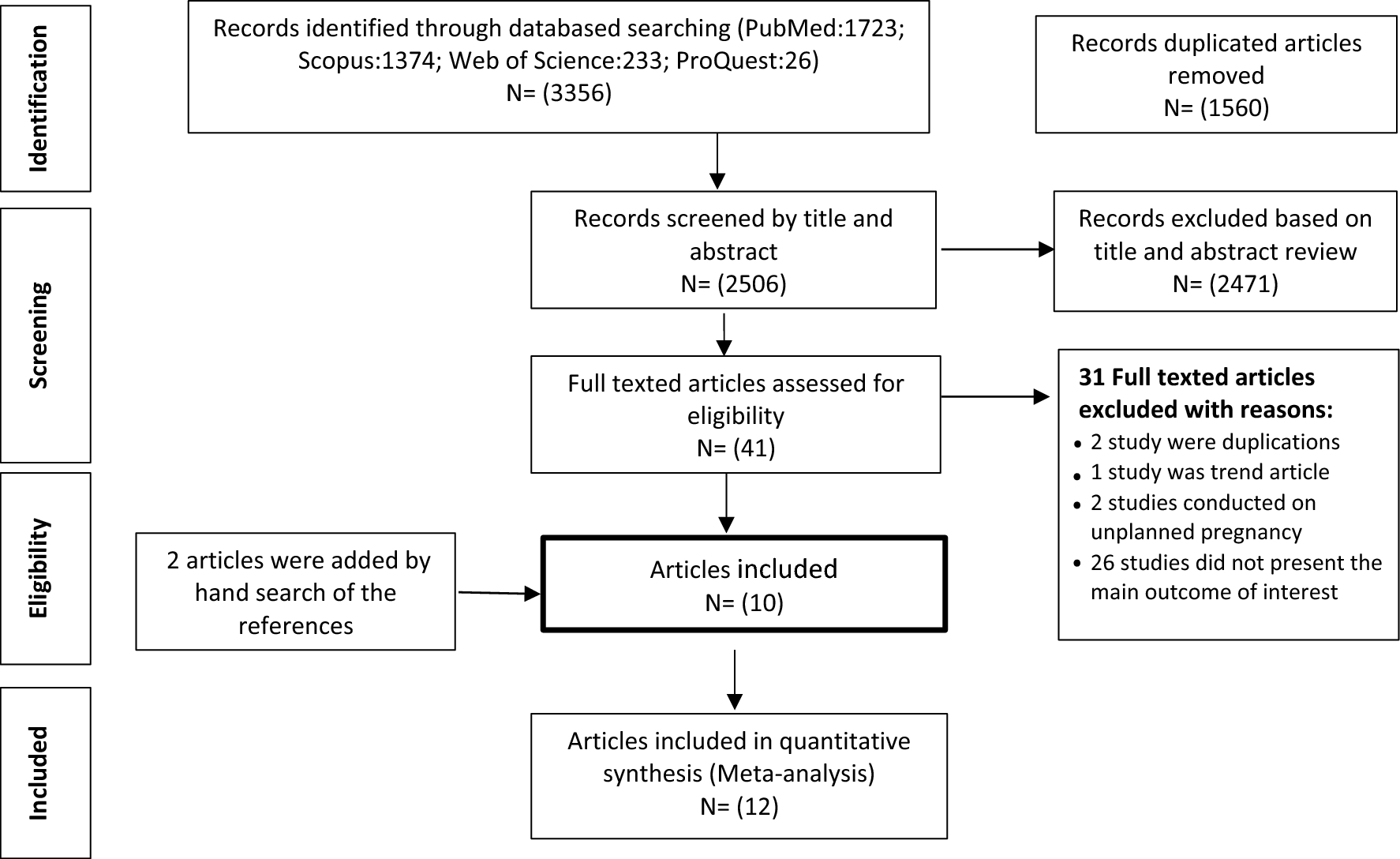
A sampling frame containing a list of wives who had given birth in the last 12 months was obtained from the health posts, where birth information was available. The list of wives who had given birth in the last 12 months was identified, and each was assigned a unique identifier. Then, the husbands of the wives who had given birth during the previous year were selected for interviews using a simple random selection technique generated by a computer. Three follow-up visits were conducted for husbands who were not available during the initial appointment (Fig. 1).
Fig. 1
Schematic presentation of husbands' responses in BPCR in Kena District, South Ethiopia
Data collection tools and proceduresData were collected by two midwives holding bachelor's degrees and two midwives with diplomas. The data collection process was supervised by two professionals with bachelor's degrees in public health. An interviewer-administered structured questionnaire, adapted from survey tools developed by the Johns Hopkins Programme for International Education in Gynaecology and Obstetrics within Maternal and Neonatal Health Programmes [5] as well as other pertinent articles [18, 20], was used. Face-to-face interviews were conducted at the participant’s home.
One-day training was provided to both data collectors and supervisors to familiarise them with the objectives and data collection procedures. A pretest was carried out on 5% (24) of the husbands at Borkara Kebeles. Following the pretest, the questionnaire was thoroughly reviewed and refined, leading to adjustments in its logical flow, skip patterns, and any unclear wording. The interview duration was also fixed, ranging from 20 to 30 minutes.
On a daily basis, the principal investigator and the supervisors oversaw the data collectors and made necessary adjustments to the data collection process. Subsequently, the collected data was uploaded daily to ensure accuracy and consistency.
Study variablesDependent variableHusband response to birth preparedness and complication readiness.
Independent variableSocio-demographic and economic related factors: age, residence, educational status, occupation, and monthly income.
Obstetric-related factors: ANC, number of children, place of last delivery, source of information on problems during pregnancy, childbirth, and post-partum period.
Health services-related factors: nearest health facility, mode of transportation to the health facility, distance from the health facility, and attitude towards the service given.
Operational definitionGood response for BPCR: Individuals who respond to at least five components out of the ten parameters of BPCR [17] are considered to have good responses.
Poor response for BPCR: Individuals who respond to fewer than five components out of the ten parameters of BPCR [17] are considered to have poor responses.
General Knowledge of Key Danger Signs: Individuals who correctly identify five or more key danger signs during pregnancy, delivery, and the postnatal period out of the total ten key danger signs are deemed knowledgeable [20].
Knowledge of Key Danger Signs During Pregnancy: A husband is deemed knowledgeable if he spontaneously lists all three key danger signs during pregnancy, including vaginal bleeding, blurred vision, and swollen hands or face [24].
Knowledge of Key Danger Signs During Labor: A husband is considered knowledgeable if he spontaneously identifies all four key danger signs of labor, such as severe vaginal bleeding, convulsions, prolonged labor, and retained placenta; otherwise, he is deemed not knowledgeable [24].
Knowledge of Key Danger Signs During Postpartum: A husband is considered knowledgeable if he spontaneously mentions all three key danger signs of the postpartum period, such as severe vaginal bleeding, foul-smelling discharge, and high fever; otherwise, he is classified as not knowledgeable [24].
Data quality controlTo ensure the accuracy and appropriateness of the questionnaire, a comprehensive process was employed. First, the questionnaire was drafted in English and then expertly translated into Amharic. To further guarantee accuracy, the Amharic version was translated back into English by the same language experts. A pretest was conducted on 25 husbands in Borkara Kebeles, a community outside the study area, before applying to the main study. One-day training was provided to both data collectors and supervisors. Cronbach's alpha (a statistical measure of reliability) was calculated to evaluate the questionnaire's internal consistency, resulting in a score of 0.869, indicating good reliability. To ensure data quality and consistency, daily data submission was implemented. The principal investigator and supervisor diligently monitored the data collectors on a daily basis, guaranteeing accuracy and consistency in data collection.
Data Processing and analysisAfter completion of data collection, the data were coded, entered into the computer through Epi Data version 4.6 data entry forms, and then transferred to SPSS version 25 software for data cleaning and analysis. Percentages, frequencies, median, and interquartile range were used for descriptive purposes.
Bivariable logistic regression was employed to identify the associations between the BPCR and independent variables. First, a variable with a P-value less than 0.25 was used to select potential variables for the multivariable logistic regression. Then, before doing the final multivariable analysis, multicollinearity was examined using the variance inflation factor and revealed no association between each other. The model goodness-of-fit was checked using Hosmer–Lemeshow, which was insignificant (p-value = 0.57). A statistically significant result was declared using a p-value less than 0.05 with a 95% confidence interval and an adjusted odd ratio.
留言 (0)