
記住我
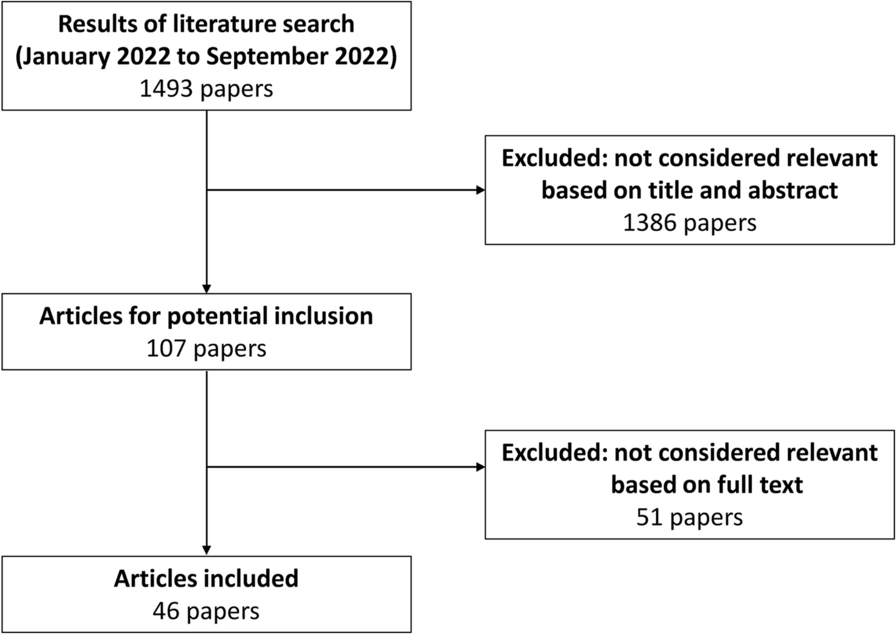
A total of 482 centers engaged in this investigative survey. Of 1973 registered patients eligible for the PMS study, 1387 provided informed consent, and case report forms were not collected from 6 patients. Thereby, 1381 patients were analyzed for safety and effectiveness. Of these, 1271 (92.0%) patients received a VKA (Fig. 1). INR measurements were obtained before initial administration of 4F-PCC in 1202 patients, of which 215 (17.9%) had INR < 2.0 group and 987 (82.1%) had INR ≥ 2.0.
Fig. 1
Patient disposition and analysis sets. INR international normalized ratio, VKA vitamin K antagonist
Patient Characteristics at BaselineThe patient characteristics of overall cohort have been previously published [20]. There were 119 male patients and 96 female patients in the INR < 2.0 group, and 617 male patients and 370 female patients in the INR ≥ 2.0 group. For most baseline variables, age (74.0 vs 74.0 years), body mass index (22.1 kg/m2 vs 21.9 kg/m2), and the ratio of inpatients (90.2% vs 88.7%) were similar between both groups (Table 1). Notably, the proportion of elderly patients was high in both groups, with those aged ≥ 80 years accounting for 39.5% in the INR < 2.0 group and 40.3% in the INR > 2.0 group.
Table 1 Baseline patient characteristicsThis study identified nine pediatric patients (under 15 years), all of whom had an INR ≥ 2.0, and there were no pediatric patients with an INR < 2.0.
The average INR values (minimum, maximum) were 1.72 (0.92, 1.99) in the INR < 2.0 group and 2.95 (2.00, 27.11) in the INR ≥ 2.0 group. Of the INR < 2.0 group, 36.3% had an INR of < 1.6.
Both groups showed a comparable ranking of reasons for VKA use, with AF (46.0% vs 48.8%; INR < 2.0 vs ≥ 2.0) as the leading cause and valvular heart disease (21.4% vs 15.9%) as the second most frequent.
Dose of 4F-PCCThe average doses of 4F-PCC were 24.5 IU/kg (INR < 2.0 group) and 29.2 IU/kg (INR ≥ 2.0 group) (Table 2).
Table 2 Summary of 4F-PCC administrationThe distribution of dose of 4F-PCC was also similar between both groups in the INR < 2.0 and ≥ 2.0. The most commonly used dose ranges were 25–35 IU/kg, followed by 20–25 IU/kg. The use of < 20 IU/kg was more frequent in the INR < 2.0 group at 18.6% compared to 7.1% in the INR ≥ 2.0 group.
Reason for Administration of 4F-PCCBoth INR < 2.0 and ≥ 2.0 groups showed a comparable ranking of reasons for the administration of 4F-PCC, with ICH (67.0% vs 59.5%), inclusive of non-traumatic ICH (27.4% vs 29.7%), and traumatic ICH (20.0% vs 17.1%) as the leading causes, followed by abdominal and cardiovascular surgery/intervention (5.6% and 7.4% vs 5.7% and 4.5%) (Table 2). Gastrointestinal (GI) bleeding was more frequent in the INR ≥ 2.0 group (7.5%) compared to the INR < 2.0 group (0.9%). Additionally, INR prolongation was observed in 13 cases (1.3%) in the INR ≥ 2.0 group but not in the INR < 2.0 group.
The rates of concomitant vitamin K and blood transfusion were similar between both groups (71.6% and 49.3% vs 72.5% and 40.0%), with over 99% of the Vitamin K being administered intravenously.
EffectivenessThe hemostatic effectiveness showed similar achievement between both INR < 2.0 and ≥ 2.0 groups (82.3% and 86.7%). Treatment with 4F-PCC significantly reduced INR (p < 0.001); median (minimum, maximum) INRs at baseline and post-administration were 1.75 (0.96, 1.99) and 1.18 (0.45, 2.30), respectively, in the INR < 2.0 group (Fig. 2a) and 2.98 (2.00, 27.11) and 1.22 (0.89, 6.61), respectively, in the INR ≥ 2.0 group (Fig. 2b). At post-administration, the percentage of patients achieving INR ≤ 1.3 was 78.9% in the INR < 2.0 group and 64.8% in the INR ≥ 2.0 group.
Fig. 2
INR before and after initial administration of 4F-PCC. Baseline (before initial administration of 4F-PCC) INR < 2.0 (a), INR ≥ 2.0 (b). INR between before and after initial administration of 4F-PCC was analyzed using a paired t test. INR prothrombin time—international normalized ratio, 4F-PCC four prothrombin complex concentrate
Resumption of Anticoagulant TherapyThe proportion of anticoagulant resumption after ICH was lower than after any bleeding, indicating a similar pattern in both groups: 61.8% vs 67.0% in INR < 2 group; 56.3% vs 62.9% in INR ≥ 2.0 group (Table 3). The date to resume anticoagulation varied across both groups and regardless of the type of bleeding events.
Table 3 Summary of anticoagulant therapy resumptionSafety and Characteristics of TEEThe reporting rate of ADR was similar in both groups. In the INR < 2.0 group, there was one case (0.5%) of shock and four cases of TEE (1.9%). Conversely, in the INR ≥ 2.0 group, there were 11 instances of TEE (1.1%) (Table 4).
Table 4 Incidence of ADRsThe characteristics of the TEEs are also presented in Table 4. The majority of TEEs were stroke, with 3 out of 4 cases occurring in the INR < 2 group and all 11 cases in the INR ≥ 2 group. Among other TEE events, there was one case of deep vein thrombosis in the INR < 2 group, while in the INR ≥ 2 group, there were also five cases of intracardiac thrombus, and one case each of pulmonary embolism, arterial embolism, and renal infarction, some of which overlapped with reports of stroke.
Upon investigating the details of the four cases of TEEs in the INR < 2.0 group revealed that three cases had a baseline INR < 1.6. Additionally, all four cases received ≥ 20 IU/kg, while no TEEs occurred in patients given < 20 IU/kg. Furthermore, in two of the four cases, anticoagulant therapy had not been resumed, and in one case, it was resumed after 16 days.
留言 (0)